eAlerts
-
Puttin’ on AIRS
Richard P. Dutton, MD, MBA, Executive Director, Anesthesia Quality Institute, Park Ridge, IL
The Anesthesia Quality Institute was founded to create and maintain the National Anesthesia Clinical Outcomes Registry (NACOR). This project is now two and a half years old and more than 135 practices, including nine ABC clients, have contributed more than 5 million records to this “every case, every day” registry. Participants have online access to the NACOR Reporting Server, where they can see continually updated summaries of their practice performance and aggregated national benchmarks. This information, and the ability to slice and dice it to examine subsets of interest, is an important business and quality management tool. After all, what can’t be measured can’t be improved.

“Say you inadvertently gave phenyle-phrine instead of ketorolac at the end of a case. The patient’s blood pressure went to 250/130 for a few minutes, but nothing bad happened. How would your report this event?”
Immature practice response: “Did anyone notice? No harm, no foul!”
Mature practice response: “I’ll record it in our incident system, and discuss it with our QM physician. Maybe other people have had the same problem.”
In a truly mature system there are secondary methods for collecting these events. An online or AIMS-based quality-capture form is completed for each case in very well-wired practices (ABC partner ePreop™ offers such a system). Another approach is to electronically search for unusual occurrences such as sudden wide swings in blood pressure or heart rate, use of naloxone or epinephrine, or unusually short or long procedures.
The presentation itself should focus on the key anesthesia decision points, such as what preoperative tests to order, what type of anesthesia to offer, and whether to proceed with a difficult case or cancel it. When presenting to a group, it makes sense to stop at these moments and ask “What would you do?” In large and well-wired practices this can be facilitated by use of an audience response system. The results will tend to provoke conversation, which in turn will reveal two seldom acknowledged aspects of clinical anesthesia: 1) There are many ways to skin a cat, and 2) Even if they’re in the next room, we have no idea what our colleagues are doing. A well-conducted M&M system will illustrate the acceptable variability in clinical practice that occursevery day, and support the discussion with brief references to the current evidence-based scientific literature. A second goal of the M&M discussion is to identify system issues that may have contributed to the incident, and solicit suggestions for how to improve them. Examples might include “put the ketorolac in a different drawer from the phenylephrine,” “buy enough video laryngoscopes,” and “increase anesthesia staffing at lunch time.” Aside from generating good ideas, the documentation from an M&M near miss conference might be valuable ammunition when requesting resources in the Executive Office.
A National Anesthesia M&M System: AIRS
Recognizing the importance of incident-based QM at the ground level, the AQI Board of Directors made an early goal of developing such a system that could operate nationally. Fueling this request was the observation that other disciplines were already doing this (e.g. aviation, mountain climbing), and that similar systems were operated by anesthesia associations in other countries. The Anesthesia Incident Reporting System (AIRS) was born after 6 months of legal research, consultation with dozens of experts in anesthesia quality management and safety, and detailed exploration of technical possibilities. Reporting to AIRS is open to any provider with access to the Internet, by connecting to the following website: www.aqiairs.org. The report form is straightforward and easy to use, and anyone reading this article is welcome to go play around with it now. (There is a button on the last page that asks “is this a real case or a test?” If you’re experimenting, please don’t mark this as a real case!)AIRS is intended for “Any unintended event related to anesthesia or pain management with the significant potential for patient harm.” Examples include unusual manifestations of patient disease, unusual reaction to medications, abnormal function of technology, drug shortages, and facility system failures. All reports to AIRS are absolutely confidential. They are protected from legal discovery by federal law, by virtue of AQI’s status as a Patient Safety Organization. Transmission to AIRS is by secure,encrypted communication protocols, and the AIRS database itself is secured behind a firewall at the AQI. Reports may be entered as confidential (the reporter’s email and practice information is recorded) or completely anonymous. Confidential reporting allows for further discussion about interesting cases, and the ability to enter follow-up information or patient outcome as it is develops.
AIRS is open to both hits—incidents which cause an injury—and near misses. The reporting form solicits some basic structured data (patient age and BMI, type of surgical procedure, classification of the incident by body system and cause) as well as a free text description of the event. The reporter is asked to opine about the preventability of the event and lessons learned. The goal is for reporting to take less than 5 minutes for any case. Compatibility with existing incident reporting systems and local requirements is achieved by having an “email echo” feature that will send a copy of the case report to any desired third party, such as the practice or hospital QM person. Some AQI participant practices are exploring the use of AIRS on a system-wide basis, to capture all their anesthesia incidents. AQI will support this use by providing practice-specific summaries of the cases that are submitted.
AIRS opened to the public on October 1, 2011. Since that time it has garnered nearly 600 reports. Table 1 shows the broad classifications of submitted events (some cases fit in more than one class). Most of the reported events occurred in the OR, but incidents have also been captured from the ICU, obstetric unit, PACU, pain clinic and general medical ward. Incidents are reported most commonly in ASA-3 patients, and about three-quarters of the incidents were deemed preventable by the reporter.All AIRS reports are confidentially reviewed by members of the AIRS Steering Committee (Table 2), for two purposes. First, any trends in new events are noted. These may be relatively trivial— such as the repeated reporting of noninvasive blood pressure monitors that spontaneously reverted from automatic to manual mode, leaving a gap in monitoring—but the fact that they recur suggests the need for systematic improvement. AQI has shared the existence of these events with the Anesthesia Patient Safety Foundation and the Society for Technology in Anesthesia, who are working with the manufacturers to find a solution. The AIRS Committee also looks for unique cases with exceptional teaching value. These are abstracted and fictionalized, then summarized in a series of case reports published on a monthly basis in the ASA Newsletter. These cases have been appearing since October, 2011 (all are available for review online at http://www.aqihq.org/casereportsandstats.aspx). Each report describes the incident itself, the pathophysiology of the event, the system factors that may have contributed, and the key points for provider education. For example, the phenylephrine for ketorolac event described above is based on a real occurrence submitted to AIRS, and was the subject of the January, 2012, AIRS Case Report in the Newsletter.
AIRS: The FutureWith basic infrastructure now established, the AQI will leverage AIRS in a number of ways. First, we will promote it at every opportunity, until its existence and purpose are as ingrained in the minds of practicing anesthesiologists as the Malignant Hyperthermia Hotline. (Any provider who would like to receive free magnets or stickers with the AIRS web address can contact j.mlodoch@asahq.org.) Second, we will continue to select and publish interesting and educational cases—the August ASA Newsletter will include an AIRS case resulting from a little known but life-threatening complication of a very common anesthesia procedure. Third, we will continue to work on the AIRS reporting software to make it as specialty specific, but easy to use, as we possibly can. And finally, we will work with AQI participant practices to build fluid two-way communications based on AIRS that facilitate both local analysis of anesthesia events and national aggregation and reporting. If you haven’t visited the AIRS website yet, you can check it out now at http://www.aqihq.org/airsIntro.aspx. My colleagues at AQI and I hope to see you there soon.
Richard P. Dutton, MD, MBA is Visiting Professor of Anesthesiology, University of Maryland School of Medicine and AQI Executive Director. To contact Dr. Dutton or the AQI, visit www.aqihq.org. -
Quality, Safety and Practice Management
Tony Mira, President and CEO
Does the title of this article seem boring—or “timeless,” for readers in a more generous mood? If the answer to either question is yes, that is not altogether a bad thing. The United States Supreme Court decision upholding the Patient Protection and Affordable Care Act alleviated much uncertainty about healthcare reform and all of its ramifications, at least until after the November elections. Trends in the delivery of healthcare that began some time ago will continue. “The coming years will bring continued dealmaking and greater scrutiny of hospital and physician performance on quality and cost control,” as speakers said at the June 2012 Healthcare Financial Management Association Annual National Institute. Quality, safety and practice management are as important as ever to the future of anesthesia practice.
