eAlerts
-
MACRA’s Physician-Focused Alternative Payment Model Options: A Multispecialty Perspective
Asa C. Lockhart, MD, MBA
Co-Founder and Principal, Golden Caduceus Consultants, Seabrook, TXThe Medicare Access and CHIP Reauthorization Act (MACRA), which replaced the perennial Sustainable Growth Rate (SGR) formula, created two options for compliance. The first path, which does not require assumption of insurance risks, is the Merit-Based Incentive Payment System (MIPS) that consolidated existing quality programs and added clinical practice improvement. The other fork in the new highway is the Alternative Payment Model (APM), with one subgroup variant being the Physician-Focused (PF-APM), in which the physician accepts some level of risk for services and expenses over which they have some control. Another subgroup variant is the Hospital-Focused (HF-APM). This article focuses on PF-APMs with an emphasis on potential multispecialty models that may provide subtle opportunities or be developed by others in the community where anesthesia may play a role. While physicians may have a wide range of experience with some MIPS elements, few physicians have any idea how APMs might apply to their practice.
 Our current system is oriented toward intervention and what is possible; emerging models emphasize prevention and experientially-based minimization of avoidable complications. Modeling focuses on balancing optimization of outcomes, costs and patient satisfaction versus fragmented silos of care (e.g., particular physicians or specialties). Disconnects between the consumer (patient) and the producer (professionals) are barriers to balancing costs and utility. The current system does not value or anticipate the questions of how often it meets expectations, at what costs and relative risks. Additionally, the patient has no affirmative responsibility to optimize their personal health. And finally, the system itself is a barrier.
Our current system is oriented toward intervention and what is possible; emerging models emphasize prevention and experientially-based minimization of avoidable complications. Modeling focuses on balancing optimization of outcomes, costs and patient satisfaction versus fragmented silos of care (e.g., particular physicians or specialties). Disconnects between the consumer (patient) and the producer (professionals) are barriers to balancing costs and utility. The current system does not value or anticipate the questions of how often it meets expectations, at what costs and relative risks. Additionally, the patient has no affirmative responsibility to optimize their personal health. And finally, the system itself is a barrier.Barriers to Redesign
Existing models may not address barriers to redesigning services that may provide higher value to healthcare. To innovate, one must have the latitude to reallocate precious but limited resources and have space to make the transition. Two commonly mentioned barriers are either no or inadequate payment for many high-value services and transitional financial risk for a different mix of services despite reduced costs to society. Patients may benefit from enhanced personal time in an alternative model or pursue lower cost options with improved or neutral outcomes. Yet we are not paid to take the time to counsel patients on lifestyle or various options available to them that are time-intensive or require relational databases. Physicians are best positioned to evaluate alternative delivery systems and optimize cost delivery settings and different combinations of services and providers. But that takes time and requires support and resources (human and financial capital) not currently available. It also takes an alignment of incentives that focus more on outcome, utility and coordination rather than component production and what is merely possible. A transition from the current model to emerging models still requires keeping the doors open! As current transactional practice revenue decreases with the delivery of fewer or lower cost services, a transitional strategy will be necessary to shield operating losses, as changes will not be proportional and may even be higher in a temporarily dual system.
No or inadequate payment is a barrier to both Medicare and private health plans for high-value services that would benefit patients and help reduce avoidable spending. For example, responding to a phone call about a symptom or problem might help patients avoid a more expensive ER visit. There is no recognition of the value of coordination of care between primary care physicians and specialists for the time saved by avoiding duplicate tests or conflicting medications, or for facilitating discharge planning in emergency departments to enable safe discharge without hospitalization. A proactive, early-stage telephone call might optimize preventive care and lower comorbidities in high-risk patients. Patients, especially deconditioned patients, would benefit from prehabilitation, but there is little support for developing this intervention. Smoking cessation reduces respiratory complications and length of stay as well as improvements in wound dehiscence. Current paradigms do not recognize these benefits. However, a well-designed APM would leverage these opportunities.
Financial penalties for delivering a different mix of services pose transitional risks to physicians in several ways. As their health improves, patients require fewer services or avoid developing a disease. They experience fewer complications and comorbidities requiring intervention. However, despite these improvements, practice overhead does not decrease; rent and utilities are not pegged to quality of care or resource utilization.Most APM savings do not come from physician payments; savings can be realized without financial targeting or implicit penalization of physician practices for delivering a societal goal. With healthier patients, physician practices would receive less income under current methodologies. This is the essential problem that must be addressed if we are to make substantial progress as APM options are developed.
What are the prerequisites to overcoming these barriers to successfully create new options? The Center for Healthcare Quality and Payment Reform (CHQPR) has identified three characteristics for enabling change:
- Flexibility in Care Delivery: the APM must provide enough innovative flexibility and patient-centric focus to deliver a mix of services that makes sense but is not covered within today’s payment methodologies to provide new paths to efficiency and effectiveness.
- Adequacy and Predictability of Payment: it is essential that financial resources be available to start the process and that there is confidence that the return on investment (ROI) will be there. The fear is that our success will be co-opted. Rules of engagement must deliver adequate and predictable resources to allow physicians to create alternative structures to identify high-quality service opportunities and address both start-up and transitional financial risk to physicians. Exposure must be risk-adjusted to recover the investment yet be within an acceptable financial risk corridor for small business medical practices.
- Accountability for Costs and Quality Under Physicians’ Control: program design must assure non-provider stakeholders (patients and payers) that outlays will be controlled or reduced with an implicit assumption that quality will be maintained or improved. The beauty of PF-APMs is that individual physicians should only be at risk for those aspects of spending and quality they can materially control or influence.
Examples of Potential Models
A Guide to Physician-Focused Alternative Payment Models, prepared by the American Medical Association (AMA) and the CHQPR, identifies seven potential models. Since this is an emerging concept with no other resources that synthesize the material as well as this publication, the following excerpts/paraphrases in quotes are from that comprehensive document, followed by examples to stimulate thought on how these models could benefit practices and communities.“APM #1: Payment for High-Value Services with physician payment for desirable services not currently billable enabling avoidance of other, more expensive services...physician bills and paid for time and resources needed to apply appropriate use criteria and engage in an education/shared decision-making process with patients to determine the most appropriate diagnostic tests.... In contrast to typical shared savings programs, physician payments would not be explicitly tied to how much money that practice saved. Instead, the physician practice would be paid adequately to deliver appropriate services, and the payer saves money by spending less on avoidable services.”
This could be a component of an early-stage perioperative surgical home (PSH) (e.g., preoperative testing protocols, prehabilitation, smoking cessation).
“APM #2: Condition-Based Payment for Physician’s Services...physician flexibility to use the most appropriate diagnostic or treatment option for a patient’s condition without reducing the operating margins of the physician’s practice...flexibility to use the payments for whatever combination of services were most effective—office visits, phone calls, emails.”
Monthly payments targeted to chronic conditions replace evaluation and management code limitations. Seamless transitions or smoking cessation achieved during PSH appeals to primary care physicians (PCPs) with global risk with enhanced management of COPD patients.
“APM #3: Multi-Physician Bundled Payment (BP)...the goal is to give multiple physicians providing services to the same patient flexibility and resources needed to redesign their services in coordinated ways to improve quality and reduce the costs of diagnosis or treatment.... Patients benefit as physicians delivering their care work together in more coordinated ways with additional resources and/or flexibility under the bundled payment to deliver different types or combinations of services not currently provided. Payers benefit because new payments enable physicians to deliver care more efficiently, order fewer or lower-cost services from other providers, and/or reduce avoidable complications. Physician practices benefit from the resources and flexibility to deliver optimal services and coordinated services agnostic to current revenue flow risks to the practices.”
