eAlerts
-
Disruption and the Theory of the Anesthesia Business
Michael R. Hicks, MD, MBA, MHCM, FACHE
CEO, EmCare Anesthesia Services, Dallas, TXThe anesthesia business, regardless of whether one chooses to define it as the practice of medicine, nursing, or some hybrid, is in the midst of upheaval. Increasing market consolidation, mergers, acquisitions and introduction of private equity funding have made the business of managing anesthesia delivery services increasingly complex. Bear in mind that delivering anesthesia and managing the delivery of anesthesia services are two very different things.
 Our unparalleled improvements in patient safety, quality, and, ultimately, morbidity and mortality make us justifiably proud of the specialty’s success and the envy of the rest of health care. One would think that this remarkable history of clinical success would provide stability for the business side of anesthesia practice. After all, the clinical product that we provide is orders of magnitude safer than when I entered the specialty 25 years ago. If anything, however, I believe our advances have actually laid the foundation for the rapid changes that we are seeing in the finance and management sides of the anesthesia business. This success now requires us to ask whether the care that we deliver and the service that we provide fit with the requirements of the health care system of the future.
Our unparalleled improvements in patient safety, quality, and, ultimately, morbidity and mortality make us justifiably proud of the specialty’s success and the envy of the rest of health care. One would think that this remarkable history of clinical success would provide stability for the business side of anesthesia practice. After all, the clinical product that we provide is orders of magnitude safer than when I entered the specialty 25 years ago. If anything, however, I believe our advances have actually laid the foundation for the rapid changes that we are seeing in the finance and management sides of the anesthesia business. This success now requires us to ask whether the care that we deliver and the service that we provide fit with the requirements of the health care system of the future.The Need to Change
In reality, our current clinical successes have done nothing to diminish the increasing demands for additional service and cost containment nor stemmed the downward pressures on reimbursement for anesthesia services. Discussion of these demands isn’t necessarily something new among anesthesiologists and CRNAs. What is new, however, is that these demands are now part of the much broader discussion of how health care is funded, delivered, and integrated into evolving models of health care delivery. Unfortunately, from my perspective, many leaders in anesthesiology are poorly equipped for this broader discussion and continue to view the care we deliver, and more importantly, how we deliver it, through the lens of history. These leaders are clinging to what has worked or what is desired by our profession over what is needed or affordable by those who receive care, benefit by its delivery, or are responsible for its funding.
Based on my observations and extensive interactions in health care, working within the anesthesia sector as well as with other physicians, nurses, hospital providers, and policy makers over the last five years, not only do I suggest that many practices are at risk, but also our continued relevance as a specialty. If we do not recognize and react appropriately to environmental and market changes occurring now outside of our usual span of attention, much of what we have known to be the domain of anesthesiologists and CRNAS may instead become the purview of other professionals. Changing relationships—even convergence—between employers, health systems, payers, and surgeons, coupled with continuing demands for value-based solutions, may necessitate the creation of multiple pricing tiers, variable coverage models, and multiple types and combinations of clinicians in order to meet the economic and quality requirements in the future perioperative environment.
Much of this reasoning is outside the traditional framework embraced by anesthesia leaders, our national professional societies, and on a more immediate and practical level, our own practice groups. To complicate matters, our ability to embrace future delivery models is hindered by a historical anchoring bias by many leaders of our specialty who believe that the way anesthesia services have been delivered, and by whom, should dictate how they are delivered in the future. More importantly, the resistance to the changing market forces is driven by a desire to maintain the status quo to protect current political power or to maximize current income and return on investment by those leading and within our organizations. Lessons from the business world outside of anesthesia suggest that these forces present difficult barriers for market incumbents to overcome. Fortunately, difficult does not mean it is impossible. Successful strategy formation and implementation requires analytical introspection and an acceptance that markets, whether in other businesses or in health care, ultimately drive demanding bargains when it comes to delivering a return on investment. Also fortunately, there are some tools such as the conceptual modeling techniques of Peter Drucker and Clayton Christensen that offer us the ability to understand and possibly devise strategies for a successful future for both our practices and for the specialty itself.Peter Drucker’s “Theory of the Business” Model
An appropriate way to frame the discussion is through Peter Drucker’s “Theory of the Business” model (Drucker, 1994). In this seminal work Drucker proposed that every business has an underlying theory, or set of assumptions, that drives both strategy and tactics. As long as the theory fits the reality of the market then the business has an opportunity to define a strategy for success (note that strategy formulation and implementation are different endeavors).
Drucker’s model entails three fundamental sets of assumptions involving the business’s environment (Why does the organization get paid?), mission (What does the organization consider to be meaningful results?), and core competencies (Where does the organization need to excel to maintain leadership?). Clarity, consistency, and focus are the hallmarks of successful business theories. Furthermore, Drucker also outlines requirements for a theory of the business to be valid (Drucker, 1994).
The first of these is a requirement that all of the assumptions concerning environment, mission, and core competencies must fit reality. So what are the typical assumptions we have made historically in anesthesia practice? Generally, our assumptions have been on the nature of the primary customer (patient, surgeon, facility, or payer), the delivery model required (physician only, care team, CRNA only), and payment methodology (fee-forservice or salaried position) to name but a few. Despite the current chatter concerning surgical homes, anesthesia clinicians today primarily get paid to safely provide anesthesia services during surgical procedures. Some practices offer pain medicine, acute and/or chronic, and a very few offer some sort of preoperative screening function. For mission, the assumption is that the primary and secondary customers, however the practice defines them, are satisfied with the service offered. Finally, the core competencies for most anesthesia practices are built around performing the aforementioned clinical activities “well enough” to maintain the current business relationship.
Secondly, the assumptions have to be consistent (“fit”) with each other. Consider the example of an anesthesia practice that works in a facility with an open anesthesia staff (their environment). The group’s mission, therefore, is to satisfy the needs of its surgeon customers and its core competencies revolve around making sure that their activities primarily satisfy the surgeons. This typically assumes a required level of clinical proficiency but also adequate availability to meet the convenience needs of the surgeons. Note that the needs of the hospital administration, payers, other physicians, and even patients may be of secondary importance in this group’s theory of its business. Fit in this case is achieved by recognizing the needs of the surgeons and ensuring that the business is built around delivering solutions to meet those needs.
Similarly, groups in closed or exclusive anesthesia staff relationships may have a somewhat different set of assumptions around environment, mission, and competencies that the reader should contemplate. Here, the primary customer of the anesthesia practice may very well be the facility administration and nursing staff. The surgeons, while primary customers of the hospital, may instead be important but secondary customers of the anesthesia group. As an aside, I will anticipate and respond to the wellworn argument that the patient is the primary concern. I agree, the patient is the primary concern on an individual basis. However, the anesthesia business is more complicated and complex than a simple summation of individual patient clinical encounters. Nearly every anesthesia practice that I have seen replaced has had satisfied patients. If the theory of the business for the practice is predicated merely on providing good patient care then it does not fit the current reality in our marketplace. This suggests to me the nature of the real customers and reinforces the validity of the argument that I make.This last example leads to Drucker’s third and fourth requirements for a valid business theory, which are that the environmental, mission, and core competency assumptions are known and understood throughout the practice and that the theory is tested constantly. How many anesthesia practices have counted on providing great care for individual patients as the way to continued success only to find their employment situation turned on its head? I cannot improve on the words of Drucker in this regard, particularly as it relates to many of the anesthesia practices across the country that I review while performing my various roles. Therefore, I quote Drucker directly:
An organization tends increasingly to take its theory for granted, becoming less and less conscious of it. Then the organization becomes sloppy. It begins to cut corners. It begins to pursue what is expedient rather than what is right. It stops thinking. It stops questioning. It remembers the answers but has forgotten the questions. The theory of the business becomes ‘culture.’ But culture is no substitute for discipline, and the theory of the business is discipline. (Drucker, 1994, p. 101)
Many anesthesia practices, even the specialty itself, would be well served by considering this aspect of the theory of the anesthesia business. Careful analysis of some of our long held assumptions likely explains much of what is happening in the market. Many in our profession are bewildered by the recent interest in the anesthesia business by large practice management organizations and even more so the interest of private equity firms. I am not one of them. In fact, I believe that others outside our field may have a better understanding of the future of anesthesiology than many within the specialty.
