Compliance Corner: Medicare’s Modifier 59 Expansion

The Centers for Medicare & Medicaid Services (CMS) began the National Correct Coding Initiative (CCI) edits as an initiative to promote correct coding by providers and to prevent Medicare payment for improperly reported services. The CCI program consists of automated edits that are part of the claims processing systems deployed by the Medicare Administrative Contractors (MACs). Specifically, the CCI edits contain pairs of Healthcare Common Procedure Coding System (HCPCS) codes (i.e., code pairs) that generally should not be billed together by a provider for a patient on the same date of service. All code pairs are arranged in two columns. Column 1 contains the primary code and column 2 the secondary code or service format. The column 2 code is generally not payable with the column 1 code.
Under certain circumstances, a provider may bill the column 2 service in a CCI code pair by including a modifier on the claim that would bypass the edit and allow both services to be paid. A modifier is a two-digit code that further describes the service performed. While the CCI edits contain 35 different modifiers that may be used to bypass the CCI edits, modifier 59 is the most frequently reported.
Modifier 59 is used to indicate that a provider performed a distinct procedure or service for a patient on the same day as another procedure or service. It is attached to the secondary, additional, or lesser service in the code pair.1 Pursuant to the Medicare Claims Processing Manual and the 2014 Current Procedural Manual, modifier 59 may represent a:
- Different session,
- Different procedure or surgery,
- Different anatomical site or organ system,
- Separate incision or excision,
- Separate lesion, or a
- Separate injury (or area of injury in extensive injuries).2
When modifier 59 is used, pursuant to the Medicare Claims Processing Manual, the provider’s documentation must demonstrate that the service was distinct from other services performed that day.3 Section 1833(e) of the Social Security Act requires that providers furnish “such information as may be necessary in order to determine the amounts due” in order to receive Medicare payment.
For example, the family of HCPCS codes 22520-22522 describes percutaneous vertebroplasty. Current Procedural Terminology (CPT®) code 22520 identifies percutaneous vertebroplasty of a single thoracic vertebral body. CPT code 22521 describes percutaneous vertebroplasty of a single lumbar vertebral body. CPT code 22522 is an add-on code for percutaneous vertebroplasty of each additional thoracic or lumbar vertebral body. If a physician performs percutaneous vertebroplasty on contiguous vertebral bodies such as T12 and L1, only one primary procedure code, the one for the first procedure, may be reported. The procedure on the second vertebral body should be reported with CPT code 22522. If a physician performs the procedure at T10 and L4, the physician may report CPT codes 22520 and 22521.4 Currently modifier 59 would be used to indicate the second procedure is distinct since it was performed on a separate organ/structure. As of January 1, 2015 modifier XS (separate structure) would also be correct. In both cases, the physician’s documentation must clearly indicate that the procedures were on different distinct structures.
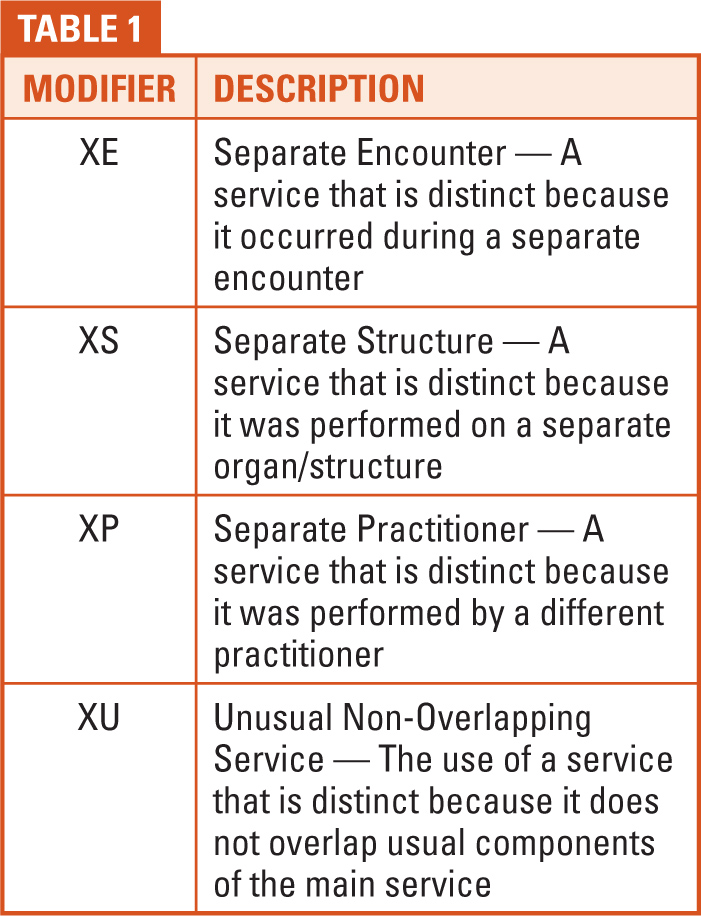
The Office of the Inspector General (OIG) and CMS have longstanding concerns about potential fraud and abuse related to the use of modifier 59. As a result, CMS released on August 15, 2014 four new modifiers for coders and billers to choose from starting January 1, 2015 when reporting services to Medicare that would have previously been reported with modifier 59. The new modifiers and their descriptors are shown in Table 1.