Richard P. Dutton, MD, MBA, Executive Director of the Anesthesia Quality Institute, bridges the small valley between traditional mortality and morbidity (M&M) conferences and the AQI’s newest database in the article that begins this issue of the Communique, Puttin’ on AIRS. AIRS in this context is the Anesthesia Incident Reporting System.
A national M&M system, AIRS is open to “any unintended event related to anesthesia or pain management with the significant potential for patient harm,” such as unusual reactions to medications or medical equipment failures. Reported hits and near misses serve to alert to trends in new events and to allow the AIRS Steering Committee to publish case reports of exceptional teaching value in the ASA Newsletter. We urge readers to accept Dr. Dutton’s invitation to “go play around with” the report form on the AIRS website to see this important new tool for themselves.
Another very important anesthesia safety database consists of the loss data collected by the well-known professional liability insurance company dedicated to our specialty, Preferred Physicians Medical (PPM). Brian J. Thomas, Esq., PPM’s Director of Risk Management, alerts us to the rise in allegations of negligence involving OSA patients in his article Obstructive Sleep Apnea: The Not-So-Silent Killer (a subtitle some of us can appreciate all too well). The growing number of OSA-related claims is not surprising, given the steady increase in the proportion of obese Americans. Mr. Thomas’s review of the clinical challenges and protective measures presented by patients with OSA is a good lesson on the issues that might determine the outcome of a malpractice claim.
Anesthesiology and pain medicine, like all areas of medical practice, face practice management risks as well as patient care risks. One that has surfaced only in the last few years is the exposure that comes with physicians’ use of social media – Linked In, Facebook, Twitter, YouTube, blog sites and others. Neda Mirafzali, Esq. provides an introduction to the ethical, legal and marketing landmines (and the benefits) of a public online presence in her article Social Media Policies: Do I Really Need One?
At the top of the list of anesthesia practice management issues is hospital contracting. ABC Vice President Jody Locke, CPC discusses ”New Rules for a New Era” in his article of that title. Negotiating a contract is likely to be much more challenging than it was the last time readers sat down to the task. Decisions on not just the fact or the amount, but on the specific method and data for calculating payments for the services that anesthesia groups provide to hospitals, require more preparation and sophistication than ever. And the time to start planning for the next round of negotiations begins as soon as the final signature is placed on the one just negotiated. As Mr. Locke also points out, however, in a sense “We have come full circle. With each day that passes the business of anesthesia practice management starts to resemble the practice of anesthesia: careful training, timely and reliable data and the willingness and commitment to make bold decisions quickly are the only prerequisites of success.”
Hospital Contracting: New Rules for a New Era notes the importance of data in negotiating the hospital contribution to the group’s income. ABC’s newest Vice President, Joette Derricks, reminds us of some of the reasons why we don’t take data at face value in her complementary article Understanding What Statistics Say, or Don’t Say, About Your Practice. Client Services Director Arne Pedersen, MBA, FACMPE describes another evolving factor in anesthesia groups’ net revenues, the growth of health benefit plans that increase the patients’ out-of-pocket expenses, and strategies to maximize collecting deductibles in his article Deductibles: Impact on the Physician.The fact that there is always something new to write about anesthesiology and pain medicine quality, safety and practice management makes our authors’ task interesting, to say the least. At the same time we enjoy being able to build on a wealth of experience in many, many areas. We are always mindful, nevertheless, that our physician, nurse anesthetist and anesthesiologist assistant readers entered their professions in order to provide clinical care – not necessarily in order to study the business and policy of health care. It is our ongoing hope that we make it easier for MDs, CRNAs, AAs and their practice management advisors to stay on top of our topics of mutual interest.
Sincerely,
Tony Mira
President and CEO -
Social Media Policies: Do I Really Need One?
Neda Mirafzali, Esq.,
Clark Hill PLC, Birmingham, MISocial media has transformed our culture, society and communication immensely over the past decade. Beginning with MySpace and, now, the omnipresent Facebook and Twitter, social media has not only transformed our interactions with one another, but also raises legal and ethical concerns for many professionals that use it. Anesthesiologists and pain management physicians are familiar with the heightened regulation associated with their practice, and the use of social media is no different.
Incorporating social media into an anesthesia group or pain practice’s marketing plan can be beneficial if utilized properly. However, the issues associated with social media use in the healthcare world, in general, have been shown to affect anesthesiologists and pain management physicians, specifically. Browsing some anesthesia group and pain management practices on popular social media sites as well as some online message boards revealed a number of issues that could implicate State and Federal laws as well as have a negative impact on the practice’s reputation in the community. Importantly, the issues raised extend beyond the practice’s own social media page, but also to personal profiles of nurses, interns, administrative personnel and other professionals working for the group or practice. Therefore, it is increasingly important for anesthesiologists and pain management physicians to be aware of the land mines in the social networking world and make it a priority to adopt effective social networking policies addressing the permissible and impermissible uses of social media sites.Benefits of Social Media
Social networking sites include Facebook, Twitter, LinkedIn, Yelp, YouTube, Doximity, blogs, etc. and provide an additional avenue through which individuals may communicate, including physicians with physicians and physicians with patients. Proper use of social media sites can result in increased positive exposure for your group or practice, which can lead to a greater bottom line. Utilizing social media sites as another means to communicate hours of operation, contact information or linking back to a practice or group’s website allows the practice or group to be more visible in the realms in which patients and/or prospective patients spend a great deal of their time. It is also an opportunity for the patient and/or prospective patient to “meet” his or her physician before the appointment or surgery time. An anesthesia group or pain management practice’s social media page may include headshots of the members of the group or practice as well as a short biography introducing each of them.
Additionally, the group or the practice may utilize the space to self-promote by including speaking opportunities of its group or practice members, published works or awards or honors received. All of these assist in building credibility with a population that is not familiar with the who’s who of the anesthesia or pain management world. Additionally, social media may be utilized to disseminate general information to patients like frequently asked questions, posting blog entries, or posting podcasts.
Taking advantage of social media is similar to utilizing a billboard, but free of charge. Utilizing social media may not involve creating new content to develop a page or a profile, but merely reiterating information that is already found on the group or practice’s website. Similar to a billboard, the information is placed in a familiar arena that appears more accessible and gets more traffic.
Common Social Media PitfallsAs mentioned above, social networks provide an avenue through which physicians may communicate with each other and their patients. In light of the ease with which this communication can be facilitated online, many forget, or are not aware of, the issues that are raised by such interactions. Common issues revealed in anesthesia groups or pain practices’ utilization of social media involve the posting of photographs, negative posts and the provision of medical advice on message boards.
Photographs
Placing photographs on social networking sites has the potential to raise patient privacy issues both on a State level as well as on a Federal level, under the Health Insurance Portability and Accountability Act (“HIPAA”). HIPAA applies to individually identifiable health information held or transmitted by a healthcare provider (a covered entity) in any form or media, including paper, oral, electronic, photographic, etc. Individually identifiable health information is information that relates to (a) the individual’s past, present or future physical or mental health condition; (b) the provision of healthcare to the individual; or (c) the past, present or future payment for the provision of healthcare to the individual. Therefore, posting photographs on a social media site implicate HIPAA if a patient’s individually identifiable health information is exposed. Examples of photographs that could raise HIPAA concerns include a photograph depicting a patient in a hospital bed outside of the operating room, or a photograph of a patient in the waiting room with a sign next to him or her that reads “pain management clinic.” Bear in mind, these photographs do not have to focus on the patient. If, for instance, a photograph is taken of all of the anesthesia residents, and a patient is in the background and the patient can be identified, an issue may arise.