In my role as a leader of a national physician practice management company I frequently am invited to evaluate opportunities to provide anesthesia and other physician services at hospitals across the United States. This happens almost entirely because the incumbent group, be it anesthesia or otherwise, has become complacent, unresponsive, out of touch with its environment, and secure in the knowledge, erroneously so, that the group and group members are irreplaceable. This latter point, of feeling irreplaceable, is particularly interesting. Despite the fervent activity of companies like mine as well as the increased interest in the anesthesia sector of private equity firms, many anesthesia groups hold the theoretical tenet that their current customer, be it surgeon, hospital, or otherwise, cannot or will not seek an alternative to them. However, as all too many anesthesia practices are learning these days, if their business theory no longer fits with reality then someone whose theory does fit will soon be in place. These groups are failing and they do so largely because they did not continually test the validity of the assumptions underlying their particular business theory. Not surprisingly, most in the field take the easy answer, which is that the problem is a desire to decrease anesthesia expense in the form of subsidy reduction. While frequently a component of the correct answer to a specific question at the moment, current finances alone don’t explain all of the changes and the interest of the large entities now in the anesthesia business. To arrive at this answer we have to first look inward.
As Drucker suggests, are we asking all of the right questions? Do we really expect that time-based billing is viable in a world where everyone else—facility, surgeon, hospitalist, etc.—is on a fixed fee? Are anesthesiologists and CRNAs really necessary for deep sedation? Even for some general anesthetics? How much difference is there between propofol, a narcotic, a benzodiazepine, and a nondepolarizing muscle relaxant when administered in an ICU without anyone with anesthesia training as a participant and the same drug combinations when given in an operating room environment where our skills are supposedly required? When are our special skills and training needed and when are they just an added cost? On a more global level do our national societies and state medical boards function primarily to protect the public’s personal and financial health or to protect the profession?
Indeed, Drucker notes that the predominant initial reactions to a failing theory of the business are defensive in nature. This is as true, maybe more so, with failing anesthesia practices, the specialty, and possibly even with the medical profession itself as it is with any of the businesses that Drucker had in mind. I remain surprised at the number of groups that willingly choose to completely ignore the reality unfolding around them while harboring the certainty that with time the hospital or surgeons will drop whatever issues they may have with the group. Many of the groups that choose to respond do so by applying Band-Aids to problems (“patching” according to Drucker) or by attempting to erect barriers to entry for substitutes such as soliciting help from friendly surgeons or hospital board members. Consider this in the context of all too common complaints about some anesthesia practices such as failing to deal internally with physician behavioral issues, requests for more coverage, need for lower subsidization, and an overall lack of participation in hospital management and governance. I believe that what we are seeing in the market and within the profession begins to make sense.
Why is this so and what can be done about it? Drucker offers suggestions for solution paths that include the need for early diagnosis and a need to rethink the theory. This includes taking “preventative care” by using two approaches that are rarely if ever considered on the business side of health care (Drucker, 1994). The first of these, abandonment, is the most difficult, especially so for those of us in the culturally entrenched professions such as medicine. Abandonment, according to Drucker, means actively challenging everything about the business and asking questions as to whether the business would look, work, or be the same if were being developed for the first time now. If the answer is no, then the product, service or even the business itself should be abandoned or reconfigured to meet the current reality. Unfortunately, for almost every anesthesia practice, and to be fair any other business as well, the concept of abandonment is antithetical to the prevailing thinking and the answers that are generated to some of these questions are driven entirely by the nature of the current revenue stream.
For example, if one were given free reign to design a perioperative care system today would it function and be paid for as it is today? Would it have the same kind of clinicians used in the same kind of ways? Would the care team, if it existed at all, have anesthesiologists, CRNAs, and AAs or would it have others instead of, or in addition to, the process? Would non-physician supervision ratios or supervision itself even be a relevant topic? The easy answer for many of us, if easy is even possible, might be yes, as many can’t imagine a world with a different reimbursement mechanism or differing roles. However, the answers in reality are not easy and so this difficult and rigorous self-examination is critical. Even more interesting for me is that others entering the business are not necessarily burdened by the same history and financial constraints that we believe we have. As a result they are not locked into our business theory and the models that some in our business think are required. I will touch more on this shortly.Consider as an example the recent forays into the provision of deep sedation by our emergency medicine and gastrointestinal physician colleagues or registered nurses into propofol sedation. Granted, these endeavors may be motivated by money initially, by increased revenue for other medical specialties, but the relevant point here is that their success suggests that our particular business theory may be failing. Likewise, consider the increasing role of medical hospitalists in the perioperative care of the surgical patient both prior to and following the actual surgical procedure itself. These physicians may well soon be the true owners of the perioperative physician title, if they are not already. Already comfortable with delegation to advanced practice nurses and physician assistants, how long is it before their comfort extends to CRNAs and managing the care of the anesthetized patient as well? This is the heart of Drucker’s second preventative suggestion, which is to study non-customers. Radical change rarely comes from within most organizations and this is absolutely true for organizations with the guild-like mentality that is so prevalent within health care.
What then is driving the current and potential changes in the anesthesia business? I think there are at least two fundamental forces driving change in the industry. One is the obvious lack of managerial and fiscal discipline within some practices which makes the response to every question and problem either a denial of responsibility for the issue or a request for more subsidy. The second, which is a subtle change, is that the nature of the very core of the care we deliver is ripe for change.
In the case of the former, clearly some anesthesia practices struggle and ultimately fail as businesses because their theory of the business has changed. Poor service or levels of financial subsidization that have been tolerated in the past are no longer acceptable and the assumptions that they are still tolerated are now invalid, as is their theory of the business. Some groups actually have appropriate theories of their business but lack the leadership necessary to perform to their theory. Partnership groups, in my experience, are particularly susceptible to this. Difficult decisions are not easily made by large committees with members that have differing agendas. When everyone is in charge, no one is really in charge. Many anesthesia practices, like other medical practices and physicians in general, equate leadership with longevity and wisdom with accommodation. Tolerating mediocre quality and service, apathy, and non-market driven reimbursement inside a practice means forcing these attributes onto the practice’s patients, facility administration, and those who ultimately pay for the care. In addition, from a financial planning perspective, it is difficult if not impossible to have a discussion about retaining capital to invest in the future of the practice because many practice partners cannot tolerate the resulting near-term decline in clinical income. Not surprisingly, this reluctance to invest in the practice is exacerbated when those in charge aren’t going to be present when the return on the investment actually arrives several years hence.