This model has a very high potential and likelihood for anesthesiologists since it offers major benefits and aligns incentives for all stakeholders to coordinate care by virtue of shared risks and rewards. This model would allow acceptance of risks for professional services, especially in circumstances where the facility partner is unable or unwilling to participate.
“APM #4: Physician-Facility Procedure Bundle...the goal is to incentivize physicians to choose the most appropriate facility to deliver particular procedures and to work with the facility to improve efficiency and quality.... Patient benefits from receiving high quality care at the lowest-cost facility with coordinated and efficient care.... Payer benefits because the Alternative Payment Entity (APE) could accept a lower payment for the bundle than the total separate amounts under current payment systems. Physician practices benefit by using the BP to cover the costs of services not currently billable or inadequate, and by receiving compensation for innovations that reduce costs at the facility.”This model has a very high potential and likelihood for participation by anesthesiologists since it offers major benefits and aligns management incentives between stakeholders but carries the utility risk of demand for certain services (e.g., GI, cataract). The marked variability in hospital charges will be a significant driver with an opportunity to engage payers. Since anesthesiologists cover multiple sites, they are in a unique position to help select the most efficient or progressive facilities (e.g., stable facilities with good policies and procedures versus lower performing options).
“APM #5: Warrantied Payment for Physician Services...the goal is adequate physician payment and flexibility to redesign care to prevent complications with reduced spending needed to treat them.... Contrasting penalties that reduce payments for complications, this approach provides greater upfront resources to redesign care for reduced complications. With the cost of treating some complications built into the warrantied payment amount, the physician is not financially penalized when a small number of complications occur yet rewarded for eliminating most or all complications.”
This could be a potential variant of a monetization strategy for a PSH.
“APM #6: Episode Payment for a Procedure...the goal is to give physicians and other providers the ability to deliver comprehensive care during and after particular procedures or treatments in coordinated, efficient ways...all of the costs involved in a procedure encompassing inpatient, rehabilitation services and treating any post-operative complications. The payment amount would be risk-adjusted, anticipating more or less inpatient or post-acute care. Payments would be adjusted based on quality and outcome measures.”
This essentially takes Models 4 and 5 and adds the post-discharge management and readmission risk components. While optimally a later, more mature option after experience in Models 4 and 5, market and political pressures may make this the initial option. The Comprehensive Care for Joint Replacement (CJR) Model added hip and femur fractures as a proposed rule APM in August.“APM #7: Condition-Based Payment...gives physicians and other providers delivering care for acute or chronic conditions flexibility and accountability to deliver the most appropriate treatment for the patient’s condition in a coordinated, efficient, high-quality manner.”
An example was Condition-Based Payment for Post-Acute Care Following a Hospitalization for spine surgery. This model may be a separate initiative, perhaps with different provider groups, as either an early stand-alone or as an independent but complementary part of Model 3 or 4, but an integral part of Model 6. The post-discharge management of a PSH patient could be a standalone approach in some circumstances. In the procedural arena, I do not see this as a long-term option and would predict a rapid integration with one of the other models.
Conclusion
We are in the interim final rule phase of rulemaking, and the American Society of Anesthesiologists and AMA are diligently evaluating options to preserve your future. The multiple system options may be payer-designed, facility-designed or physician-designed. Close your eyes and make a guess; of those three options, which avenue is most likely to provide an optimal system that treats our colleagues and our patients in the most equitable manner? The above options will evolve with both the final rulemaking and system adaptation.
I would like to acknowledge briefing materials contained in the publication A Guide to Physician-Focused Alternative Payment Models jointly produced by the AMA and the CHQPR that provided the generous excerpts, direction and resources for this article. I would like to thank Sandra Marks (AMA) and Harold Miller (CHQPR) for their copyright permission in general, allowed use of generous excerpts and edits in particular. For a deeper understanding of how you can take control of your future, this excellent resource may be accessed at: www.ama-assn.org/ama/pub/advocacy/topics/medicare-alternative-payments-models.page.
Asa C. Lockhart, MD, MBA is Co-Founder and Principal of Golden Caduceus Consultants, an anesthesiology consulting firm in Seabrook, TX. Over the past 16 years, GCC has developed stabilization strategies for more than 185 hospitals and/or anesthesia groups and departments in 37 states. In addition to his consulting work, Dr. Lockhart had an active anesthesia practice in Tyler, TX and has an MBA with an emphasis in healthcare that brings validity and insight to the challenges facing many anesthesia groups and hospitals. Dr. Lockhart is the founder and course director for the ASA Certificate in Business Administration Course created by the ASA Committee on Practice Management. He was also a member of the ASA Committee on Future Models of Anesthesia Practice and has served as president and treasurer of the Texas Society of Anesthesiologists. He serves on the AMA Council on Medical Services, which develops healthcare policy options for consideration by the AMA House of Delegates, and is a vice-chair with the National Physicians’ Council for Health Care Policy. He can be reached at (903) 521-6728 and aclhart@goldencaduceusconsultants.com. -
Anesthesia’s Transition to Value-Based Care
The fate of the Affordable Care Act (ACA) remains unclear following the outcome of the presidential and Congressional elections (with president-elect Trump stating his desire and Republicans in both House and Senate showing their zeal to repeal the ACA, as discussed in our final eAlert of 2016). The bipartisan Medicare Access and CHIP Reauthorization Act (MACRA) and the healthcare sector’s transition to value-based care are expected to remain intact, however. As Andy Slavitt, acting administrator of the Centers for Medicare and Medicaid Services (CMS), advises eligible clinicians, move ahead as planned with your participation in the Quality Payment Program (QPP).
Considering the QPP’s newness and complexity, many clinicians are likely to feel some uncertainty regarding what they must report, how they must report it and how they will fare under the new Medicare payment system. According to a national survey of more than 17,000 physicians by The Physicians Foundation reported in September, only 20 percent of respondents indicated they were somewhat or very familiar with the system.1
To assist in this first performance year, Kathryn Hickner, Esq. returns to this issue with an overview of the QPP and its two tracks, the Merit-Based Incentive Payment System (MIPS) and Advanced Alternative Payment Models (APMs). Ms. Hickner encourages anesthesia providers to “promptly and proactively develop a strategy to thrive under MACRA and the QPP,” noting that CMS expects the majority of eligible clinicians to participate in MIPS in this initial performance year and anticipates that 90 percent will receive a neutral or positive payment adjustment. To us, that looks like a clear sign that the QPP can be met with confidence.
Although most eligible clinicians are expected to participate in MIPS in the QPP’s first year, CMS expects clinicians to eventually participate in APMs, so it is not too soon for those of you who are not already in APMs to explore the possibilities. Anesthesia consultant Asa C. Lockhart, MD, MBA takes us on a brief but intriguing journey of some potential options developed by the American Medical Association and the Center for Healthcare Quality and Payment Reform.
An innovative care delivery model that is gaining traction within anesthesiology and with which many of you are already familiar is the perioperative surgical home (PSH). In his sixth in a series of articles on the PSH, Rick Bushnell, MD, MBA discusses how anesthesiologists can parlay the clinical skills they already have to optimize and risk-stratify patients during the preoperative appointment that is a hallmark of the PSH.