Negative Comments
Another repeated issue encountered on anesthesia and pain group pages involved postings by patients who have had negative experiences at a group or with a particular physician or his/her staff. Allegations of unprofessionalism, breach of patient information and practicing below the standard of care were plastered on the pages of sites that many use when determining whether to receive services from a practice. Of course, disgruntled patients are inevitable in any service-oriented field, medicine included, and cannot be completely silenced; however, being aware of the capabilities of the social networking sites on which the practices and groups participate could limit the impact of such negative patient comments. Many of these sites have the functionality to prohibit posting on profiles or pages by unauthorized individuals and such functionality should, when appropriate, be utilized.
Message Boards
Message boards raise a myriad of issues, including whether a physician-patient relationship has formed or is implicated, patient privacy issues and ethical issues, to name a few.
The Physician-Patient Relationship
The Federation of State Medical Boards (the “FSMB”) issued its Model Policy Guidelines for the Appropriate Use of Social Media and Social Networking in Medical Practice (the “Model Policy”) in April of this year. Within the Model Policy, the FSMB emphasized the boundaries of the physician-patient relationship. Recognizing that “advanced technologies may facilitate the physician-patient relationship, they can also be a distracter which may lessen the quality of the interactions they have with patients.” Importantly, the FSMB touched on an issue that is not explored enough in most policies or commentaries on social networking relationships in the healthcare world: the difference between social networking interactions with current patients and the interactions with those who are not currently patients.
When a physician and a patient have formed a relationship, a physician owes that patient a duty (the extent of which is usually prescribed by state law) and a breach of that duty could result in a negligence action brought against the physician if the patient sustains damages (i.e., a medical malpractice claim). While most physicians are aware of the concept of negligence, it may not always be clear to where this duty extends. Is it limited to the confines of the hospital or the office? Does it extend to e-mail? Does it reach Facebook messages or message boards? Oftentimes it is difficult to ascertain the expectations and the full extent of a patient’s medical issue through electronic interactions and, therefore, a physician must always be mindful of the risk associated with such communications. When a physician and a patient do not yet have a formal treatment relationship formed, online interactions between the physician and patient often lead to questions about whether a relationship has formed and, if so, when? At which point does the physician have a duty? After one message? After five messages? Do the messages have to be private or can it be on a public message board? Every situation is extremely fact specific and each state has its own requirements for what constitutes a physician-patient relationship, but being aware of the fine line is important when communicating electronically with patients.Patient Privacy
As mentioned above, HIPAA is implicated by the use of social media and social networking sites. This is no exception when it comes to message boards and online forums. Anesthesiologists and pain management physicians must always be aware of, and be responsible for, the safety and security of the sites in which they participate and must ensure any discussion of a patient’s information is done so within the confines of the applicable State privacy laws and HIPAA. HIPAA permits communication between physicians for the purpose of treatment without requiring authorization from the patient. However, such communication must be secure (and the responsibility to ensure security rests with the anesthesiologist or pain management physician) so as not to result in a breach. Accordingly, the FSMB takes the position that “[w]hile physicians may discuss their experiences in non-clinical settings, they should never provide any information that could be used to identify patients. Physicians should never mention patients’ room numbers, refer to them by code names, or post their pictures.”
Ethical Issues
Interactions on social networking sites may blur the line between patient and friend. Therefore, consistent with the FSMB’s position it would behoove anesthesiologists and pain management physicians to keep separate their personal and professional social networking accounts and content to ensure a clearer divide and role.
Drafting and Instituting a Social Media Policy
While much of this article has discussed many of the common risk areas associated with social media in the healthcare arena, it takes more than just avoiding these few mines to provide protection for a practice or group. Drafting and instituting an effective social media policy raises awareness of the issues at hand as well as provides boundaries within which members of an anesthesia group or pain practice may participate in such sites. Some points to bear in mind and consider when drafting and instituting the policy include the following:
- Clarity—Drafting a policy that includes superfluous language and complex terms will be ineffective in conveying the importance of the policy and how the policy should be used. The policy should be drafted in such a way to ensure all individuals required to comply with it are capable of understanding and abiding by it.
- Definitions—Define what social networks are, so that those who are expected to comply know the extent of the policy. Does the policy only apply to Facebook and Twitter or does it apply to blogs, message boards, YouTube and other sites? Knowing the extent of the reach of the policy will assist members of your group or practice to know when their responsibilities under the policy are triggered.
- Purpose and Expectations—Why is the practice or group adopting this policy? What is the practice’s or group’s expectations for the policy? Clearly stating why this policy is being adopted and what the group hopes to achieve with it fosters a culture of compliance when everyone knows and participates in achieving a common goal.
- Social Media Officer—Designate someone to be practice or the group’s social media officer. This person would be the only (or one of the only) person with the right to access the practice or the group’s social media accounts and make amendments to it. This person could also designate the profile’s privacy settings.
- Coordination with HIPAA Policies—Ensure that the social media policy and the HIPAA policies complement one another. Because many of the issues that arise in the social media realm are patient privacy-related issues, ensuring that the two policies agree with one another and work together minimizes confusion among those expected to comply.
- Acceptable Social Media Uses—List examples of acceptable social media uses. Social media can be a powerful marketing tool and a way to reach out to patient populations. Posting general information on what patients can do before anesthesia or how patients can deal with pain, including frequently asked questions, blogging, posting podcasts, articles, group photos, highlighting awards, etc. can be a tool to assist the practice in connecting with its patients and having an online presence.
- Electronic Communication with Patients—The group or practice may find it beneficial to include in its policy the permissible parameters within which members of the group or practice may communicate with current or prospective patients electronically.
- Discipline—Including a disciplinary provision under the policy informs those required to comply with the policy that the group or practice takes the issues raised under the social media policy seriously. Moreover, if an incident arises where discipline is warranted, uniformly disciplining members of the group or practice contributes to a culture of compliance.
Included in many social media policies is blanket prohibitions on employees from disparaging the employer on social media sites. Such policies allow the employers to terminate employees for such remarks. However, incorporating such provisions in social media policies should be carefully reviewed by qualified counsel to ensure they are enforceable and will not become a source of liability for the anesthesia group or pain practice.
The National Labor Relations Board (the “NLRB”) enforces the National Labor Relations Act (the “NLRA”) and has recently turned its attention to social media policies. Specifically, the NLRB has issued two reports regarding social media policies—one in August 2011 and one in January 2012—that provide guidance on the extent to which social media policies may govern employees “concerted activity,” which is protected under Section 7 of the NLRA. Briefly, Section 7 provides that employees have a right to engage in “concerted activities” for the purpose of collective bargaining or to improve working conditions and/or terms of employment. Employees may exercise this right in person or by utilizing technology or other media, such as social networking. Employers that terminate employees who are exercising their right to engage in concerted activity may find themselves becoming legally or financially liable. According to the NLRB’s recent reports, blanket policies that prohibit disparaging remarks about the employer have been deemed overbroad and terminations pursuant to such policies have been deemed improper.
Conclusion
As with compliance plans, in general, they must be adopted and updated as times change. Incorporating a social media policy into an anesthesia group or pain management practice’s larger compliance plan would benefit any group or practice as participation on such sites, both professionally and personally, is growing exponentially.