These obstacles, however, are opportunities for others. In fact, the obstacles are core aspects of their business. Practice management companies and private equity firms see great opportunity in the anesthesia business because they bring discipline to a largely undisciplined market. Undisciplined does not refer to bad behavior, although that certainly is tolerated in many practices. It also doesn’t mean unregulated, as health care is among the most highly regulated of industries. Instead, the anesthesia business is undisciplined in the sense that market forces have not heretofore shaped the business in the conventional sense in terms of product creation, profit, loss, and market share. Mediocre service in other service industries (and like it or not anesthesia is a service industry) is typically not rewarded with continued high incomes and lack of competition except, of course, when there are high barriers to entry for competitors.This is not the case now. There are at least ten practice management companies that offer anesthesia services that have the scale, scope, and capital structure to deliver on a commitment to provide service on the national stage. Factor in large regional groups that are as yet unaffiliated, and any given anesthesia practice may have fifteen or more viable competitors for its existing business. Each of these companies purports to be capable of bringing sound business and financial management skills to bear on existing practice locations. This includes identifying whether other physicians and CRNAs will willingly do the existing work at a lower cost than the existing group. While this alone may be startling to many readers, if it’s any solace, more times than not these companies are merely the messengers that the market is changing and not the cause. Other service industries, with lower barriers to entry than health care and more transparent pricing, see more active and less tumultuous changes and on a more regular basis. No one among us would lose any sleep over changing from the US Postal Service to FedEx if we weren’t satisfied with the package delivery time.
Finally, however, for those of us that now compete nationally, particularly in companies that offer more than anesthesia management services, the more interesting opportunities are not in merely applying management expertise and financial rigor to traditional anesthesia practices, although this is certainly a very viable business strategy for the present. Instead, there are now increasing opportunities to redefine the structure of the perioperative delivery system using existing providers in potentially different ways or even different providers in novel ways. Not surprisingly, many within anesthesia view this with some degree of skepticism. What suggests that this may be done successfully?
Clayton Christensen’s Theory of Disruptive Innovation
Clayton Christensen’s work on disruptive innovation is useful for shedding light on this strategy (Christensen, 1997). For those unfamiliar with his work, Christensen has written extensively on disruptive innovation and why wildly successful businesses can ultimately fail despite continual, sometimes dramatic, improvements in their products. This usually happens because the improvements in products (and services in the case of anesthesia), unfortunately, reach a point where they outstrip the requirements of many of the existing customers. Conversely, disruptive innovation frequently results in products that are initially inferior to the general market and of limited utility to the mainstream customer. Over time, however, the disruptive technology improves to the point where it begins to meet the needs of ever increasing numbers of an industry’s customers, leading eventually to a new market order. Apple iPods are a wellknown example of this phenomenon.
Health care, interestingly enough, has been an industry that has not historically been as susceptible to this type of disruption until relatively recently (Christensen, Grossman, & Hwang, 2009; Hwang & Christensen, 2008; Herzlinger, 2006). However, I believe that this is changing in extraordinary ways. Advances in pharmacology and technology are rapidly changing how, where, and to whom we can deliver care. Remote monitoring capabilities are already changing the care for some of the most critically ill patients in hospital ICUs (Gawande, 2012). How long before this technology is deployed in operating suites? How long before the traditional perioperative team and processes are replaced? I can tell you it is sooner than most of you think.Quite frankly, we have reached a point in anesthesia where some of our capabilities outstrip the needs of many of our patients. Does every patient undergoing general anesthesia require the one-on-one presence of an anesthesiologist? Clearly not. Does every patient receiving sedation require an anesthesiologist or CRNA? Again, clearly not. Does adding or substituting propofol to the sedation regimen now change the answer? Many of us in anesthesia certainly have strong feelings on the issue but our colleagues in emergency medicine, gastroenterology, radiology, and pediatrics have similarly strong and opposing feelings. Most importantly, how long do others pay for services they don’t need?
Finally, I hope that the reader recognizes my dual attempt in this is to provide some opinions and also to provoke meaningful discussion. I am proud to be an anesthesiologist and proud to work with my physician and nursing colleagues in the field. I live in Texas and here we have the saying, “It’s just business” that is used to explain that my profiting at your expense isn’t personal. However, it is never a pleasure to see the lives of colleagues upended. Nevertheless, there are market forces at work and, if anything, they will accelerate. Understanding and applying the basic tenets of business, challenging the conventional wisdom, and seeking opportunity and innovation are all now mandatory for the practice of anesthesia. My experience caring for patients and my experience as an executive tell me that these changes are really just beginning in the business of anesthesia and that our days of being protected by the four walls of the operating room are ending. We must answer the tough questions about who we are and where we fit in the new paradigm of health care. Embracing this will allow us to change and grow as a specialty, staying viable and useful to those we serve.
Bibliography
1. Christensen, C. M. (1997). The innovator’s dilemma: when new technologies cause great firms to fail. Harvard Business Press.
2. Christensen, C. M., Grossman, J. H., & Hwang, J. (2009). The innovator’s prescription: a disruptive solution for health care. McGraw-Hill New York.
3. Drucker, P. F. (1994). The theory of the business. Harvard business review, 72(5), 95-104.
4. Gawande, A. (2012). Big med. The New Yorker.
5. Herzlinger, R. E. (2006). Why innovation in health care is so hard. Harvard business review, 84(5), 58.
6. Hwang, J., & Christensen, C. M. (2008). Disruptive innovation in health care delivery: a framework for business-model innovation. Health Affairs, 27(5), 1329-1335.
Michael R. Hicks, MD, MBA, MHCM, FACHE is a physician executive based in Dallas, Texas. He leads the anesthesia division of a national physician practice management firm as well as managing a large regional physician-owned anesthesia practice. In addition Dr. Hicks is a consultant for a national hospital and ambulatory surgery center company. He can be reached at michael@hicks.net.
-
Anesthesia Cliffhangers and Reprieves
Over the New Year holiday, Congress finally passed legislation to stop the U.S. economy from going over the fiscal cliff. The new law included a temporary reprieve from the 26.5 percent cut provided for by the Medicare Sustainable Growth Rate (SGR) formula. There will be no SGR reduction throughout 2013—a development that lets us all breathe a deep sigh of relief, even though the formula itself, and its future depredations, are still in the law. Medicare payments to physicians and hospitals are not inviolate for the coming year, it must be noted: automatic two-percent reductions will hit Medicare as part of the “sequestration” process just two months from now if Congress and the White House do not reach another deal.
For many anesthesia practices, the runup to negotiations with hospitals and payers is a cliffhanger—indeed, even contemplating future negotiations often feels precarious. Last year, one of the national anesthesia practice management companies (APMCs) acquired no fewer than eight independent and largely successful anesthesia practices. Other APMCs were just as busy. Consolidation in the health care industry, combined with the shift from paying for procedures to paying for “value,” loomed large in the guise of nonstop discussions of accountable care organization (ACO) formation.
Can anesthesia and pain medicine practices continue to do well by providing excellent patient care—without making real changes to adapt to new definitions of “value” in the health care environment? Michael Hicks, MD, MBA, chief executive officer of EmCare Anesthesia Services in Dallas, TX answers that question with a thought-provoking and well-reasoned “no” in Disruption and the Theory of the Anesthesia Business which starts on page 1 of this issue of the Communiqué.
Dr. Hicks applies Peter Drucker’s “theory of the business” model to the anesthesia department and shows that assumptions about being irreplaceable can come from the wrong questions. Instead, the department or the group should be looking at “abandonment” of products that do not meet the current reality: “For example,” Dr. Hicks asks, “if one were given free rein to design a preoperative care system today would it function and be paid for as it is today? Would it have the same kinds of clinicians used in the same kinds of ways?” As an anesthesiologist, Dr. Hicks has the standing to ask that everyone take an objective look at the role of emergency and gastrointestinal physicians, registered nurses and hospitalists from the point of view of noncustomers. As CEO of a national physician practice management company, he also has the standing to warn colleagues about the perils of poor leadership—particularly the fragmented and sluggish decision-making of overly democratic practices. The lack of disciplined and strategic leadership leaves the anesthesia marketplace wide open in many areas. It also beckons new leaders with innovative ideas about perioperative services and various forms of “disruptive innovation,” in the phrase of Clayton Christensen.