Regardless of what happens to it in the next few years, the historic and controversial ACA has left its mark on American healthcare and healthcare payment. According to Maurice Madore, MBA, CPC, chief client officer of Anesthesia Business Consultants, while millions fewer Americans lack healthcare coverage as a result of the ACA, “providers have been forced to restructure how they get paid for services as patients have become responsible for a higher percentage of their healthcare costs.”
Also in this issue:
- Consultant Will Latham, MBA gives us another article on strategic business planning. This time, Mr. Latham probes the ins and outs of the strategic planning retreat, providing practical advice on organizing the event and keeping it on track.
- Frequent contributor Mark F. Weiss, JD discusses the little known “verein” or confederation model, a potential business structure for anesthesia groups interested in forming a larger structure out of existing groups that “frees the organizers from many of the problems encountered in creating alignment.” The verein structure “lowers the barrier of ‘trust to entry,’” Mr. Weiss writes. “It’s far easier to trust in a vision if it doesn’t require giving up your ownership and local control, and becoming liable for someone else’s debts.”
- Jody Locke, MA vice president of anesthesia and pain practice management for ABC, reviews the evolution of the electronic medical record in anesthesia, sheds light on why EMR implementation within the specialty is often fraught with challenges, and offers guidance to anesthesia practices for avoiding some of the obstacles.
We look forward to seeing many of you at the 2017 ASA Practice Management Conference in Grapevine, Texas.With best wishes,
Tony Mira
President and CEO
12016 Survey of America’s Physicians: Practice Patterns & Perspectives, The Physicians Foundation, September 2016. http://www.physiciansfoundation.org/uploads/default/Biennial_Physician_Survey_2016.pdf
-
The MACRA Quality Payment Program Is Here. Are You Ready?
Kathryn Hickner, Esq.
Ulmer & Berne LLP, Cleveland, OHYou have heard of the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) and, most likely, its Quality Payment Program (QPP). But do you really know what it is? Do you know what it means to your practice? Do you know what your practice will need to do to thrive under the QPP? If you haven’t already, you’ll need to develop a firm understanding of the reimbursement landscape under MACRA. The time is now. Ready. Set. Go.
Background and Context
In October 2016, the Centers for Medicare and Medicaid Services (CMS) issued the MACRA final rule with comment period titled “Medicare Program; Merit-Based Incentive Payment System (MIPS) and Alternative Payment Model (APM) Incentive under the Physician Fee Schedule, and Criteria for Physician-Focused Payment Models” (the Final Rule).1
Although it is more than 800 pages long, the MACRA final rule is designed to simplify participation by eligible clinicians. MACRA essentially replaces the old methodology used to determine the Medicare Physician Fee Schedule. This methodology, the Sustainable Growth Rate formula, threatened to impose payment cutbacks for physicians for more than a decade. The QPP aims to reward the provision of high quality and efficient services through a single cohesive system that unifies and replaces several different Medicare payment programs.In 2015, CMS announced its goal of tying 90 percent of traditional Medicare payments to quality or value by 2018.2
The QPP advances these goals and related objectives. More specifically, CMS has clarified that the QPP aims to achieve the following:
- To improve beneficiary outcomes and engage patients through patient-centered policies.
- To enhance clinician experience through flexible and transparent program design and interactions with easy-to-use program tools.
- To increase the availability and adoption of robust Advanced APMs.
- To promote program understanding and maximize participation through customized communication, education, outreach and support that meets the needs of the diversity of physician practices and patients, especially the unique needs of small practices.
- To improve data and information sharing to provide accurate, timely and actionable feedback to clinicians and other stakeholders.
- To ensure operational excellence in program implementation and ongoing development.3
Quality Payment Program
The QPP, which commenced on January 1, 2017 and is anticipated to continue through 2022 and beyond, will result in negative, neutral and positive adjustments to physician compensation. CMS refers to 2017 as a transitional year for the final rule and anticipates a ramp-up period as clinicians adjust to the QPP. Note, however, that, although the reporting periods commence during 2017, physicians will not receive increased reimbursement under the QPP until 2019. For this reason, participation in the QPP should be viewed as a long-term investment.
The QPP provides physicians with the ability to choose from one of two options: (1) the Advanced APMs and (2) the MIPS. It’s important for physicians to understand their options and find the best QPP track for their particular practice.
Advanced Alternative Payment Models
CMS anticipates that up to 120,000 clinicians will participate in the Advanced APM track during the 2017 performance year. Advanced APMs must satisfy certain criteria.
They must:
- Be CMS Innovation Center models, Shared Savings Program tracks or certain federal demonstration programs
- Use certified electronic health record (EHR) technology
- Base payments for services on quality measures comparable to those in MIPS
- Be a Medical Home Model expanded under CMS Innovation Center authority or require participants to bear more than nominal financial risk for losses
As this article is being written, CMS anticipates that the following models will be Advanced APMs for the 2017 performance year:
- Comprehensive End-Stage Renal Disease Care Model (two-sided risk arrangements)
- Comprehensive Primary Care Plus (CPC+)
- Medicare Shared Savings Program, Track 2
- Medicare Shared Savings Program, Track 3
- Next Generation Accountable Care Organization (ACO)
The list of participating Advanced APMs will change over time and updates will be posted on the CMS website.
Note that the QPP does not change the Advanced APMs, but rather, offers additional incentives for sufficiently participating in them. In the event that a practice receives 25 percent of Medicare covered professional services or sees 20 percent of its Medicare patients through an Advanced APM during 2017, then such practice will earn a five percent Medicare incentive payment during 2019.
Merit-Based Incentive Payment System
CMS anticipates that most clinicians will participate in MIPS instead of the Advanced APM track, at least initially. The agency expects up to 500,000 clinicians to participate in MIPS during the 2017 performance year and that 90 percent of eligible clinicians will receive a neutral or positive payment adjustment.
The MIPS track is available not only to physicians but also to physician assistants, nurse practitioners, clinical nurse specialists and certified registered nurse anesthetists who bill more than $30,000 per year to Medicare and provide care to more than 100 Medicare patients per year.
The MIPS track replaces three Medicare programs: (1) the Medicare EHR Incentive Program (Meaningful Use); (2) the Physician Quality Reporting System (PQRS); and (3) the Value-Based Payment Modifier. Accordingly, the requirements for participating in MIPS are familiar to many physicians.
Performance Categories
For 2017, there are four weighted performance categories:
- Quality (which replaces the PQRS and carries a 60 percent weight)
- Improvement Activities (a new category that carries a 15 percent weight)
- Advancing Care Information (which replaces the Medicare EHR Incentive Program and carries a 25 percent weight)
- Cost (which replaces the Value-Based Payment Modifier but is not counted in the composite score until 2018)
CMS encourages clinicians to submit measures and activities in the quality, improvement activities and advancing care information categories in order to achieve the highest possible composite score. (When the cost measure becomes a part of the composite score in 2018, no reporting will be required because it will be calculated based on claims submitted.)
Specific measure-related and reporting requirements, exceptions and nuances will differ based on various circumstances. An abundance of additional information regarding the potential quality and advancing care information measures and the improvement activities can be found on the QPP website. This article covers some basic information.