Although the new modifiers will take effect, January 1, 2015, CMS stated in the Transmittal that modifier 59 will remain active. However, the agency may “selectively require” use of one of the new modifiers for certain codes that have a higher risk of incorrect billing.5
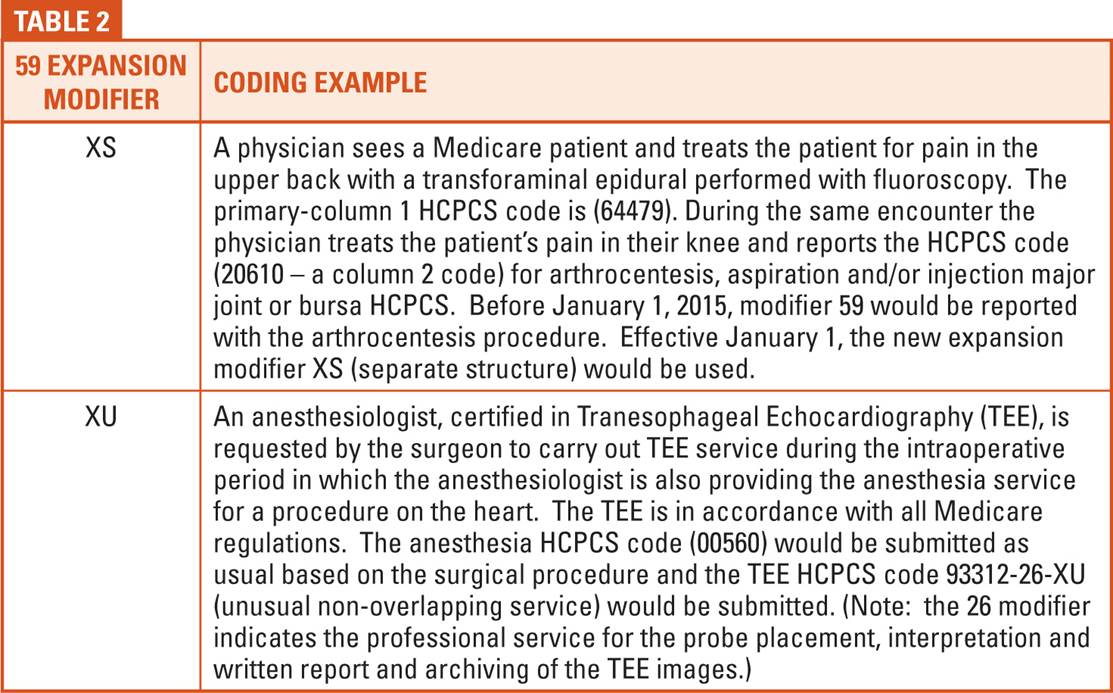
Table 2 sets forth a few additional scenarios in which the new modifiers might add clarity to why both services/procedures were performed.
Modifier 59 (distinct procedural service) has never been well understood by physicians, coders or billers. Often it is used by a coder or a biller as a default modifier to get a previously denied service reimbursed. In its announcement regarding the new HCPCS modifiers, CMS cites high rates of misuse as a factor for the change, noting that the 2013 Comprehensive Error Rate Testing (CERT) program report projected $770 million in improper payments involving modifier 59. A November 2005 OIG report had previously found that forty percent of code pairs billed with modifier 59 in FY 2003 did not meet program requirements, resulting in $59 million in improper payments.6
Opinions on whether the new 59 modifier expansion effort to clarify distinct procedural services will reduce or increase denials are about 50-50. Many industry experts are waiting for additional clarification from CMS or the MACs about exactly how to use the new subset modifiers. Surprisingly, CMS stated in the transmittal that either 59 or a subset modifier may be payable on a claim line, though it goes on to say that “a rapid migration of providers to the more selective modifiers is encouraged.”7 In addition, as of yet private payers have not indicated what, if anything, they will implement or accept regarding the four expansion modifiers.
Each January, CMS releases corresponding CCI guidance specific to each range of HCPCS codes. Many experts believe that the 2015 guidance manual will require a major rewrite to correspond to CMS statement that particular code pairs in CCI may be identified as payable only with one of the new X modifiers. Currently, CCI edits state only that a modifier is or is not allowed with the edit without guidance on specific modifiers. Providers, coders and billers should stay alert to additional guidance from CMS or their MAC as the effective date grows closer.
1 “Medicare Claims Processing Manual,” Chapter 23, section 20.9, http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/clm104c23.pdf
2 Ibid.
3 Medicare Claims Processing Manual,” Chapter 12, section 30, http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/clm104c12.pdf
4 “National Correct Coding Policy Manual for Medicare Part B Carriers,” Chapter IV Surgery: Musculoskeletal System CPT Codes 20000-29999, January 1, 2014, http://www.cms.gov/Medicare/Coding/NationalCorrectCodInitEd/index.html
5 “CMS Manual System, Pub 100-02 One-Time Notification, Transmittal 1422, August 15, 2014, http://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/Downloads/R1422OTN.pdf
6 Office of Inspector General, “Use Of Modifier 59 To Bypass Medicare’s National Correct Coding Initiative Edits” November 2005, OEI-03-02-00771, http://oig.hhs.gov/oei/reports/oei-03-02-00771.pdf
7 “CMS Manual System, Pub 100-02 One-Time Notification, Transmittal 1422, August 15, 2014, http://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/Downloads/R1422OTN.pdf