While figuring out and preparing for new paradigms, our readers must of course attend to the immediate and more familiar challenges of anesthesia and pain practice. A number of articles in this issue offer tools for that purpose, starting with Part II of Neda Ryan, Esq.’s Survey of State Prompt Pay Laws covering Montana through Wyoming (Part I, covering Alabama through Missouri, appeared in the Fall 2012 issue of the Communiqué). Other updates include a new Patient Checklist from the Institute for Safety in Office-Based Surgery by Noah Rosenberg, MD and Fred Shapiro, DO; an expanded list of reasons Why You Need a Quality Management Program by Richard Dutton, MD, MBA, and a discussion by Christopher Ryan, Esq. and Neda Ryan, Esq. of important new language in the National Correct Coding Initiative (NCCI) edits in Reporting Post-Operative Pain Management Procedures in 2013. Also on the topic of compliance, ABC Vice President Joette Derricks, CPC summarizes Three Common Issues that appear on a recent CMS contractor medical directors’ list of problem claims.
In More Ingredients for your Alphabet Soup, our newest contributor, Christine Sikora, practice administrator at Hartford Anesthesiology Associates, Inc. explains the requirements and uses of the Joint Commission’s medical staff evaluation tools, the Ongoing Professional Practice Evaluation (OPPE) and the Focused Professional Practice Evaluation (FPPE). Done properly, the OPPE/FPPE process can help anesthesia groups demonstrate the value that they bring to their hospitals.
Rounding out the Winter Issue, ABC Vice President Jody Locke, CPC discusses Is Big Better?from the point of view of a prototypical hard-working, high-quality anesthesiologist whose fifteen-physician group has been negotiating a merger with a larger practice. Mr. Locke conducts a tour de force of the concerns that will preoccupy any anesthesiologist confronted with a major practice reconfiguration. His article is, indeed, a profound counterpoint to Dr. Hicks’s discussion of the imperatives of the changing nature of anesthesiology and perioperative medicine. There can be little argument that the assumptions underlying the business of anesthesia must evolve. What remains constant, of course, and what causes such arduous self-examination is anesthesiologists’ “professional commitment to compassionate care for their patients.”Dr. Hicks stated explicitly that he hoped to provoke meaningful discussion, a hope that I share. All of us at ABC look forward to continuing the discussion and successfully navigating the challenges with you in the year ahead.
Tony Mira
President and CEO -
Is Big Better?
Jody Locke, CPC
Vice President of Anesthesia and Pain Management Services, ABCI am an anesthesiologist. The leadership of my small group of 15 physicians has been negotiating a merger with the large group in a nearby city. They have made some compelling arguments for the strategic advantages of an affiliation with a larger entity. But as logical as the rationale for merging is, so are the concerns and the questions raised by detractors. It is just not clear that all the disruption of closing out our current entity and transitioning to employment status with the big group will result in a more favorable situation for us as individuals or even as a division of the new entity. I personally worry about losing control of my practice and the clinical autonomy that attracted me to this practice in the first place. The fact is that I am still unsure how I will vote when we all get together to make a final decision.
Our mailboxes and inboxes have been full of information about all the changes taking place in healthcare. The consensus of opinion seems to indicate that the Affordable Care Act (Obamacare) will usher in a new set of priorities and focus for all health care organizations. Most observers believe that the provisions of the law will greatly encourage competition for a shrinking pool of health care dollars. The recurring theme is that now is the time to start getting ready for the changes to ensure a favorable position. The underlying implication is that those groups that fail to take the necessary precautions may well get left behind, forcing their members to look for new jobs under very different terms and conditions. My perception is that each group must either choose its own destiny, or one will be imposed on it.
The good news is that we have just renegotiated our contract with our hospital. The administration made it quite clear that they are happy with the service we provide. The only issue was whether they would increase our subsidy. We reviewed our numbers and concluded we could make do without an increase, which was exactly what the administration wanted to hear. The new agreement gives us a three year window of security but it is anyone’s guess where we will find ourselves and what kind of leverage we will have when it comes to negotiating the next agreement.A quick survey of national trends reveals just what an outlier we are. At national meetings there is considerable discussion of the amount of consolidation taking place in hospitals and medical groups. The word is that the nation’s largest anesthesia practices have kicked their expansion activities into overdrive. Organizations like Somnia, EmCare, NAPA, Northstar, et cetera, are receiving significant infusions of venture capital to fund the acquisitions of some of the country’s largest private practices. Some very shrewd investors are betting big dollars on a very different vision of the future of healthcare. The logic seems to mirror the growth of service organizations like Waste Management, which set out to acquire all the nation’s trash companies in order to minimize costs and take advantage of recycling opportunities. It is just not clear what the end game is for anesthesia. Who benefits from a gas company strategy and how?
Proponents of growth and aggregation base their arguments on three common themes they believe predict the future of the healthcare market place. They argue that the competition will focus on cost, competitive advantage—typically described in terms of customer service—and compliance. It is hard to argue with the logic of the argument. The evidence is pretty convincing. The problem is that I chose anesthesia because I wanted to be a good clinician, to give consistently compassionate care and to enjoy the satisfaction of providing a professional service. I am struggling to reconcile these personal objectives with the impersonal economics of the market place.
Ours is a physician-only practice. As often as we have analyzed the numbers and discussed the options we have yet to agree that CRNAs fit in our concept of group practice. This may make us somewhat vulnerable on an abstract scale of cost competitiveness. Maybe our subsidy could be reduced slightly if we hired nurses but that is not what our calculations indicated. In other words, the economics of the issue were simply not sufficiently compelling to make such a profound change to the structure of our practice. The fact is that many of us simply prefer to do our own cases.
Beyond the question of the cost of our staffing model, we are very active on a variety of hospital committees where we regularly contribute to cost containment initiatives. Our billing company provides us regular reports showing operating room productivity by location and hour of the day, which reports we share in our discussions of ways to improve operating room productivity. We have made suggestions to the pharmacy committee to control drug costs and we continue to be very engaged in any discussion of a new line of business or expansion opportunities that could enhance revenue to the hospital. It is hard to imagine that this commitment or focus would change much if we were part of a larger organization although it is possible that a larger group with more experience might have some new and creative ideas to infuse in the discussions. It just does not appear that there are many significant ways for anesthesia to impact the profitability of a hospital.
Some of my partners keep asking what our competitive advantage is—as if to imply that we are missing something because of our limited experience and myopic view of the market. To be honest, we are not all perfect in all aspects of the service we provide. We have had some issues. We had to encourage one member to leave as a result of his attitude and treatment of O.R. staff, but surely we are not outliers in this. All in all, the care our group members provide is excellent. Our outcomes are consistently good. We have no malpractice claims pending. All the feedback we get from administration is positive. I absolutely believe this is because we all take ownership of our franchise and do whatever we can to make sure that our future with this institution is secure.
The big groups talk about all the additional resources they bring to the relationship with an administration. They present an impressive array of charts and tables purporting to demonstrate how they monitor and evaluate the performance of every provider. Is anesthesia really such a commodity that it can be compared to the preparation of a latte at Starbucks? Is that really the ultimate goal, that every anesthetic has the consistency of a caramel macchiato? Clearly consistency of quality is important but achieving it requires considerable skill and finesse: a global set of goals and objectives must always be carefully applied to a very specific mix of patient, surgeon and procedure. I would like to believe that what makes me a good anesthesiologist is my training, my years of clinical experience and, most of all, my personal professional commitment to the art and science of the specialty.