Quality
For purposes of the quality category, most MIPS participants will need to report up to six quality measures (to the extent such measures are applicable), including an outcome measure, for a minimum of 90 days. Quality measures will be determined on an annual basis. For 2017, the anesthesiology measures are as follows:
- Anesthesiology Smoking Abstinence
- Coronary Artery Bypass Graft (CABG): Preoperative Beta-Blocker in Patients with Isolated CABG Surgery
- Documentation of Current Medications in the Medical Record
- Perioperative Temperature Management
- Post-Anesthetic Transfer of Care Measure: Procedure Room to a Post-Anesthesia Care Unit (PACU)
- Post-Anesthetic Transfer of Care: Use of Checklist or Protocol for Direct Transfer of Care from Procedure Room to Intensive Care Unit (ICU)
- Prevention of Central Venous Catheter (CVC)-Related Bloodstream Infections
- Prevention of Post-Operative Nausea and Vomiting (PONV): Combination Therapy
- Preventive Care and Screening: Screening for High Blood Pressure and Follow-Up Documented
Improvement Activities
The MIPS measure for improvement activities will require most participants to attest that they completed up to four improvement activities for a minimum of 90 days. Groups that are located in a rural or health professional shortage area or with 15 or fewer participants will need to attest that they completed up to two activities for a minimum of 90 days.
Advancing Care Information
For the 2017 transition year, participants may select from one of two sets of measures based on their EHR. Subject to certain exceptions, the MIPS advancing care information category requires that participants report on at least the following required categories for a minimum of 90 days:
- Security Risk Analysis
- Electronic Prescribing
- Patient Electronic Access
- Send Summary of Care
- Request/Accept Summary of Care
Reporting and Adjustments
Participating clinicians may start collecting performance data anytime between January 1, 2017 and October 2, 2017. Note that performance data must be submitted by March 31, 2018 irrespective of the specific starting date. Similar to the Advanced APMs track, the first payment adjustments (which may be increases, decreases or neither) under MIPS will not occur until 2019.
Figure 1 briefly summarizes how practices will receive increases and decreases in Medicare payments during 2019 based on their 2017 participation.
In summary, for clinicians who select MIPS, three levels of reporting will avoid a negative MIPS payment adjustment. Clinicians can avoid a downward adjustment though the submission of a minimal amount of 2017 data (e.g., even one quality measure or improvement activity). Positive adjustments will be based on the actual performance data within the reported information and not on the amount of information submitted or the length of time for which such information is submitted.
For clinicians who submit MIPS data as an individual, the payment adjustment will be based on individual performance. Such individual data for the MIPS categories described above may be submitted through an EHR, registry or Qualified Clinical Data Registry (QCDR). Quality data may also be submitted through the Medicare claims process.
For clinicians who submit MIPS data through a group, the group will receive a single payment adjustment based on the group’s performance as a whole. Group-level data may be submitted through the CMS web interface (if the group registers by June 30, 2017) or third-party data submission services (e.g., a certified EHR, registry or QCDR). In future years, the federal government intends to permit clinicians to participate in MIPS through virtual groups and will propose further policies in such regard after soliciting additional input.
Practical Guidance and Next Steps
Physicians and their groups should promptly and proactively develop a strategy to thrive under MACRA and the QPP. If you participate, you need to determine which track is best (i.e., APMs or MIPS) based on your individual circumstances. Such determination should take into account whether your practice already participates in an Advanced APM or whether such participation in the future is desirable. If you select the MIPS track, you will need to decide whether to participate as an individual or a group, the level and timing of participation, and the type of reporting that is practicable.
CMS recommends that physicians take the following steps to prepare for MIPS in 2017:
- Check that your EHR is certified by the Office of the National Coordinator for Health Information Technology. If it is, it should be ready to capture information for the MIPS advancing care information category and certain measures for the quality category.
- Consider using a QCDR or a registry to extract and submit your quality data.
- Use the QPP website to explore the MIPS data your practice can choose to send in. Check to see which measures and activities best fit your practice.
The federal government offers resources to assist small practices through the Transforming Clinical Practice Initiative and through certain small, rural and health professional shortage area exceptions. Additional resources are available through governmental guidance, professional associations, consultants, software, technology and practice management companies, attorneys and others.
Additional QPP resources are available at the following sites:
- https://qpp.cms.gov/
- https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/Value-Based-Programs/MACRA-MIPS-and-APMs/MACRA-MIPS-and-APMs.html.
- www.ama-assn.org/MACRA
- http://www.asahq.org/quality-and-practice-management/macra
- https://innovation.cms.gov/initiatives/Transforming-Clinical-Practices/
Good luck. You can do this.
181 Fed. Reg. 77008 (Nov. 4, 2016).
3https://qpp.cms.gov/docs/QPP_Executive_Summary_of_Final_Rule.pdf.
Kathryn (Kate) Hickner, Esq. is an attorney at Ulmer & Berne LLP, where she co-chairs the firm’s Health Care Practice Group. Additional information regarding Kate’s background, experience, publications and presentations can be found at http://www.ulmer.com/attorneys/Hickner-Kathryn-E.aspx. She can be reached at (216) 583-7062 and khickner@ulmer.com. -
The Perioperative Surgical Home: Preoperative Risk Stratification, Optimization and Value
Rick Bushnell, MD, MBA
Director, Department of Anesthesia, Shriners Hospital for Children, Los Angeles, CA
and Clinical Anesthesiologist, Huntington Memorial Hospital, Pasadena, CAPayers, patients and partners are demanding better outcomes, and evolving healthcare paradigms are begging for greater anesthesia engagement. If you have been following this series, then you already know that the perioperative surgical home (PSH) is the answer to the call and the future of our specialty. What you may not know is how easy it can be as an anesthesiologist to make a contribution.
Stationing an anesthesiologist in the preoperative clinic is magic. The presence of anesthesia medical knowledge is magic to the preoperative nurses, magic to the patients and magic to the surgeons. Preoperative clinic nurses need support and direction when complicated patients present. Surgeons need the ability to obtain an anesthesia consult and patients truly need reassurance sooner than three minutes before surgery that the entire surgical continuum is engaged for their benefit.
Anesthesia offers major value to all of these people. The fact that we selflimit our presence to three minutes before surgery sends the message that we are unengaged. As anesthesiologists, we know nothing could be farther from the truth. We each have spent years developing the skills needed to spot trouble. Too often, though, we’re spotting it too late in the process and off-loading the medical issues, responsibility and leadership.
It is now time to translate our intuitive anesthesia preoperative skills into more objective assessments, management and leadership. The PSH provides the practice platform by which to lead the entire surgical process and continuum. The anesthesia preoperative appointment uses the same skills you have honed for years. It consists of a directed anesthesia history and physical, risk stratification and management. You already know how to assess a patient and past medical record, so I’ll save the lecture. What’s new and improved is the use of the American College of Surgeons National Surgical Quality Improvement Program (NSQIP)1 to objectify and augment your professional intuition and communicate the information effectively to others.Consider the 83-year-old patient I recently saw in our PSH. She presented for right total knee arthroplasty with a diagnosis of diabetes, chronic poorly controlled hypertension, 3+ pitting edema at the ankles and no cardiac consult. Her NSQIP calculation is shown in Figure 1. Easy enough; I sent her for a cardiac consult, and the echocardiogram results came back with a hyper-dynamic heart, 81 percent ejection fractions and an ascending aortic root dilation of 4.8 cm (severe). The preoperative clinic appointment, the consult and the surgical risk calculator all facilitated a more timely and objective conversation between the surgeon, the patient and the anesthesiologist. This would not have been possible on the day of surgery, if the edema had been caught at all. This process saved time, money and maybe a life, all well worth the investment in the PSH.