Neda Mirafzali, Esq. is an associate with Clark Hill, PLC in the firm’s Birmingham, MI office. Ms. Mirafzali practices in all areas of health care law, assisting clients with transactional and corporate matters; representing providers and suppliers in health care litigation matters; providing counsel regarding compliance and reimbursement matters; and representing providers and suppliers in third party payor audit appeals. She can be reached at (248) 988-5884 or at nmirafzali@clarkhill.com. -
Obstructive Sleep Apnea: The Not-So-Silent Killer
Brian J. Thomas, JD, Director of Risk Management & Senior Claims Attorney,
Preferred Physicians Medical, Shawnee Mission, KSAs the prevalence of obesity in the general population is rapidly increasing, so too is the incidence of obstructive sleep apnea. Anesthesiologists face significant challenges and risks when treating patients with diagnosed obstructive sleep apnea or patients who exhibit all the signs and symptoms of obstructive sleep apnea. Concurrent with the increase in obesity and obstructive sleep apnea, Preferred Physicians Medical’s loss data reflect an increase in allegations of medical negligence involving obstructive sleep apnea patients. These cases often involve catastrophic brain damage or death. In light of the increased risks presented by obstructive sleep apnea patients, anesthesiologists frequently seek risk management advice for managing these challenging patients.
Obstructive Sleep Apnea Defined
Obstructive sleep apnea (OSA) is defined as upper airway collapse during sleep that may be accompanied by sleep disruption, hypoxemia and arterial oxygen desaturation. OSA is common in obese patients due to the propensity of fat deposition in the pharynx causing the upper airway to close. However, non-obese patients can have OSA from tonsillar hypertrophy or craniofacial abnormalities, especially in pediatric patients. OSA disrupts normal sleep patterns and results in arousal events that may lead to other symptoms including, but not limited to, hypertension, coronary artery disease, congestive heart failure, fatal arrhythmias, myocardial infarction, daytime somnolence, diabetes, and restrictive pulmonary disease.
Preoperative AssessmentPreoperative assessment of patients for potential identification of OSA includes: 1) medical record review, 2) patient and/or family interview, 3) physical examination, 4) sleep studies, and 5) preoperative x-rays for cephalometric measurement in selected cases. All obese patients, BMI ? 30, undergoing surgery should be suspected of having OSA preoperatively. There are several screening tools and scoring systems available to assist anesthesiologists in evaluating whether a patient might have OSA. However, it should be noted these screening tools and scoring systems have not been clinically validated and should be used as a guide in evaluating patients for OSA. In the absence of a sleep study, a presumptive diagnosis of OSA may be made using the STOP-BANG scoring model (see Figure 1).
Other physical characteristics such as enlarged tonsils, prominent tonsillar pillars, enlarged nasal turbinates, narrowed maxilla or mandible, pronounced tongue and enlarged adenoids are often reflected by a high Mallampati score used by anesthesiologists to predict difficulty with intubation. A high Mallampati score, with anticipated intubation difficulty, should alert the anesthesiologist and perioperative team to the high potential for OSA.
Preoperative Management
Prescribing sedatives preoperatively may be problematic for OSA patients, as they are often sensitive to sedatives, especially if the OSA is untreated. Even minimal sedation can cause airway obstruction and ventilatory arrest. Therefore, many anesthesiologists do not give preoperative sedatives to patients with OSA, unless the patient can be carefully monitored.
The most serious perioperative complication is the loss of airway control after induction of general anesthesia. Because of reduced oxygen reserve due to decrease in lung volume in the morbidly obese patient, these patients cannot tolerate a lack of ventilation for appreciable periods before hypoxemia results. It is for that reason anesthesiologists should be prepared for a difficult intubation and have all of the necessary resources and equipment, including supraglottic devices, to follow the ASA difficult airway algorithm. It may also be prudent under certain circumstances to have an experienced surgeon available at the time of induction of general anesthesia in case tracheostomy becomes necessary. An alternative to general anesthesia for OSA patients is regional anesthesia (epidural, intravenous regional or peripheral nerve block).Postoperative Care
The period of awakening from anesthesia can be problematic for patients with OSA. In patients who have undergone surgery for treatment of their OSA, the airway can be narrowed from swelling and inflammation. Also, the lingering sedative and ventilatory depressant effects of the anesthetic can pose difficulty. Perioperative vigilance should continue into the postoperative period. Some patients require postoperative intubation and mechanical ventilation until fully awake. A CPAP machine can be used in some patients postoperatively to reduce obstruction, especially if a patient has been on a CPAP preoperatively. For some patients, it may be prudent to admit them to an intermediate care or intensive care area postoperatively to facilitate close monitoring and airway support measures. Narcotics can precipitate or potentiate apnea that may result in ventilatory arrest. If narcotics are deemed necessary in the post-operative period, appropriate monitoring of oxygenation, ventilation and cardiac rhythm should be provided. SummaryPatients with OSA present many challenges to anesthesiologists. Obese and morbidly obese patients are particularly prone to this sleep disorder. Anesthesiologists frequently elicit the symptoms and suspect OSA during examination of the airway and sleep history. Special care must be taken in the management of anesthetic induction, intubation and maintenance of these patients with particular attention to titration of neuromuscular relaxation and analgesic use. Perioperative and postoperative management should ideally include CPAP therapy for those patients with diagnosed OSA. Outpatient procedures must be approached with caution and should include clinical judgment and patient selection criteria based on the severity of OSA, presence of coexisting co-morbidities, invasiveness of surgery, type of anesthesia, anticipated postoperative opioid requirements, and adequacy of post-discharge observation. Anesthesiologists should make their own independent evaluation as to whether a patient is an appropriate candidate for anesthesia in an outpatient surgery facility and admit those patients who do not meet those criteria.
Brian J. Thomas, JDis Director of Risk Management & Senior Claims Attorney for Preferred Physicians Medical Risk Retention Group, Inc. in Shawnee Mission, KS. He can be reached at (800) 562-5589 or at brian.thomas@ppmrrg.com.
References:
1. Isono S. Obstructive Sleep Apnea of Obese Adults. Anesthesiology. 2009;110:908-21.
2. ASA Practice Guidelines for the Perioperative Management of Patients with Obstructive Sleep Apnea. Anesthesiology. 2006;104:1081-93.
3. Doyle JD. Obstructive Sleep Apnea And the Surgical Patient: What the Anesthesiologist Should Know. Anesthesiology News—Guide to Airway Management. Supplement. 2009.
4. Ogan OU, Plevak DJ. Anesthesia Safety Always an Issue with Obstructive Sleep Apnea. See, http://www.apsf.org/newsletters/html/1997/summer/sleepapnea.html.
5. Joshi GP. The Adult Patient with Morbid Obesity and/or Sleep Apnea Syndrome For Ambulatory Surgery. Presentation—American Society of Anesthesiology Annual Meeting, October 16, 2010.
6. Leone, BJ. Obstructive Sleep Apnea and Anesthesia. Revista Mexicana de Anestesiologia. Vol. 30, Suppl. 1, April-June 2007.
-
Hospital Contracting: New Rules for a New Era
Jody Locke, CPC,
Vice President of Anesthesia and Pain Management Services, ABCNegotiating a contract for anesthesia services with a hospital or Ambulatory Surgery Center (ASC) has never been an activity for the faint of heart. Even under the best of circumstances the process can bring out the worst in all parties. No matter that the relationship has been mutually beneficial something inevitably crops up as a point of contention. While most groups have typically had at least one member who could navigate a few minor challenges in the past, today’s new business challenges and the stresses of a competitive healthcare marketplace have completely changed the landscape and the result is a whole new set of issues requiring a completely different approach and strategy. The most common refrain among consultants and attorneys who represent anesthesia practices for a living has become: “getting the last contract done was a cake walk compared to this.”
img src="/images/stories/Communique/Summer2012/Summer 2012 article 5 photo 1.bmp" border="0" alt="" height="275" align="left" style="margin: 10px 20px 10px 0;"
Many factors have pitted anesthesia practices against their administrations. The expansion of managed care and the perceived need to participate with key payors set the stage for a potential showdown. Certainly it was the significance of managed care contracting that triggered so many requests from hospital administrators to their anesthesia providers that they needed to form groups. Whatever the trigger, most can now identify a point in time after which things would never be quite the same again in their interactions with administration.