Administratively, it is obvious that one aspect of health care that frustrates and challenges all of us is compliance. First there was the focus on billing compliance that resulted in an expensive compliance plan. Once we got used to that was had to start modifying our forms to accommodate pay for performance measures, SCIP measures and the Medicare Physician Quality Reporting System (PQRS). Now we are struggling with Meaningful Use, and the Value-Based Purchasing Modifier is just around the corner. What is next? Where will it all end? Are we really making anesthesia any safer or outcomes any better?It is not a game that I chose to play when I selected my residency program but apparently this administrative burden is part of the cost of membership. This being said, I can definitely see the advantages that a larger, well managed practice can bring to the tedium of bureaucracy. It is a big if, though. Too often bureaucracy takes on a life of its own and we lose the swifter, quicker, nimbler aspects of our practice that got us to where we are today. Too often I get the impression that such arguments are carefully crafted to support pre-conceived notions. There is always a utopian dimension to the line of reasoning as if suggesting a different strategy and approach will automatically solve today’s challenges. If there is one thing we know as anesthesiologists it is the reality that solving one problem often results in a new one. Rarely is any situation so unidimensional. Success is usually a matter of constantly triaging options.
Just as confounding as arguments for change are those intended to thwart it. Here the motives are no less pure, and too often very self-centered. Critics often do themselves in with their clear focus on the I versus the we and the today versus the tomorrow. Nevertheless the logic of criticism does infuse the debate with a critical dose of reality, especially to the extent it focuses on compensation, constituency and contractual dimensions of the question. Responsible members must carefully evaluate and assess all dimensions of the issue. Neither should we be too optimistic nor too critical in our support of one position or another.
I must confess that when asked if my compensation will improve after the merger or if my lifestyle will be enhanced, I am hard pressed to respond with anything but a gut response. I know what I want to believe, but how do I know that itwill come true. There appears to be some evidence that large groups do have higher overhead costs than smaller groups. Our overhead is about nine percent of total revenue. Some have suggested that this could increase by a percentage or two. Securing the future with well paid staff is not cheap, the argument goes. That is fine, so long as both parts of the proposition are true. We all know that sometimes you have to invest money to make money. It is certainly true that too many anesthesiologists have a pathological fixation with overhead costs.
The real question, however, must focus on the potential return on investment. Can a larger group negotiate better payor contracts? Can it extract more money out of hospitals? Can it leverage data and experience to change hospital behavior and improve operating room productivity? Hypothetically the answer to all these questions should be yes. The experience of too many practices actually indicates a somewhat mixed picture of results. This is the hardest part of this debate: sorting out the wishful thinking from the hard evidence of experience.
The constituency question is a tricky one. While many of us want to think we should have a say and input into every business decision our group makes we all know that is not realistic or practical. Constituency is one of those mythical ideals that makes us skeptical of delegation and authority. My friends from San Diego have suggested that the big group there, Anesthesia Services Medical Group (ASMG) resolved to consolidate the power of the Board of Directors a number of years ago. The formula adopted left the Board pre-eminent in all business matters but left the individual pre-eminent in all matters clinical. They explained that a simple majority of a seven-member Board can hire or fire any shareholder without cause. They explained that this was perceived as a critical strategic decision given the dynamic market conditions in San Diego. What a leap of faith that must have been. I just don’t know if my colleagues are ready for that kind of structure. We seem to be a bunch of cowboys.
My research reveals there are more than a few groups that merged when it was quite fashionable to do so, only to decide that being merged did not, actually, make things better. A case in point involved some physicians in New Mexico many years ago. Anesthesia Associates of New Mexico started in Albuquerque and then integrated the group in Santa Fe. Over time, however, the Santa Fe physicians started to feel disenfranchised. Their perspective was that they were sending their money to Albuquerque without getting anything in return. Eventually, they filed for divorce and opted for their own local market strategy and an independent entity. They would probably contend that, in retrospect, merging was not really the best option; that they got caught up in the hype without really understanding the reality of their market and their prospects and a unified group.
How big can anesthesia groups realistically get and still function well? The really big staffing companies seem very corporate and quite different from the kind of practice we have now. Just as osmotic pressure defines the size of a cell, there appears to be a delicate balance of factors that determines the optimum size of a medical practice. The organization survives to the extent that it serves the needs and expectations of its members. Historians often speak of the ebb and flow of empires; why should it be any different with anesthesia practices. I wonder how many of today’s mega group will become tomorrow’s case studies. Without a compelling vision and some strong glue to hold the organization together it will inevitably disintegrate. My perception is that if there is no compelling business strategy to enhance the security of all the members in the market, it does not matter how big the group is.What concerns me most is the fine print. No discussion of practice mergers and aggregation would be complete without a serious review of the role of the law, lawyers and contracts. Hours can be spent crafting a deal, only to have legal counsel rip it to shreds over a number of legal technicalities. A long list of issues must be addressed and considered before the final documents can be written. Anti-trust often tops the list, at least initially. Is the proposed merger even legal given the potential impact on the market? Fortunately, most mergers can satisfy the necessary requirements but this does not mean the issue can be dismissed out of hand. I have been advised by reliable sources that a qualified opinion letter is always useful, and worth its price. Specifically, I have been told that most mergers will typically be subjected to a business review if there is any antitrust concern. This is why it is preferable to address this issue up front.
No less important is the question of entity structure and name. Who is merging with whom? Which entity will be the survivor and how will the disparate provisions and governance structure of the one be incorporated into the other? Every group that seeks to merge goes into the process believing that it brings significant value to the table and wants to be recognized for its contribution to the new entity. The practical reality of anesthesia mergers seems to indicate that this is another of those ideal principles that often gets compromised as the deal gets put together. On one level this makes perfect sense. If an entity is well structured and managed and strong in its market position, why should it have to restructure every time it merges with another group? There are limits to this, however: a 75-member group covering a large geographic footprint may require an entirely different structure and management than one somewhat smaller that covers a single hospital or one tightlydefined geographic area.
I am especially concerned about billing. We happen to be very happy with our current billing vendor but the entity we are in discussions with has its own billing office. I have suggested that an audit be conducted as part of our due diligence but this request appears to have been dismissed for reasons that are not entirely clear to me. My concern here is that a large entity with a compelling vision of the future should have an infrastructure that matches the vision.
I have been assured that we will not have to pay a buy-in and that after one year we will all be made shareholders in the group we are merging with, but I have yet to see an agreement that confirms this. It is not that I am questioning what I have been told but it would be nice to see it clearly spelled out in writing. The last thing I would want is to lose my status as a result of this transaction and be reduced to just another salaried employee.
I understand that these kinds of negotiations must be managed by a small group of authorized representatives, that it is unrealistic to think that all members can participate in all discussions, but the reality of a negotiating committee making significant decisions for the membership as a whole can be very nerve-racking. It has certainly given rise to considerable concern and debate within our group. Listening to some of our debates I could not help but be reminded of the advice often given to wagon trains crossing the great plains: when you circle the wagons remember to have all the guns pointing out. It is amazing how when the discussion starts to hit home and the potential for change becomes more imminent passions start to run high. I often sense that the more our leadership suggested that we should just trust them, the more concern this has evoked among many of my partners.
So how will I vote? I am not sure. I am inclined to go with the majority—I have no desire to be seen as the holdout nay-sayer—but my training as an anesthesiologist has taught me to be cautious and skeptical. The hardest part for me is trying to envision the unfolding developments that form the basis of the argument for merging. I have been in this business long enough to have lived through similar scenarios many times. How many times have new threats to our practice unleashed the doomsayers when in most cases the initial hype far exceeded the reality of implementation? We have survived so many changes to our practice. We are still here doing what we do at a good hospital with the security of a good contract.