For cases that are allowed to proceed to surgery, the PSH appointment then becomes about optimization. Consider the Generalized Protocol (Figure 2) for Enhanced Recovery After Surgery (ERAS). As an anesthesiologist, you control the largest portion of this protocol and you stand to make a huge contribution right there. This is because the largest portion of ERAS involves the avoidance of opioids. That avoidance starts during the PSH preoperative appointment. In our preoperative appointments, we start patients on a seven-day regimen of acetaminophen, Celebrex and gabapentin (two days preoperatively and five days postoperatively). By coupling this with intraoperative ultrasound regional nerve blocks, we have reduced our opioid requirements by 75 percent. (The depiction of the first-order pharmacokinetic dosing logic and the timing of surgical incision are shown in Figure 3.)
Pain management in the PSH—a service that only an anesthesiologist can provide—is essential for the effective delivery of the core ERAS protocols. Other portions of our protocol include two days of twice-daily skin decolonization (Hibiclens protocol for the surgical site), two days of pulmonary preconditioning with an incentive spirometer, and two days of amino acid, carbohydrate and essential fatty acid loading (immunonutritional optimization). Additionally, we should not underestimate the importance of the message being delivered by an anesthesiologist. Coaching by an anesthesiologist on these optimization protocols sends a powerful message to patients of the importance of their own medical outcome: “This is your surgery and your outcome and this is how to get the best result.” Mid-level providers do not have the credibility to deliver this message as effectively.
The PSH, NSQIP, ERAS and postoperative results can most effectively be managed by a physician anesthesiologist. It means using the skills you already have and understanding the importance of objective risk stratification and optimization. This is real value that only you as an anesthesiologist can deliver. These are positive outcomes that will become evident in your hospital’s quality metrics and increase your anesthesia group’s value to your institution. That value and those metrics will be useful in negotiations with your accountable care organization.As the 5th century B.C. Japanese warlord Sun Tzu said: “Victorious warriors win first, then go to war.” Win first with your risk stratification, with your optimization and by demonstrating value in your metrics, and then have that ACO conversation.
1American College of Surgeons National Surgical Quality Improvement Program®, https://www.facs.org/quality-programs/acs-nsqip
Rick Bushnell, MD, MBA is the Director of the Department of Anesthesia, Shriners Hospital for Children, Los Angeles, CA and a Clinical Anesthesiologist at Huntington Memorial Hospital in Pasadena, CA. Dr. Bushnell graduated from the University of Illinois College of Medicine and attended the University of Pittsburgh Medical Center, and Loma Linda University for internship and residency. He has been with Pacific Valley Medical Group since 2003 and consults with Shriners Hospital for Children, Los Angeles. He and his partner have six adopted children in Tanzania where he serves as Visiting Clinical Anethesiologist at St. Elizabeth’s Hospital for the Poor in Arusha. He can be reached at propofolstingsme@gmail.com. -
Hope Is Not a Strategy: How to Create Your Strategic Business Plan
Will Latham, MBA
President, Latham Consulting Group, Inc., Chattanooga, TNIn the previous issue of The Communiqué (“Hope Is Not a Strategy: A Primer for Anesthesia Groups on Strategic Planning,” Fall 2016) we described the need for strategic planning and described the overall process. This process includes:
- Developing mission and vision statements for the group.
- Identifying internal strengths and weaknesses and external opportunities and threats.
- Discussing key issues.
- Developing objectives and strategies.
- Creating action plans to implement those strategies.
Let’s now turn to the “nuts and bolts” of how your anesthesia group can conduct a successful strategic planning process.
Retreat vs. Series of Meetings
Anesthesia group strategic planning meetings provide an opportunity for the physicians to discuss key issues and develop plans for the group.The meeting process typically comes in one of two forms: (1) a retreat; or (2) a series of meetings.
We believe that a retreat approach is the preferable process for the following reasons:
- With a series of meetings, you will chew up a lot of time reorienting everyone to what you are doing and what has been decided.
- Often, the attendee mix changes from meeting to meeting, the result being that the group zig-zags in its decision making.
- Typically, groups conduct these meetings in the evening, which is when the physicians also tend to be tired or stressed. The result is that discussions often turn to the same subjects discussed at the group’s regular meetings.
A strategic planning retreat might last one to two days, depending on the issues to be addressed and the time the physicians are willing to give to the process.
Preparing for the Retreat
It is essential to use the time spent at a retreat in the most efficient and effective manner possible. Why? - Most managers and group leaders know that it’s hard to pull all the physicians together. When you have them together, you want to make the most of it.
- The most expensive part of the process is the time at the retreat. If you multiply the number of people in the room by an hourly rate for an eight-hour day, you end up with a large number. For example, if you have 20 people in the room, eight hours at an hourly rate of $300 would cost $48,000.
Retreat time needs to be structured to be as efficient and effective as possible. That’s why preparation is key. Preparation involves considering the following:
- Who will be the participants?
- What will be the timing of the meeting?
- Who will serve as the retreat facilitator?
- What data/information will be needed for the meeting?
- What are the key issues?
- What is the agenda?
- What other arrangements are needed?
We will cover the first two items—participants and timing—in this article and the remaining preparation steps in future articles.
Participants
Who should attend the anesthesia group’s strategic planning retreat? Typically, attendees should include all shareholder physicians and the group’s manager. Depending on your group’s situation, you might also consider:
- Shareholder-track physicians
- Employed physicians
- Selected mid-level providers
- The group’s CPA
- Other advisors
Typically, we recommend the following:
- The group should limit the number of attendees, especially those who are more likely to be "observers" (such as members of the administrative team beyond the manager, employed physicians or mid-level providers). You want the physicians to have a free and open discussion about the issues. Sometimes physicians "clam up" if too many non-shareholders are in the room.
- If you include non-shareholder physicians, you might want to consider having a "shareholder-only" segment.
Timing
You will need to agree on the timing of the meeting—both when will it be held and how long the retreat will last.Most anesthesia groups conduct their retreats over a weekend. If the group plans to allocate one and one-half days to the process, often, it allocates a full day on Saturday and a half-day on Sunday.
The group should pick a time when most, if not all, of the physicians can be present. However, every group has some who are more involved and vocal than others. The timing should be planned to make sure these engaged physicians attend. If you try to avoid the "nay-sayers," they will use that as an excuse to resist implementing the plan.
Logic would say the retreat should be held in the fall so that once it is complete, management can develop the annual business plan and budget, and implementation can begin in January. However, we find that most groups conduct their retreats on weekends in January through April to avoid holding the retreat on weekends during nicer weather.
Agenda
Once the preceding steps have been taken it is time to put together the meeting agenda. Your agenda might look like this if you are conducting a one and one-half or two-day retreat.
Saturday
- Meeting goals and ground rules
- Decision making
- Interview feedback:
- Internal analysis - strengths and weaknesse
- Environmental analysis - opportunities and threats
- Mission and vision statement
- Discuss key strategic issues
Sunday
- Discuss key strategic issues, continued
- Next steps in strategic planning process
- Summary
As you can see, the retreat includes some introductory work related to meeting goals, ground rules and decisions; feedback from the interviews; and the work of defining the mission and vision and discussion of key strategic issues.