Paranoid cynics have tended to dismiss the change as a hostile affront to the professional integrity of the specialty and expressed their exasperation by means of a variety of passive-aggressive behaviors, but the more visionary among them saw this phenomenon for what it was, a paradigm shift that would require new approaches, that the beliefs and strategies that had gotten the practice to where it was would not get it to where it needed to be going forward. The lesson is clear, though: the earlier the rift set in and the longer it was left to fester, the harder it would be to cure and the more difficult it would be to negotiate reasonable terms for a service agreement.
How and why did this happen? Could it have been avoided? And what was the long-term impact? Many would argue that anesthesiologists have been quite myopic in their understanding of the environment in which they work. They have seen themselves as captive to a system over which they never believed they could have much influence or control. So long as this environment provided them above average incomes and favorable lifestyles, their relative captivity was not viewed as a problem.
Customer Service
It was not all that long ago—perhaps 15 or 20 years—that the anesthesia group with an exclusive contract with its hospital was the exception rather than the rule. In most hospitals they were simply not seen as necessary. How quickly things have changed. Two issues can virtually explain the origin of every anesthesia contract: the impact of managed care and a desire for the protection of exclusivity on the part of anesthesia practices. This is not to say that such agreements were entered into willingly at first or that they were generally viewed as advantageous. Many were considered a necessary evil and an unfortunate waste of time and expensive legal resources. The fact is that, as with so many other aspects of anesthesia practice, they have now become a standard fixture providing a modicum of protection until they become the catalyst for termination.
Ideally an anesthesia contract should define a franchise and codify ways to make it mutually profitable to all parties.
Ideally an anesthesia contract should define a franchise and codify ways to make it mutually profitable to all parties. The evolution of standard contract terms has been a reflection of the changing face of healthcare. Each party strives to maximize the potential value of the relationship while minimizing the exposure and risks associated with its obligations. In most cases there is more language dedicated to term and termination than economic potential and profitability. It is only recently that the proliferation of arrangements for financial support have begun to change the fundamental purpose of the document, but even here the heavy hand of the law is evident. Hospitals are strictly forbidden from paying anything more than fair market value for anesthesia services. It is a very arcane set of guidelines and conventions that defines how generous a hospital may actually be to its anesthesia providers.
To a large extent it was the very nature of anesthesia practice and the independent-mindedness of its practitioners that made the negotiation of the earliest contracts so problematic. Early negotiations were marked by some fundamental disconnects. While the administrators sought keep their options open with vague terms and loose terminology that only lawyers could interpret, the anesthesiologists kept demanding clarity and concision. While the administrators strove to minimize their risk and financial exposure, the anesthesia practices struggled to protect themselves and build in safeguards and safety nets. Worst of all, though, was the persistent request to see the books and understand just how profitable anesthesia was; this was the line in the sand that most private practices would not cross. The result was a careful, but often not-so-carefully choreographed dance around the real points of contention.
Opposite Perspectives
The history of anesthesia group formation only underscores the differences in perspective of the parties to this process. Administrators like numbers and balance sheets. Theirs is a world of averages and statistics. They use terms like ‘profitability’ and ‘bottom line’. Anesthesiologists, on the other hand, talk about the art and science of their specialty. While they plan for complications, ultimately each anesthesia provider responds to complications on an ad hoc basis. To them administrators are pencil pushers who speak an abstract administrative jargon. The anesthesia providers, on the other hand, are concrete problem-solvers intent on resolving life and death issues real-time. And so when they would sit down across from each other the administrators would propose and ponder options that anesthesiologists felt merited prompt and definitive decisions. Progress could only occur when they started to get their decision cycles in sync.
The legacy of these early days and the ensuing tectonic shift in the environment is a paranoid fear of losing control that continues to haunt specialty of anesthesiology to this day. Any attempts on the part of administration to limit the right to practice at a facility were and continue to be viewed as a violation of the rules of free trade. The single most egregious provision in most service agreements continues to be the “clean-sweep clause” that ties hospital privileges to termination of the contract. In retrospect, however, such issues and concerns were only a preview of coming attractions.
From the facility’s perspective the efforts necessary to bring anesthesia providers to the table as a single entity set the stage for a common realization that more often than not the “anesthesia group” was actually little more than a professional fraternal organization with no ability or commitment to discipline itself or speak with a single voice. Professional hospital administrators tended to be suspicious of these entities and their lack of clearly-defined business practices. Before long, administrators started to explore a variety of strategies to outmaneuver the anesthesiologists. Frustration at the inability of these group practices to speak with one voice, consistently make good on their contractual obligations and keep their own houses in order gave rise to the Request for Proposal (RFP) which in turn stimulated the growth of an entirely new industry: the anesthesia management company, of which Premier and Sheridan were prototypical examples.
No period in the history of anesthesiology has been so dramatically shaken by the winds of change as the decade of the 1990s. Health care reform threatened to undermine the viability of the specialty. Anesthesia residents fled their training programs in droves resulting in one of the most profound manpower shortages in history. The demographics of the specialty were clearly shifting as more women entered the specialty. As ambulatory surgery centers proliferated across the country, a shift in clinical venues rapidly eroded the economic underpinning of the specialty: the notion that a good day’s work in a well-placed facility would easily generate enough revenue to support the income and lifestyle requirements of the provider.
Organizationally, anesthesia practices struggled to come to terms with a whole new vocabulary that was as foreign to most as ancient Aramaic. As groups of physicians continued to form new entities, their attorneys tried to apprise them of the potential for antitrust violations. Democracy was all they knew but it did not seem to work. They struggled to adapt old ways of compensation to new forms of management, but nothing seemed to make sense. Never had the future seemed so uncertain. Is it any wonder that the American Society of Anesthesiologists(ASA) found it necessary to publish a practice management video and initiate a new conference focused exclusively on anesthesia practice management in 1994?
Many would describe the current state of anesthesia practice in nearly Marxian terms where all that matters is economics. There is more truth here than many are willing to admit. The fact is that the quality of anesthesia care overall has become so high that most patients are at greater risk driving to the hospital for a procedure than undergoing general anesthesia. Superior training and dramatic advances in technology and pharmacology have generally created the perception that serious anesthetic complications are a thing of the past. At the very point anesthesia practices need some leverage to argue their case for more financial support they find they have little to leverage; moreover, the market appears to be conspiring against them. What used to be the home court advantage of the local team is eroding quickly. The hospital now has the upper hand.
The fact is that the quality of anesthesia care overall has become so high that most patients are at greater risk driving to the hospital for a procedure than undergoing general anesthesia.
A survey of current subsidy arrangements reveals four broad categories:
- fixed annual payments,
- FTE-based support,
- service-line subsidies and,
- coverage formulas based on per diem anesthetizing location rates.
The simplest of these is the fixed annual payment where the parties sit down, throw numbers back and forth and finally agree on an amount that the hospital will pay the anesthesia group each year. This is the hospital budget driven approach. Despite administration preference for such an approach, there is little protection for the anesthesia practice and it is safe to say that what was the right number at one point in time may be totally inadequate later on. This fundamental limitation has given rise to some very creative approaches.
Sometimes the discussion will start with an assessment of the manpower necessary to meet the facility’s coverage requirements. It is not uncommon for administration to accept a staffing plan and then plug in compensation amounts and expense allocations. Inevitably the administration will also insist that the practice project collections, which are deducted from the projected cost to determine the subsidy. Such agreements inevitably define a pool of money that the group taps into based on need. More often than not, the pool is insufficient for the group to meet the projected budget.