I know that getting beyond that reality is both my challenge and our opportunity. I remember reading a book on strategic planning that I found in an airport bookstore by Nate Booth called Strategies for Fast-Changing Times. He suggests that we must all balance two principles as we navigate change. First, he suggests, we must always remain true to the great truths of life. For me this means never giving up my professional commitment to compassionate care for my patients. He also suggests that very often the beliefs and strategies that have gotten us to where we are today will not get us to where we need to be tomorrow. Both perspectives make perfect sense to me. His point is clear. We must all find ways to use the changes taking place in our environment to our own advantage. We all have an obligation to study the issues, evaluate the options and be willing to commit ourselves to new approaches. It is not enough to sit on the sidelines judging whether change is good or bad, but rather to take responsibility for the successful outcome of our metamorphosis.
Jody Locke, CPC, serves as Vice President of Pain and Anesthesia Management for ABC. Mr. Locke is responsible for the scope and focus of services provided to ABC’s largest clients. He is also responsible for oversight and management of the company’s pain management billing team. He will be a key executive contact for the group should it enter into a contract for services with ABC. He can be reached at Jody.Locke@AnesthesiaLLC.com.
-
More Ingredients for your Alphabet Soup
Christine Sikora, CHM
Practice Administrator, Hartford Anesthesiology Associates, Inc., Hartford, CTAll of you are familiar with some of the regulatory requirements that affect your practice, as identified by their acronyms and initials: HIPAA, CMS, CoPs,PQRS, SCIP, ACO, HCAHPS. For hospital-based practices, there are now two additional “ingredients” in our regulatory alphabet soup that will require your attention: OPPE and FPPE.
Historically, hospital medical staff appointments and reappointments have been primarily a subjective process, where the clinical chief signed off on credential/privilege requests, perceived competencies and specific skills.The Joint Commission and other accrediting bodies and payers have established more stringent guidelines for the ongoing evaluation of medical staff members. The Ongoing Professional Practice Evaluation (OPPE) and Focused Professional Practice Evaluation (FPPE) are now becoming part of every hospitalbased anesthesia practice’s routine. These evaluations are expected to occur on a regular basis and serve as the key component to the hospital reappointment process.
Key Components
In adopting the Accreditation Council for Graduate Medical Education’s (ACGME) established competencies, www.acgme.org, the Joint Commission requires the following components as part of the OPPE/FPPE process (See Table 1)
A Systematic Approach to Your OPPE Program
Advice for this alphabetic avalanche: don’t panic! There is a systematic approach that you can take to develop your OPPE program. Start by considering all the elements that are part of your daily clinical practice. Do you have practice management software that tracks provider certifications, licensure, privileges and CMEs? Do you have an AIS (anesthesia information system), interfaced to a hospital EMR and further interfaced to your billing application? Do you have an event reporting application, submit to the Anesthesia Quality Institute (AQI), or track your own adverse events for quality indicators and CORE/SCIP measures JCAH SCIP?Once you have a list of these elements, continue to think of all the regulatory and required training that you might have to complete for the hospital. Such things as mandatory fire safety training, Malignant Hyperthermia drills, and risk management education sessions can fulfill components in your OPPE process.
Next, focus on clinical and billing documentation requirements. All of your qualified anesthesia providers must follow the CMS Anesthesia Conditions of Participation (CoPs). If you conduct clinical and/or billing documentation audits focusing on any of the anesthesia CoPs, audit results can be part of your OPPE program. Another hint: if your hospital conducts medical record audits for such things as non-approved medical abbreviations, missing signatures, and informed consent completion, request this information for your anesthesia providers and include it in your OPPE.
As we progress in the new era of healthcare, value-based purchasing indicators and HCAHPS scores are other ingredients that can really make your anesthesia OPPE program effective, and demonstrate your practice value to the hospital administration.
An OPPE Tool
The goal of an effective OPPE program is more objective, relying on data elements, rates, goals and thresholds. Gone are the days of the total subjective evaluation. This is a very critical point that should be used to secure your physician’s participation in the overall OPPE process. If they can manage their own performance, they are more likely to be accountable. If they are more accountable, the quality of their patient care improves.Figure 1 is an example of a physician OPPE tool that incorporates the required ACGME components and applicable anesthesia practice elements. You will see that we’ve kept three components as a subjective evaluation.
FPPE Process
Once you have your OPPE framework, the same process applies to conducting a more focused evaluation, or FPPE. An FPPE is usually completed when there is a concern about a currently privileged practitioner’s ability to provide safe, high quality patient care. It may be triggered through a peer review process, complaint, or ongoing professional practice review or for the evaluation of privilege-specific competence for all new medical staff members (including allied or adjunct staff) and for new privielges granted to members of the Medical Staff. For the FPPE, you may have specific information that would yield a “less than average” or “poor” result for one of the subjective elements, thereby requiring documentation, counseling, and/or corrective action.
“Killing two birds with one stone”
Your OPPE/FPPE template that you develop can also serve a dual process. You can adjust the template, as needed, adding in either subjective or other more objective competency evaluations, or attendance records, and utilize as part of your annual physician, CRNA, and AA internal evaluation process.
In summary, the elements for an effective OPPE program are already part of your daily clinical and operational practice management. By developing a list of your available data elements, you will be able to match them to the required OPPE components. Then develop a form that matches your data elements to the requierd OPPE components. Not only will you be able to manage the alphabet soup of rules and regulations, you will also be able to better demonstrate the value of your anesthesia practice to hospital administration.
Christine Sikora, CHM is the Practice Administrator with Hartford Anesthesiology Associates, Inc., (HAA), in
Hartford, CT, since 1998. Working with this 85 member physician anesthesia practice, Ms. Sikora focuses on corporate as well as daily operational responsibilities that include regulatory compliance and auditing, QAPI Program and staff privileging and credentialing. Contact her at (860)-545-2033 or csikora@harthosp.org. -
A Survey of State Prompt Pay Laws, Part II
Neda M. Ryan, Esq.
Clark Hill, PLC, Birmingham, MIPart I of this survey (Alabama-Missouri) appeared in the Fall 2012 issue of the Communiqué. In Part II, we summarize the laws and regulations that require health plans to pay claims within a given period in the remaining states (Montana-Wyoming), as well as the penalties for violations. Neda M. Ryan, Esq. is an associate with Clark Hill, PLC in the firm’s Birmingham, MI office.
Ms. Ryan practices in all areas of health care law, assisting clients with transactional and corporate matters; representing providers and suppliers in health care litigation matters; providing counsel regarding compliance and reimbursement matters; and representing providers and suppliers in third party payor audit appeals. She can be reached at (248)988-5884 or at nryan@clarkhill.com.
 Our unparalleled improvements in patient safety, quality, and, ultimately, morbidity and mortality make us justifiably proud of the specialty’s success and the envy of the rest of health care. One would think that this remarkable history of clinical success would provide stability for the business side of anesthesia practice. After all, the clinical product that we provide is orders of magnitude safer than when I entered the specialty 25 years ago. If anything, however, I believe our advances have actually laid the foundation for the rapid changes that we are seeing in the finance and management sides of the anesthesia business. This success now requires us to ask whether the care that we deliver and the service that we provide fit with the requirements of the health care system of the future.