Other Arrangements
You also need to make some detailed arrangements about where the meeting will be held. We typically recommend a meeting room at a hotel. Hotels are usually set up to host meetings and can provide meal services. Meeting at the hospital is typically a bad idea as hospital meeting rooms are not conducive to a group meeting, and many hospitals don’t offer food service on weekends when meetings are typically held.Some groups hold their retreats out of town and use meals and evenings to build camaraderie. While this is can be a good idea, some physicians are resistant to traveling. You will need to determine your group’s willingness to travel.
If you do decide to hold the meeting out of town, we suggest that you do not make it a “family outing.” Family outings have two downsides: (1) reduced time for camaraderie-building and physician-to-physician interaction; and (2) increased anxiety among some physicians to complete the retreat work as fast as possible to spend time with their families.
You will also need to make a final decision as to how long you will meet. As noted earlier, the length of the meeting depends on two things:
- The issues to be covered
- The amount of time the physicians are willing to give to the planning process
If they are only willing to give one day, you will need to prioritize your key issue list to make sure the most important issues are covered. You will also need to make sure the meeting room is set up in the way you like (we typically suggest a U-shaped table set-up) and has flipcharts available to record discussion points and decisions, and that you arrange for any needed handouts.
Communication About the Retreat
The last task in preparing for your retreat is developing a memo and sending it and the agenda to the participants. The memo package should:
- Describe strategic planning and tell why it is important.
- Discuss the goals of the retreat.
- Include details of the retreat (where and when).
- Include the agenda.
- Include important background information related to specific issues (cost benefit analysis, etc.).
- Include articles about the future of healthcare. Underline or highlight the important passages.
Strategic Planning for Larger Groups
Once a group grows to a certain size (e.g., 25-30) it becomes increasingly difficult to conduct a planning retreat that meets the following criteria:
- All physicians attend the retreat.
- There is an in-depth and complete discussion of the important issues.
The problem is group processes. With 50 people in the room, it is nearly impossible to have a complete debate and discussion that includes all members. What often happens is that five or six individuals debate the issues while everyone else watches.
If you must have all of the physicians in the room, these problems can be mitigated by:
- Using the retreat as an information- sharing only meeting
- Using subgroups to discuss issues
- Using a rigorous process to discuss and debate motions that were developed prior to the retreat
We have used the following approach for large group strategic planning efforts that balance the desire for involvement with the ability to have beneficial in-depth discussion on the issues.
Step 1: Survey/Interviews
Typically, all physicians are surveyed to obtain their input on:
- Group strengths and weaknesses
- Opportunities and threats the group faces
- How group members would like to see the group evolve
- The issues that should be addressed during the planning process
- Other questions that the group would like to ask
In addition to the surveys, we typically conduct individual interviews with those who will attend the “Board+” Retreat (discussed below).
Step 2: “Board+” Retreat
A subset of the group then meets to discuss key issues and develop plans for the group. Typically this group is composed of the board and other key leaders. It is best to keep this group to 15 or fewer. The meeting typically lasts one to two days, with one and one-half days being the most common. This group develops what we call the “draft” plan for the group. At this meeting the attendees:
- Develop or update the group’s mission/vision
- Review environmental opportunities and threats
- Discuss internal strengths and weaknesses
- Create clear goals and objectives
- Work to resolve key issues facing the group
Subsequent to the retreat, a draft plan is developed that is a written summary of the conclusions reached at the retreat.
Step 3: Full Group Meeting
Following the Board+ Retreat, a meeting of all physicians is conducted and the results of the planning retreat presented. At this time, all physicians will be able to give their feedback about the results of the planning process.
This step is usually completed at an evening dinner meeting. It is important to note that the goal of this step is not to re-do the work of the retreat. Instead, the larger group is asked three questions:
- What plans or objectives are you most pleased with?
- What changes/improvements to the plan would you suggest?
- What key issues were not adequately addressed in the draft plan?
Operationally, the physicians sit at small tables of six or so, with at least one person at each table who attended the retreat. You should try to spread out the “nay-sayers” to prevent negative momentum.
Once again, this meeting is to allow the shareholders to have one more chance to provide input into the planning process.
Step 4: Board Adoption
At a board meeting the board members review the results from the full group meeting and decide whether the draft plan should be adjusted. The final plan is then adopted by the board. This process balances the need for input, in-depth discussion and decisionmaking.
Will Latham, MBA is President of Latham Consulting Group, Inc., which helps medical group physicians make decisions, resolve conflict and move forward. For more than 25 years Mr. Latham has assisted medical groups in the areas of strategy and planning, governance and organizational effectiveness, and mergers, alliances and networks. During this time he has facilitated over 900 meetings or retreats for medical groups; helped hundreds of medical groups develop strategic plans to guide their growth and development; helped over 130 medical groups improve their governance systems and change their compensation plans; and advised and facilitated the mergers of over 120 medical practices representing over 1,200 physicians. Mr. Latham has an MBA from the University of North Carolina in Charlotte. He is a frequent speaker at local, state, national and specialty-specific healthcare conferences. Mr. Latham can be reached at (704) 365- 8889 or wlatham@lathamconsulting.com.
 Our current system is oriented toward intervention and what is possible; emerging models emphasize prevention and experientially-based minimization of avoidable complications. Modeling focuses on balancing optimization of outcomes, costs and patient satisfaction versus fragmented silos of care (e.g., particular physicians or specialties). Disconnects between the consumer (patient) and the producer (professionals) are barriers to balancing costs and utility. The current system does not value or anticipate the questions of how often it meets expectations, at what costs and relative risks. Additionally, the patient has no affirmative responsibility to optimize their personal health. And finally, the system itself is a barrier.
Our current system is oriented toward intervention and what is possible; emerging models emphasize prevention and experientially-based minimization of avoidable complications. Modeling focuses on balancing optimization of outcomes, costs and patient satisfaction versus fragmented silos of care (e.g., particular physicians or specialties). Disconnects between the consumer (patient) and the producer (professionals) are barriers to balancing costs and utility. The current system does not value or anticipate the questions of how often it meets expectations, at what costs and relative risks. Additionally, the patient has no affirmative responsibility to optimize their personal health. And finally, the system itself is a barrier. Financial penalties for delivering a different mix of services pose transitional risks to physicians in several ways. As their health improves, patients require fewer services or avoid developing a disease. They experience fewer complications and comorbidities requiring intervention. However, despite these improvements, practice overhead does not decrease; rent and utilities are not pegged to quality of care or resource utilization.
Financial penalties for delivering a different mix of services pose transitional risks to physicians in several ways. As their health improves, patients require fewer services or avoid developing a disease. They experience fewer complications and comorbidities requiring intervention. However, despite these improvements, practice overhead does not decrease; rent and utilities are not pegged to quality of care or resource utilization. A Guide to Physician-Focused Alternative Payment Models, prepared by the American Medical Association (AMA) and the CHQPR, identifies seven potential models. Since this is an emerging concept with no other resources that synthesize the material as well as this publication, the following excerpts/paraphrases in quotes are from that comprehensive document, followed by examples to stimulate thought on how these models could benefit practices and communities.