Service-line subsidies can be far more complicated. These involve the identification of unprofitable lines of business that are deemed important to the facility. Examples might include cardiac call, obstetric coverage and the GI suite. The total subsidy each month or quarter normally involves adding up the specific types of financial support. Such an approach can be quite profitable until the hospital decides that the approach has become just too complicated and cumbersome and refuses to discuss support for any new service lines.
A new approach has been gaining currency in recent years. This method simply assigns a value to cover an anesthetizing location for a day. Typical rates range from $1700 to $2100 depending on staffing model and type of service. In the simplest cases the group will tally the number of locations covered in a month, multiply this tally by the rate agreed to and subtract actual collections to determine the invoice amount. Not all administrations will accept such flexible arrangements, but those that have, and there are many, like the potential for aligning the incentives of group and facility.
In other words, the need to provide financial support to an anesthesia practice has given rise to a very specialized form of consulting services. It is not uncommon in today’s environment for a group to hire a consultant to formulate a proposal and then for the hospital to hire another consultant to evaluate the proposal and provide its own proposal. Once the consultants agree, the terms then get turned over to the lawyers who hammer out the details of an actual contract. Needless to say, this has greatly complicated the process and added significant costs that must be borne by both parties.
Of particular note and concern to many anesthesia practices is the need to disclose considerably more financial information than used to be the case, especially as may pertain to individual provider compensation and benefits. Hospital consultants will scrutinize volume trends and payor mix to asses the adequacy of collections and accounts receivable management. No hospital wants to support a group simply because its billing function is lacking.
The need to provide financial support to an anesthesia practice has given rise to a very specialized form of consulting services.
In the final analysis, hospital contracting can be compared to running for public office. There is an expectation that once the contract is signed that the process stops and everyone goes back to work as usual. Too often this is not really what happens. More often than not the implementation of a new contract only opens a new chapter in the relationship with the hospital in which all the stakeholders are constantly evaluating whether they got it right and whether the relationship is stronger or weaker. A well known attorney, Judith Jurin Semo, Esq. often tells the story of a contract she worked on for 8 months. A month after it was signed the client came back to her asking how they could get out of the deal. Hospital contracting has gone the way of managed care contracting: a careful monitoring of each provision and condition is essential to the next round of negotiations.
Reasonable observers might well ask where all this is headed? It is a good question. Given the current uncertainty related to the future of healthcare reform and the terms of the Affordable Care Act, there is considerable speculation how much the relationship between hospitals and their hospital-based physicians is likely to change. The potential impact of Accountable Care Organizations (ACOs) is a topic of frequent concern, but such uncertainly should not mask the underlying trends that have already become very clear: most discussion of any medicalservice is now focused on cost.
It seems fairly safe to predict that four themes will inspire future discussions with hospital administrative staff. Any group anticipating a negotiation or renegotiation of a contract would be well advised to honestly consider each and to ask the tough questions necessary to use these to maximum advantage. These are more than just the buzz words of the day; they have clearly become the primary focus of hospital administrators all across the country: customer service, collaboration, cost and competition. Practices that lead with these in their proposals and interactions with administration are far more likely to achieve successful outcomes and feel more secure in their practices.
Many would argue that anesthesia has always been a quintessential service specialty. Despite the service nature of the specialty, anesthesia has come under increasing scrutiny for its lack of customer service orientation. This puzzles some providers, but others understand that what is being asked of anesthesiologists and CRNAs is a different perspective. No one doubts their qualifications to manage patients safely through the peri-operative continuum. What is not clear are how well they can address the variety of customer requirements and expectations outside the operative suite. Anesthesia practices have to reinvent themselves as more customer-friendly entities. There is an entire vocabulary of customer service that is quite foreign to the typical anesthesia practice that has little experience in satisfaction surveys, 360 degree reviews and pro-active involvement in operating room management. They also have to learn how to identify and reset customer expectations. It is clearly a new challenge for a new era in anesthesia practice management. Most anesthesia providers find it easier to manage a complicated AAA at three in the morning than to sit down with a surgeon over utilization metrics.
img src="/images/stories/Communique/Summer2012/Summer 2012 article 5 photo 6.bmp" border="0" alt="" height="220" align="right" style="margin: 10px 0 10px 20px;"If better customer service is the opening volley of a new dialogue, collaboration is what the dialogue is now about. The days of anesthesia providers showing up in the morning to do their cases and quietly disappearing at the end of the day are over. The administration wants what anesthesia brings to the table. Most anesthesia practices have more and better data about what actually happens in the operating room suite than the hospital. They also bring a tremendous body of experience to the table. The time has come for joint problem-solving and collaboration in the effective management of patients through the surgical experience. In fact, the more anesthesia groups step up to the plate and offer up their insights and ideas, the more secure they are in their franchises.
Defining Your Value Proposition
There is no doubt about the fact that the cost question poses unique and challenging questions. Hospitals do not necessarily need anesthesia groups to change how they provide care but they do need reassurance that the mode and method used is the most cost-effective possible for the value provided. The opportunity for anesthesia lies in shifting the focus of discussion from cost, per se, to value. Practices must be clear in the defining of and consistent in the implementation of their value proposition. Some assume that all hospitals would prefer to work with nurse anesthetists because they are perceived as cheaper. To the extent that such a discussion exists in a facility, anesthesia has failed to manage the terms of the discussion.
Today’s environment appears complicated to some and threatening to others but it is actually little more than the culmination of general themes and specific circumstances and should be viewed with no more skepticism than any other period in the history of the specialty. There have always been challenges and there will continue to be challenges. Success will be defined by those who can appreciate the past and use its lessons to their advantage while they develop the tools and strategies to assess the specific circumstances of their practices. In many ways it is the perfect anesthesia paradigm. We have come full circle. With each day that passes the business of anesthesia practice management starts to resemble the practice of anesthesia: careful training, timely and reliable data and the willingness and commitment to make bold decisions quickly are the only prerequisites of success. The only things standing in the way are history, tradition and an unwillingness to embrace change. The tools are and resources are widely-available and the opportunity is at hand.
img src="/images/stories/Communique/Summer2012/Summer 2012 article 5 author.bmp" border="0" alt="" height="100" align="right" style="margin: 10px 0 10px 20px;"
Jody Locke, CPC, serves as Vice President of Pain and Anesthesia Management for ABC. Mr. Locke is responsible for the scope and focus of services provided to ABC’s largest clients. He is also responsible for oversight and management of the company’s pain management billing team. He will be a key executive contact for the group should it enter into a contract for services with ABC. He can be reached at Jody.Locke@AnesthesiaLLC.com.