Our unparalleled improvements in patient safety, quality, and, ultimately, morbidity and mortality make us justifiably proud of the specialty’s success and the envy of the rest of health care. One would think that this remarkable history of clinical success would provide stability for the business side of anesthesia practice. After all, the clinical product that we provide is orders of magnitude safer than when I entered the specialty 25 years ago. If anything, however, I believe our advances have actually laid the foundation for the rapid changes that we are seeing in the finance and management sides of the anesthesia business. This success now requires us to ask whether the care that we deliver and the service that we provide fit with the requirements of the health care system of the future. Much of this reasoning is outside the traditional framework embraced by anesthesia leaders, our national professional societies, and on a more immediate and practical level, our own practice groups. To complicate matters, our ability to embrace future delivery models is hindered by a historical anchoring bias by many leaders of our specialty who believe that the way anesthesia services have been delivered, and by whom, should dictate how they are delivered in the future. More importantly, the resistance to the changing market forces is driven by a desire to maintain the status quo to protect current political power or to maximize current income and return on investment by those leading and within our organizations. Lessons from the business world outside of anesthesia suggest that these forces present difficult barriers for market incumbents to overcome. Fortunately, difficult does not mean it is impossible. Successful strategy formation and implementation requires analytical introspection and an acceptance that markets, whether in other businesses or in health care, ultimately drive demanding bargains when it comes to delivering a return on investment. Also fortunately, there are some tools such as the conceptual modeling techniques of Peter Drucker and Clayton Christensen that offer us the ability to understand and possibly devise strategies for a successful future for both our practices and for the specialty itself.
Much of this reasoning is outside the traditional framework embraced by anesthesia leaders, our national professional societies, and on a more immediate and practical level, our own practice groups. To complicate matters, our ability to embrace future delivery models is hindered by a historical anchoring bias by many leaders of our specialty who believe that the way anesthesia services have been delivered, and by whom, should dictate how they are delivered in the future. More importantly, the resistance to the changing market forces is driven by a desire to maintain the status quo to protect current political power or to maximize current income and return on investment by those leading and within our organizations. Lessons from the business world outside of anesthesia suggest that these forces present difficult barriers for market incumbents to overcome. Fortunately, difficult does not mean it is impossible. Successful strategy formation and implementation requires analytical introspection and an acceptance that markets, whether in other businesses or in health care, ultimately drive demanding bargains when it comes to delivering a return on investment. Also fortunately, there are some tools such as the conceptual modeling techniques of Peter Drucker and Clayton Christensen that offer us the ability to understand and possibly devise strategies for a successful future for both our practices and for the specialty itself. Similarly, groups in closed or exclusive anesthesia staff relationships may have a somewhat different set of assumptions around environment, mission, and competencies that the reader should contemplate. Here, the primary customer of the anesthesia practice may very well be the facility administration and nursing staff. The surgeons, while primary customers of the hospital, may instead be important but secondary customers of the anesthesia group. As an aside, I will anticipate and respond to the wellworn argument that the patient is the primary concern. I agree, the patient is the primary concern on an individual basis. However, the anesthesia business is more complicated and complex than a simple summation of individual patient clinical encounters. Nearly every anesthesia practice that I have seen replaced has had satisfied patients. If the theory of the business for the practice is predicated merely on providing good patient care then it does not fit the current reality in our marketplace. This suggests to me the nature of the real customers and reinforces the validity of the argument that I make.
Similarly, groups in closed or exclusive anesthesia staff relationships may have a somewhat different set of assumptions around environment, mission, and competencies that the reader should contemplate. Here, the primary customer of the anesthesia practice may very well be the facility administration and nursing staff. The surgeons, while primary customers of the hospital, may instead be important but secondary customers of the anesthesia group. As an aside, I will anticipate and respond to the wellworn argument that the patient is the primary concern. I agree, the patient is the primary concern on an individual basis. However, the anesthesia business is more complicated and complex than a simple summation of individual patient clinical encounters. Nearly every anesthesia practice that I have seen replaced has had satisfied patients. If the theory of the business for the practice is predicated merely on providing good patient care then it does not fit the current reality in our marketplace. This suggests to me the nature of the real customers and reinforces the validity of the argument that I make.
 For example, if one were given free reign to design a perioperative care system today would it function and be paid for as it is today? Would it have the same kind of clinicians used in the same kind of ways? Would the care team, if it existed at all, have anesthesiologists, CRNAs, and AAs or would it have others instead of, or in addition to, the process? Would non-physician supervision ratios or supervision itself even be a relevant topic? The easy answer for many of us, if easy is even possible, might be yes, as many can’t imagine a world with a different reimbursement mechanism or differing roles. However, the answers in reality are not easy and so this difficult and rigorous self-examination is critical. Even more interesting for me is that others entering the business are not necessarily burdened by the same history and financial constraints that we believe we have. As a result they are not locked into our business theory and the models that some in our business think are required. I will touch more on this shortly.
For example, if one were given free reign to design a perioperative care system today would it function and be paid for as it is today? Would it have the same kind of clinicians used in the same kind of ways? Would the care team, if it existed at all, have anesthesiologists, CRNAs, and AAs or would it have others instead of, or in addition to, the process? Would non-physician supervision ratios or supervision itself even be a relevant topic? The easy answer for many of us, if easy is even possible, might be yes, as many can’t imagine a world with a different reimbursement mechanism or differing roles. However, the answers in reality are not easy and so this difficult and rigorous self-examination is critical. Even more interesting for me is that others entering the business are not necessarily burdened by the same history and financial constraints that we believe we have. As a result they are not locked into our business theory and the models that some in our business think are required. I will touch more on this shortly. These obstacles, however, are opportunities for others. In fact, the obstacles are core aspects of their business. Practice management companies and private equity firms see great opportunity in the anesthesia business because they bring discipline to a largely undisciplined market. Undisciplined does not refer to bad behavior, although that certainly is tolerated in many practices. It also doesn’t mean unregulated, as health care is among the most highly regulated of industries. Instead, the anesthesia business is undisciplined in the sense that market forces have not heretofore shaped the business in the conventional sense in terms of product creation, profit, loss, and market share. Mediocre service in other service industries (and like it or not anesthesia is a service industry) is typically not rewarded with continued high incomes and lack of competition except, of course, when there are high barriers to entry for competitors.
These obstacles, however, are opportunities for others. In fact, the obstacles are core aspects of their business. Practice management companies and private equity firms see great opportunity in the anesthesia business because they bring discipline to a largely undisciplined market. Undisciplined does not refer to bad behavior, although that certainly is tolerated in many practices. It also doesn’t mean unregulated, as health care is among the most highly regulated of industries. Instead, the anesthesia business is undisciplined in the sense that market forces have not heretofore shaped the business in the conventional sense in terms of product creation, profit, loss, and market share. Mediocre service in other service industries (and like it or not anesthesia is a service industry) is typically not rewarded with continued high incomes and lack of competition except, of course, when there are high barriers to entry for competitors. Health care, interestingly enough, has been an industry that has not historically been as susceptible to this type of disruption until relatively recently (Christensen, Grossman, & Hwang, 2009; Hwang & Christensen, 2008; Herzlinger, 2006). However, I believe that this is changing in extraordinary ways. Advances in pharmacology and technology are rapidly changing how, where, and to whom we can deliver care. Remote monitoring capabilities are already changing the care for some of the most critically ill patients in hospital ICUs (Gawande, 2012). How long before this technology is deployed in operating suites? How long before the traditional perioperative team and processes are replaced? I can tell you it is sooner than most of you think.
Health care, interestingly enough, has been an industry that has not historically been as susceptible to this type of disruption until relatively recently (Christensen, Grossman, & Hwang, 2009; Hwang & Christensen, 2008; Herzlinger, 2006). However, I believe that this is changing in extraordinary ways. Advances in pharmacology and technology are rapidly changing how, where, and to whom we can deliver care. Remote monitoring capabilities are already changing the care for some of the most critically ill patients in hospital ICUs (Gawande, 2012). How long before this technology is deployed in operating suites? How long before the traditional perioperative team and processes are replaced? I can tell you it is sooner than most of you think.