A Guide to Physician-Focused Alternative Payment Models, prepared by the American Medical Association (AMA) and the CHQPR, identifies seven potential models. Since this is an emerging concept with no other resources that synthesize the material as well as this publication, the following excerpts/paraphrases in quotes are from that comprehensive document, followed by examples to stimulate thought on how these models could benefit practices and communities. “APM #4: Physician-Facility Procedure Bundle...the goal is to incentivize physicians to choose the most appropriate facility to deliver particular procedures and to work with the facility to improve efficiency and quality.... Patient benefits from receiving high quality care at the lowest-cost facility with coordinated and efficient care.... Payer benefits because the Alternative Payment Entity (APE) could accept a lower payment for the bundle than the total separate amounts under current payment systems. Physician practices benefit by using the BP to cover the costs of services not currently billable or inadequate, and by receiving compensation for innovations that reduce costs at the facility.”
“APM #4: Physician-Facility Procedure Bundle...the goal is to incentivize physicians to choose the most appropriate facility to deliver particular procedures and to work with the facility to improve efficiency and quality.... Patient benefits from receiving high quality care at the lowest-cost facility with coordinated and efficient care.... Payer benefits because the Alternative Payment Entity (APE) could accept a lower payment for the bundle than the total separate amounts under current payment systems. Physician practices benefit by using the BP to cover the costs of services not currently billable or inadequate, and by receiving compensation for innovations that reduce costs at the facility.” This essentially takes Models 4 and 5 and adds the post-discharge management and readmission risk components. While optimally a later, more mature option after experience in Models 4 and 5, market and political pressures may make this the initial option. The Comprehensive Care for Joint Replacement (CJR) Model added hip and femur fractures as a proposed rule APM in August.
This essentially takes Models 4 and 5 and adds the post-discharge management and readmission risk components. While optimally a later, more mature option after experience in Models 4 and 5, market and political pressures may make this the initial option. The Comprehensive Care for Joint Replacement (CJR) Model added hip and femur fractures as a proposed rule APM in August. Asa C. Lockhart, MD, MBA is Co-Founder and Principal of Golden Caduceus Consultants, an anesthesiology consulting firm in Seabrook, TX. Over the past 16 years, GCC has developed stabilization strategies for more than 185 hospitals and/or anesthesia groups and departments in 37 states. In addition to his consulting work, Dr. Lockhart had an active anesthesia practice in Tyler, TX and has an MBA with an emphasis in healthcare that brings validity and insight to the challenges facing many anesthesia groups and hospitals. Dr. Lockhart is the founder and course director for the ASA Certificate in Business Administration Course created by the ASA Committee on Practice Management. He was also a member of the ASA Committee on Future Models of Anesthesia Practice and has served as president and treasurer of the Texas Society of Anesthesiologists. He serves on the AMA Council on Medical Services, which develops healthcare policy options for consideration by the AMA House of Delegates, and is a vice-chair with the National Physicians’ Council for Health Care Policy. He can be reached at (903) 521-6728 and
Asa C. Lockhart, MD, MBA is Co-Founder and Principal of Golden Caduceus Consultants, an anesthesiology consulting firm in Seabrook, TX. Over the past 16 years, GCC has developed stabilization strategies for more than 185 hospitals and/or anesthesia groups and departments in 37 states. In addition to his consulting work, Dr. Lockhart had an active anesthesia practice in Tyler, TX and has an MBA with an emphasis in healthcare that brings validity and insight to the challenges facing many anesthesia groups and hospitals. Dr. Lockhart is the founder and course director for the ASA Certificate in Business Administration Course created by the ASA Committee on Practice Management. He was also a member of the ASA Committee on Future Models of Anesthesia Practice and has served as president and treasurer of the Texas Society of Anesthesiologists. He serves on the AMA Council on Medical Services, which develops healthcare policy options for consideration by the AMA House of Delegates, and is a vice-chair with the National Physicians’ Council for Health Care Policy. He can be reached at (903) 521-6728 and  We look forward to seeing many of you at the 2017 ASA Practice Management Conference in Grapevine, Texas.
We look forward to seeing many of you at the 2017 ASA Practice Management Conference in Grapevine, Texas. Although it is more than 800 pages long, the MACRA final rule is designed to simplify participation by eligible clinicians. MACRA essentially replaces the old methodology used to determine the Medicare Physician Fee Schedule. This methodology, the Sustainable Growth Rate formula, threatened to impose payment cutbacks for physicians for more than a decade. The QPP aims to reward the provision of high quality and efficient services through a single cohesive system that unifies and replaces several different Medicare payment programs.
Although it is more than 800 pages long, the MACRA final rule is designed to simplify participation by eligible clinicians. MACRA essentially replaces the old methodology used to determine the Medicare Physician Fee Schedule. This methodology, the Sustainable Growth Rate formula, threatened to impose payment cutbacks for physicians for more than a decade. The QPP aims to reward the provision of high quality and efficient services through a single cohesive system that unifies and replaces several different Medicare payment programs.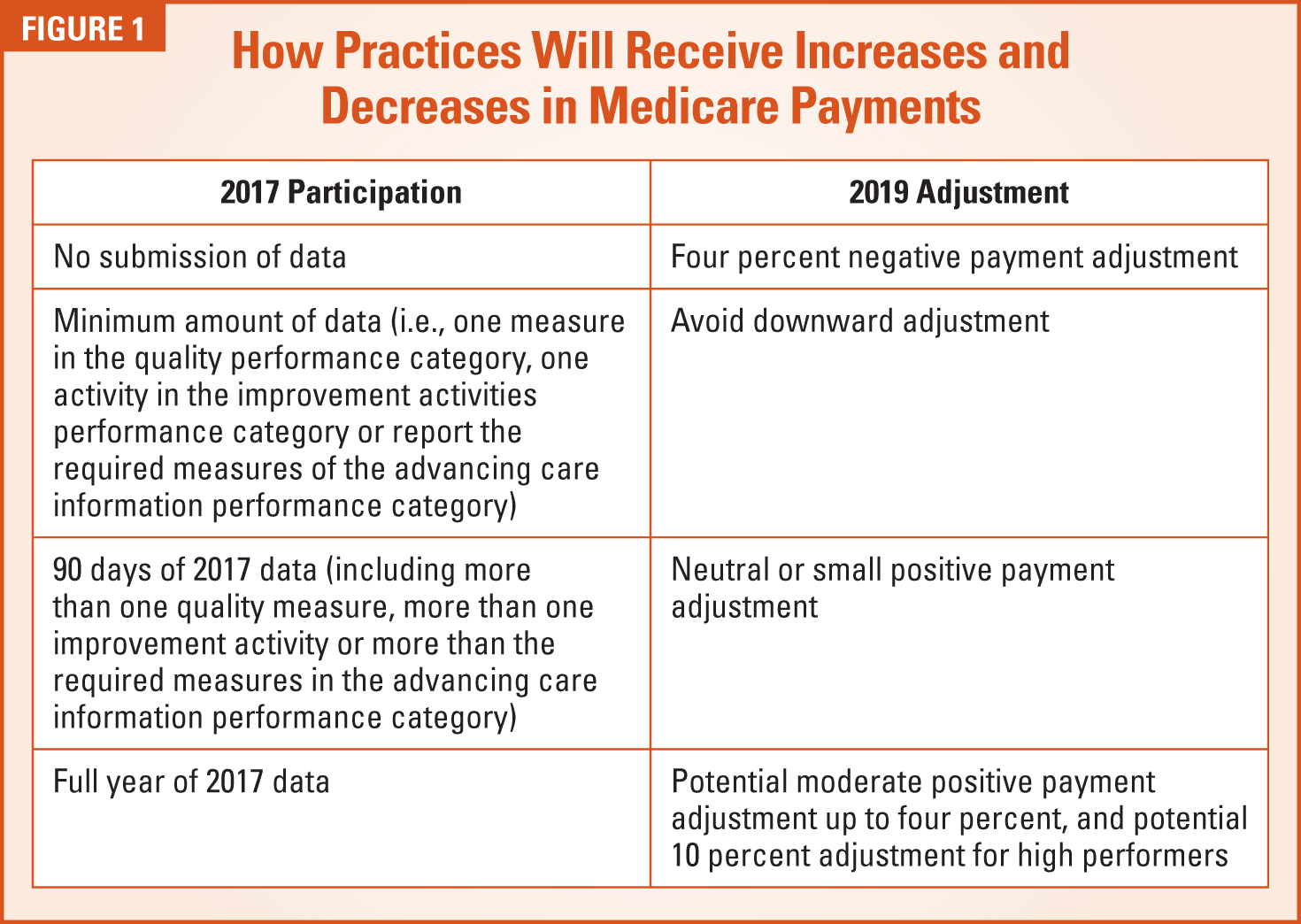

 Kathryn (Kate) Hickner, Esq. is an attorney at Ulmer & Berne LLP, where she co-chairs the firm’s Health Care Practice Group. Additional information regarding Kate’s background, experience, publications and presentations can be found at
Kathryn (Kate) Hickner, Esq. is an attorney at Ulmer & Berne LLP, where she co-chairs the firm’s Health Care Practice Group. Additional information regarding Kate’s background, experience, publications and presentations can be found at  It is now time to translate our intuitive anesthesia preoperative skills into more objective assessments, management and leadership. The PSH provides the practice platform by which to lead the entire surgical process and continuum. The anesthesia preoperative appointment uses the same skills you have honed for years. It consists of a directed anesthesia history and physical, risk stratification and management. You already know how to assess a patient and past medical record, so I’ll save the lecture. What’s new and improved is the use of the American College of Surgeons National Surgical Quality Improvement Program (NSQIP)1 to objectify and augment your professional intuition and communicate the information effectively to others.