 Recognizing the importance of incident-based QM at the ground level, the AQI Board of Directors made an early goal of developing such a system that could operate nationally. Fueling this request was the observation that other disciplines were already doing this (e.g. aviation, mountain climbing), and that similar systems were operated by anesthesia associations in other countries. The Anesthesia Incident Reporting System (AIRS) was born after 6 months of legal research, consultation with dozens of experts in anesthesia quality management and safety, and detailed exploration of technical possibilities. Reporting to AIRS is open to any provider with access to the Internet, by connecting to the following website:
Recognizing the importance of incident-based QM at the ground level, the AQI Board of Directors made an early goal of developing such a system that could operate nationally. Fueling this request was the observation that other disciplines were already doing this (e.g. aviation, mountain climbing), and that similar systems were operated by anesthesia associations in other countries. The Anesthesia Incident Reporting System (AIRS) was born after 6 months of legal research, consultation with dozens of experts in anesthesia quality management and safety, and detailed exploration of technical possibilities. Reporting to AIRS is open to any provider with access to the Internet, by connecting to the following website: 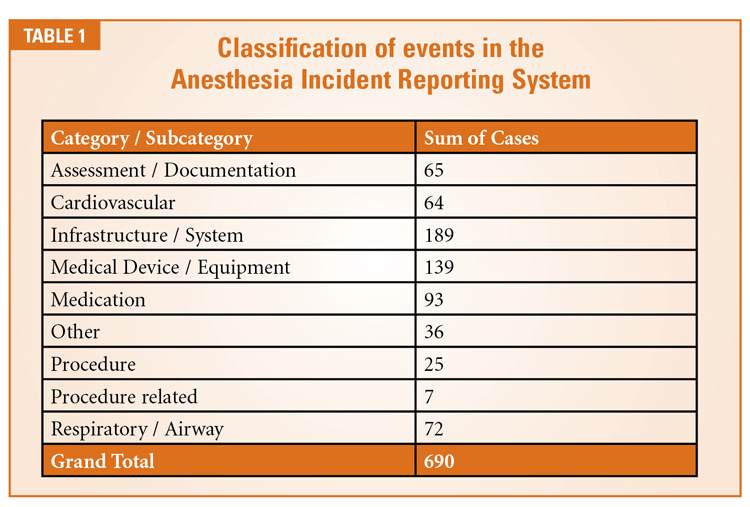 AIRS opened to the public on October 1, 2011. Since that time it has garnered nearly 600 reports. Table 1 shows the broad classifications of submitted events (some cases fit in more than one class). Most of the reported events occurred in the OR, but incidents have also been captured from the ICU, obstetric unit, PACU, pain clinic and general medical ward. Incidents are reported most commonly in ASA-3 patients, and about three-quarters of the incidents were deemed preventable by the reporter.
AIRS opened to the public on October 1, 2011. Since that time it has garnered nearly 600 reports. Table 1 shows the broad classifications of submitted events (some cases fit in more than one class). Most of the reported events occurred in the OR, but incidents have also been captured from the ICU, obstetric unit, PACU, pain clinic and general medical ward. Incidents are reported most commonly in ASA-3 patients, and about three-quarters of the incidents were deemed preventable by the reporter. AIRS: The Future
AIRS: The Future Richard P. Dutton, MD, MBA is Visiting Professor of Anesthesiology, University of Maryland School of Medicine and AQI Executive Director. To contact Dr. Dutton or the AQI, visit
Richard P. Dutton, MD, MBA is Visiting Professor of Anesthesiology, University of Maryland School of Medicine and AQI Executive Director. To contact Dr. Dutton or the AQI, visit  Hospital Contracting: New Rules for a New Era notes the importance of data in negotiating the hospital contribution to the group’s income. ABC’s newest Vice President, Joette Derricks, reminds us of some of the reasons why we don’t take data at face value in her complementary article Understanding What Statistics Say, or Don’t Say, About Your Practice. Client Services Director Arne Pedersen, MBA, FACMPE describes another evolving factor in anesthesia groups’ net revenues, the growth of health benefit plans that increase the patients’ out-of-pocket expenses, and strategies to maximize collecting deductibles in his article Deductibles: Impact on the Physician.
Hospital Contracting: New Rules for a New Era notes the importance of data in negotiating the hospital contribution to the group’s income. ABC’s newest Vice President, Joette Derricks, reminds us of some of the reasons why we don’t take data at face value in her complementary article Understanding What Statistics Say, or Don’t Say, About Your Practice. Client Services Director Arne Pedersen, MBA, FACMPE describes another evolving factor in anesthesia groups’ net revenues, the growth of health benefit plans that increase the patients’ out-of-pocket expenses, and strategies to maximize collecting deductibles in his article Deductibles: Impact on the Physician. Incorporating social media into an anesthesia group or pain practice’s marketing plan can be beneficial if utilized properly. However, the issues associated with social media use in the healthcare world, in general, have been shown to affect anesthesiologists and pain management physicians, specifically. Browsing some anesthesia group and pain management practices on popular social media sites as well as some online message boards revealed a number of issues that could implicate State and Federal laws as well as have a negative impact on the practice’s reputation in the community. Importantly, the issues raised extend beyond the practice’s own social media page, but also to personal profiles of nurses, interns, administrative personnel and other professionals working for the group or practice. Therefore, it is increasingly important for anesthesiologists and pain management physicians to be aware of the land mines in the social networking world and make it a priority to adopt effective social networking policies addressing the permissible and impermissible uses of social media sites.
Incorporating social media into an anesthesia group or pain practice’s marketing plan can be beneficial if utilized properly. However, the issues associated with social media use in the healthcare world, in general, have been shown to affect anesthesiologists and pain management physicians, specifically. Browsing some anesthesia group and pain management practices on popular social media sites as well as some online message boards revealed a number of issues that could implicate State and Federal laws as well as have a negative impact on the practice’s reputation in the community. Importantly, the issues raised extend beyond the practice’s own social media page, but also to personal profiles of nurses, interns, administrative personnel and other professionals working for the group or practice. Therefore, it is increasingly important for anesthesiologists and pain management physicians to be aware of the land mines in the social networking world and make it a priority to adopt effective social networking policies addressing the permissible and impermissible uses of social media sites. Common Social Media Pitfalls
Common Social Media Pitfalls When a physician and a patient have formed a relationship, a physician owes that patient a duty (the extent of which is usually prescribed by state law) and a breach of that duty could result in a negligence action brought against the physician if the patient sustains damages (i.e., a medical malpractice claim). While most physicians are aware of the concept of negligence, it may not always be clear to where this duty extends. Is it limited to the confines of the hospital or the office? Does it extend to e-mail? Does it reach Facebook messages or message boards? Oftentimes it is difficult to ascertain the expectations and the full extent of a patient’s medical issue through electronic interactions and, therefore, a physician must always be mindful of the risk associated with such communications. When a physician and a patient do not yet have a formal treatment relationship formed, online interactions between the physician and patient often lead to questions about whether a relationship has formed and, if so, when? At which point does the physician have a duty? After one message? After five messages? Do the messages have to be private or can it be on a public message board? Every situation is extremely fact specific and each state has its own requirements for what constitutes a physician-patient relationship, but being aware of the fine line is important when communicating electronically with patients.
When a physician and a patient have formed a relationship, a physician owes that patient a duty (the extent of which is usually prescribed by state law) and a breach of that duty could result in a negligence action brought against the physician if the patient sustains damages (i.e., a medical malpractice claim). While most physicians are aware of the concept of negligence, it may not always be clear to where this duty extends. Is it limited to the confines of the hospital or the office? Does it extend to e-mail? Does it reach Facebook messages or message boards? Oftentimes it is difficult to ascertain the expectations and the full extent of a patient’s medical issue through electronic interactions and, therefore, a physician must always be mindful of the risk associated with such communications. When a physician and a patient do not yet have a formal treatment relationship formed, online interactions between the physician and patient often lead to questions about whether a relationship has formed and, if so, when? At which point does the physician have a duty? After one message? After five messages? Do the messages have to be private or can it be on a public message board? Every situation is extremely fact specific and each state has its own requirements for what constitutes a physician-patient relationship, but being aware of the fine line is important when communicating electronically with patients. Neda Mirafzali, Esq. is an associate with Clark Hill, PLC in the firm’s Birmingham, MI office. Ms. Mirafzali practices in all areas of health care law, assisting clients with transactional and corporate matters; representing providers and suppliers in health care litigation matters; providing counsel regarding compliance and reimbursement matters; and representing providers and suppliers in third party payor audit appeals. She can be reached at (248) 988-5884 or at nmirafzali@clarkhill.com.