 Rounding out the Winter Issue, ABC Vice President Jody Locke, CPC discusses Is Big Better?from the point of view of a prototypical hard-working, high-quality anesthesiologist whose fifteen-physician group has been negotiating a merger with a larger practice. Mr. Locke conducts a tour de force of the concerns that will preoccupy any anesthesiologist confronted with a major practice reconfiguration. His article is, indeed, a profound counterpoint to Dr. Hicks’s discussion of the imperatives of the changing nature of anesthesiology and perioperative medicine. There can be little argument that the assumptions underlying the business of anesthesia must evolve. What remains constant, of course, and what causes such arduous self-examination is anesthesiologists’ “professional commitment to compassionate care for their patients.”
Rounding out the Winter Issue, ABC Vice President Jody Locke, CPC discusses Is Big Better?from the point of view of a prototypical hard-working, high-quality anesthesiologist whose fifteen-physician group has been negotiating a merger with a larger practice. Mr. Locke conducts a tour de force of the concerns that will preoccupy any anesthesiologist confronted with a major practice reconfiguration. His article is, indeed, a profound counterpoint to Dr. Hicks’s discussion of the imperatives of the changing nature of anesthesiology and perioperative medicine. There can be little argument that the assumptions underlying the business of anesthesia must evolve. What remains constant, of course, and what causes such arduous self-examination is anesthesiologists’ “professional commitment to compassionate care for their patients.” The good news is that we have just renegotiated our contract with our hospital. The administration made it quite clear that they are happy with the service we provide. The only issue was whether they would increase our subsidy. We reviewed our numbers and concluded we could make do without an increase, which was exactly what the administration wanted to hear. The new agreement gives us a three year window of security but it is anyone’s guess where we will find ourselves and what kind of leverage we will have when it comes to negotiating the next agreement.
The good news is that we have just renegotiated our contract with our hospital. The administration made it quite clear that they are happy with the service we provide. The only issue was whether they would increase our subsidy. We reviewed our numbers and concluded we could make do without an increase, which was exactly what the administration wanted to hear. The new agreement gives us a three year window of security but it is anyone’s guess where we will find ourselves and what kind of leverage we will have when it comes to negotiating the next agreement. Administratively, it is obvious that one aspect of health care that frustrates and challenges all of us is compliance. First there was the focus on billing compliance that resulted in an expensive compliance plan. Once we got used to that was had to start modifying our forms to accommodate pay for performance measures, SCIP measures and the Medicare Physician Quality Reporting System (PQRS). Now we are struggling with Meaningful Use, and the Value-Based Purchasing Modifier is just around the corner. What is next? Where will it all end? Are we really making anesthesia any safer or outcomes any better?
Administratively, it is obvious that one aspect of health care that frustrates and challenges all of us is compliance. First there was the focus on billing compliance that resulted in an expensive compliance plan. Once we got used to that was had to start modifying our forms to accommodate pay for performance measures, SCIP measures and the Medicare Physician Quality Reporting System (PQRS). Now we are struggling with Meaningful Use, and the Value-Based Purchasing Modifier is just around the corner. What is next? Where will it all end? Are we really making anesthesia any safer or outcomes any better? How big can anesthesia groups realistically get and still function well? The really big staffing companies seem very corporate and quite different from the kind of practice we have now. Just as osmotic pressure defines the size of a cell, there appears to be a delicate balance of factors that determines the optimum size of a medical practice. The organization survives to the extent that it serves the needs and expectations of its members. Historians often speak of the ebb and flow of empires; why should it be any different with anesthesia practices. I wonder how many of today’s mega group will become tomorrow’s case studies. Without a compelling vision and some strong glue to hold the organization together it will inevitably disintegrate. My perception is that if there is no compelling business strategy to enhance the security of all the members in the market, it does not matter how big the group is.
How big can anesthesia groups realistically get and still function well? The really big staffing companies seem very corporate and quite different from the kind of practice we have now. Just as osmotic pressure defines the size of a cell, there appears to be a delicate balance of factors that determines the optimum size of a medical practice. The organization survives to the extent that it serves the needs and expectations of its members. Historians often speak of the ebb and flow of empires; why should it be any different with anesthesia practices. I wonder how many of today’s mega group will become tomorrow’s case studies. Without a compelling vision and some strong glue to hold the organization together it will inevitably disintegrate. My perception is that if there is no compelling business strategy to enhance the security of all the members in the market, it does not matter how big the group is. Historically, hospital medical staff appointments and reappointments have been primarily a subjective process, where the clinical chief signed off on credential/privilege requests, perceived competencies and specific skills.
Historically, hospital medical staff appointments and reappointments have been primarily a subjective process, where the clinical chief signed off on credential/privilege requests, perceived competencies and specific skills.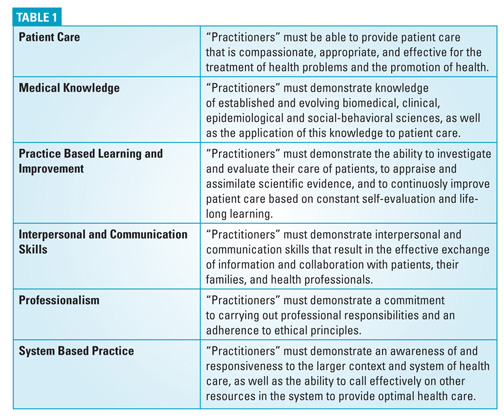
 Advice for this alphabetic avalanche: don’t panic! There is a systematic approach that you can take to develop your OPPE program. Start by considering all the elements that are part of your daily clinical practice. Do you have practice management software that tracks provider certifications, licensure, privileges and CMEs? Do you have an AIS (anesthesia information system), interfaced to a hospital EMR and further interfaced to your billing application? Do you have an event reporting application, submit to the Anesthesia Quality Institute (AQI), or track your own adverse events for quality indicators and CORE/SCIP measures JCAH SCIP?
Advice for this alphabetic avalanche: don’t panic! There is a systematic approach that you can take to develop your OPPE program. Start by considering all the elements that are part of your daily clinical practice. Do you have practice management software that tracks provider certifications, licensure, privileges and CMEs? Do you have an AIS (anesthesia information system), interfaced to a hospital EMR and further interfaced to your billing application? Do you have an event reporting application, submit to the Anesthesia Quality Institute (AQI), or track your own adverse events for quality indicators and CORE/SCIP measures JCAH SCIP? The goal of an effective OPPE program is more objective, relying on data elements, rates, goals and thresholds. Gone are the days of the total subjective evaluation. This is a very critical point that should be used to secure your physician’s participation in the overall OPPE process. If they can manage their own performance, they are more likely to be accountable. If they are more accountable, the quality of their patient care improves.
The goal of an effective OPPE program is more objective, relying on data elements, rates, goals and thresholds. Gone are the days of the total subjective evaluation. This is a very critical point that should be used to secure your physician’s participation in the overall OPPE process. If they can manage their own performance, they are more likely to be accountable. If they are more accountable, the quality of their patient care improves.
 Hartford, CT, since 1998. Working with this 85 member physician anesthesia practice, Ms. Sikora focuses on corporate as well as daily operational responsibilities that include regulatory compliance and auditing, QAPI Program and staff privileging and credentialing. Contact her at (860)-545-2033 or
Hartford, CT, since 1998. Working with this 85 member physician anesthesia practice, Ms. Sikora focuses on corporate as well as daily operational responsibilities that include regulatory compliance and auditing, QAPI Program and staff privileging and credentialing. Contact her at (860)-545-2033 or  Part I of this survey (Alabama-Missouri) appeared in the Fall 2012 issue of the Communiqué. In Part II, we summarize the laws and regulations that require health plans to pay claims within a given period in the remaining states (Montana-Wyoming), as well as the penalties for violations.
Part I of this survey (Alabama-Missouri) appeared in the Fall 2012 issue of the Communiqué. In Part II, we summarize the laws and regulations that require health plans to pay claims within a given period in the remaining states (Montana-Wyoming), as well as the penalties for violations.