It is now time to translate our intuitive anesthesia preoperative skills into more objective assessments, management and leadership. The PSH provides the practice platform by which to lead the entire surgical process and continuum. The anesthesia preoperative appointment uses the same skills you have honed for years. It consists of a directed anesthesia history and physical, risk stratification and management. You already know how to assess a patient and past medical record, so I’ll save the lecture. What’s new and improved is the use of the American College of Surgeons National Surgical Quality Improvement Program (NSQIP)1 to objectify and augment your professional intuition and communicate the information effectively to others.


 The PSH, NSQIP, ERAS and postoperative results can most effectively be managed by a physician anesthesiologist. It means using the skills you already have and understanding the importance of objective risk stratification and optimization. This is real value that only you as an anesthesiologist can deliver. These are positive outcomes that will become evident in your hospital’s quality metrics and increase your anesthesia group’s value to your institution. That value and those metrics will be useful in negotiations with your accountable care organization.
The PSH, NSQIP, ERAS and postoperative results can most effectively be managed by a physician anesthesiologist. It means using the skills you already have and understanding the importance of objective risk stratification and optimization. This is real value that only you as an anesthesiologist can deliver. These are positive outcomes that will become evident in your hospital’s quality metrics and increase your anesthesia group’s value to your institution. That value and those metrics will be useful in negotiations with your accountable care organization. Rick Bushnell, MD, MBA is the Director of the Department of Anesthesia, Shriners Hospital for Children, Los Angeles, CA and a Clinical Anesthesiologist at Huntington Memorial Hospital in Pasadena, CA. Dr. Bushnell graduated from the University of Illinois College of Medicine and attended the University of Pittsburgh Medical Center, and Loma Linda University for internship and residency. He has been with Pacific Valley Medical Group since 2003 and consults with Shriners Hospital for Children, Los Angeles. He and his partner have six adopted children in Tanzania where he serves as Visiting Clinical Anethesiologist at St. Elizabeth’s Hospital for the Poor in Arusha. He can be reached at
Rick Bushnell, MD, MBA is the Director of the Department of Anesthesia, Shriners Hospital for Children, Los Angeles, CA and a Clinical Anesthesiologist at Huntington Memorial Hospital in Pasadena, CA. Dr. Bushnell graduated from the University of Illinois College of Medicine and attended the University of Pittsburgh Medical Center, and Loma Linda University for internship and residency. He has been with Pacific Valley Medical Group since 2003 and consults with Shriners Hospital for Children, Los Angeles. He and his partner have six adopted children in Tanzania where he serves as Visiting Clinical Anethesiologist at St. Elizabeth’s Hospital for the Poor in Arusha. He can be reached at  Anesthesia group strategic planning meetings provide an opportunity for the physicians to discuss key issues and develop plans for the group.
Anesthesia group strategic planning meetings provide an opportunity for the physicians to discuss key issues and develop plans for the group. It is essential to use the time spent at a retreat in the most efficient and effective manner possible. Why?
It is essential to use the time spent at a retreat in the most efficient and effective manner possible. Why?  You will need to agree on the timing of the meeting—both when will it be held and how long the retreat will last.
You will need to agree on the timing of the meeting—both when will it be held and how long the retreat will last. You also need to make some detailed arrangements about where the meeting will be held. We typically recommend a meeting room at a hotel. Hotels are usually set up to host meetings and can provide meal services. Meeting at the hospital is typically a bad idea as hospital meeting rooms are not conducive to a group meeting, and many hospitals don’t offer food service on weekends when meetings are typically held.
You also need to make some detailed arrangements about where the meeting will be held. We typically recommend a meeting room at a hotel. Hotels are usually set up to host meetings and can provide meal services. Meeting at the hospital is typically a bad idea as hospital meeting rooms are not conducive to a group meeting, and many hospitals don’t offer food service on weekends when meetings are typically held. Will Latham, MBA is President of Latham Consulting Group, Inc., which helps medical group physicians make decisions, resolve conflict and move forward. For more than 25 years Mr. Latham has assisted medical groups in the areas of strategy and planning, governance and organizational effectiveness, and mergers, alliances and networks. During this time he has facilitated over 900 meetings or retreats for medical groups; helped hundreds of medical groups develop strategic plans to guide their growth and development; helped over 130 medical groups improve their governance systems and change their compensation plans; and advised and facilitated the mergers of over 120 medical practices representing over 1,200 physicians. Mr. Latham has an MBA from the University of North Carolina in Charlotte. He is a frequent speaker at local, state, national and specialty-specific healthcare conferences. Mr. Latham can be reached at (704) 365- 8889 or
Will Latham, MBA is President of Latham Consulting Group, Inc., which helps medical group physicians make decisions, resolve conflict and move forward. For more than 25 years Mr. Latham has assisted medical groups in the areas of strategy and planning, governance and organizational effectiveness, and mergers, alliances and networks. During this time he has facilitated over 900 meetings or retreats for medical groups; helped hundreds of medical groups develop strategic plans to guide their growth and development; helped over 130 medical groups improve their governance systems and change their compensation plans; and advised and facilitated the mergers of over 120 medical practices representing over 1,200 physicians. Mr. Latham has an MBA from the University of North Carolina in Charlotte. He is a frequent speaker at local, state, national and specialty-specific healthcare conferences. Mr. Latham can be reached at (704) 365- 8889 or