Neda Mirafzali, Esq. is an associate with Clark Hill, PLC in the firm’s Birmingham, MI office. Ms. Mirafzali practices in all areas of health care law, assisting clients with transactional and corporate matters; representing providers and suppliers in health care litigation matters; providing counsel regarding compliance and reimbursement matters; and representing providers and suppliers in third party payor audit appeals. She can be reached at (248) 988-5884 or at nmirafzali@clarkhill.com. Preoperative Assessment
Preoperative Assessment The most serious perioperative complication is the loss of airway control after induction of general anesthesia. Because of reduced oxygen reserve due to decrease in lung volume in the morbidly obese patient, these patients cannot tolerate a lack of ventilation for appreciable periods before hypoxemia results. It is for that reason anesthesiologists should be prepared for a difficult intubation and have all of the necessary resources and equipment, including supraglottic devices, to follow the ASA difficult airway algorithm. It may also be prudent under certain circumstances to have an experienced surgeon available at the time of induction of general anesthesia in case tracheostomy becomes necessary. An alternative to general anesthesia for OSA patients is regional anesthesia (epidural, intravenous regional or peripheral nerve block).
The most serious perioperative complication is the loss of airway control after induction of general anesthesia. Because of reduced oxygen reserve due to decrease in lung volume in the morbidly obese patient, these patients cannot tolerate a lack of ventilation for appreciable periods before hypoxemia results. It is for that reason anesthesiologists should be prepared for a difficult intubation and have all of the necessary resources and equipment, including supraglottic devices, to follow the ASA difficult airway algorithm. It may also be prudent under certain circumstances to have an experienced surgeon available at the time of induction of general anesthesia in case tracheostomy becomes necessary. An alternative to general anesthesia for OSA patients is regional anesthesia (epidural, intravenous regional or peripheral nerve block). The period of awakening from anesthesia can be problematic for patients with OSA. In patients who have undergone surgery for treatment of their OSA, the airway can be narrowed from swelling and inflammation. Also, the lingering sedative and ventilatory depressant effects of the anesthetic can pose difficulty. Perioperative vigilance should continue into the postoperative period. Some patients require postoperative intubation and mechanical ventilation until fully awake. A CPAP machine can be used in some patients postoperatively to reduce obstruction, especially if a patient has been on a CPAP preoperatively. For some patients, it may be prudent to admit them to an intermediate care or intensive care area postoperatively to facilitate close monitoring and airway support measures. Narcotics can precipitate or potentiate apnea that may result in ventilatory arrest. If narcotics are deemed necessary in the post-operative period, appropriate monitoring of oxygenation, ventilation and cardiac rhythm should be provided.
The period of awakening from anesthesia can be problematic for patients with OSA. In patients who have undergone surgery for treatment of their OSA, the airway can be narrowed from swelling and inflammation. Also, the lingering sedative and ventilatory depressant effects of the anesthetic can pose difficulty. Perioperative vigilance should continue into the postoperative period. Some patients require postoperative intubation and mechanical ventilation until fully awake. A CPAP machine can be used in some patients postoperatively to reduce obstruction, especially if a patient has been on a CPAP preoperatively. For some patients, it may be prudent to admit them to an intermediate care or intensive care area postoperatively to facilitate close monitoring and airway support measures. Narcotics can precipitate or potentiate apnea that may result in ventilatory arrest. If narcotics are deemed necessary in the post-operative period, appropriate monitoring of oxygenation, ventilation and cardiac rhythm should be provided. 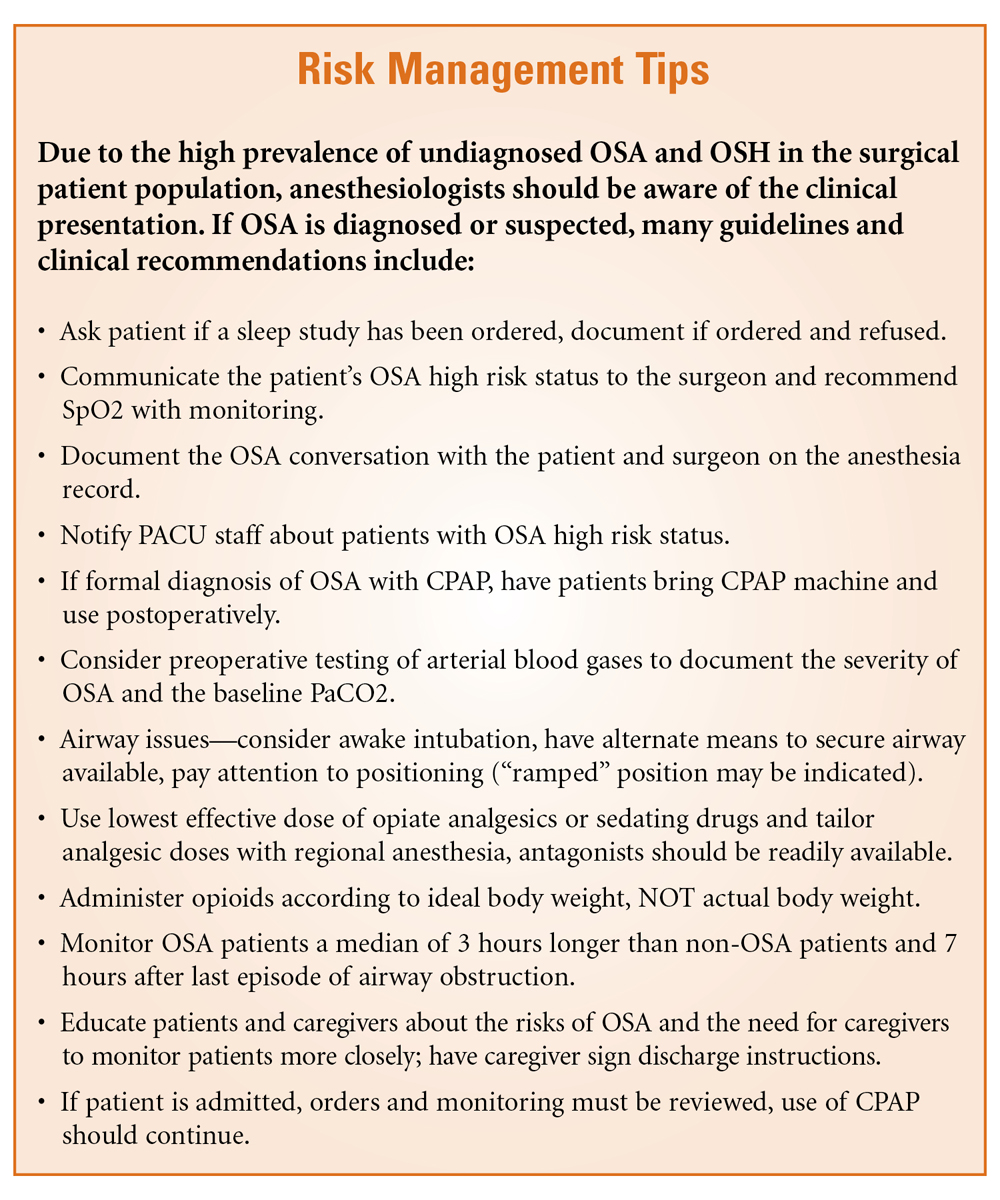 Summary
Summary Brian J. Thomas, JDis Director of Risk Management & Senior Claims Attorney for Preferred Physicians Medical Risk Retention Group, Inc. in Shawnee Mission, KS. He can be reached at (800) 562-5589 or at
Brian J. Thomas, JDis Director of Risk Management & Senior Claims Attorney for Preferred Physicians Medical Risk Retention Group, Inc. in Shawnee Mission, KS. He can be reached at (800) 562-5589 or at 


