eAlerts
-
What Anesthesiologists And Pain Management Physicians Need To Know About The RAC Program
Abby Pendleton, Esq., and Jessica L. Gustafson, Esq.
The Health Law Partners, P.C., Southfield, MIAnesthesiologists and pain management physicians, like other Medicare providers, should be prepared for increased Medicare auditing activity. The Centers for Medicare and Medicaid Services (CMS) Recovery Audit Contractor (RAC) program has been made permanent and is expanding nationwide, and the RACs will begin auditing in the very near future. Medicare providers should be aware that RAC claim denials and overpayment demands, like other Medicare denials, can be appealed through the standard Medicare appeals process.
1. RECOVERY AUDIT CONTRACTORS
Section 306 of the Medicare Prescription Drug, Improvement and Modernization Act of 2003 (MMA) directed the Department of Health and Human Services (HHS) to conduct a three-year demonstration program using RACs. The demonstration began in 2005 in the three states with the highest Medicare expenditures: California, Florida and New York. In 2007, the demonstration expanded to include Massachusetts, South Carolina and Arizona. The purpose of the RAC demonstration program was to determine whether the use of RACs would be a cost-effective way to identify and correct improper payments in the Medicare program.
The RAC demonstration program proved highly “cost effective” to CMS. Over the three-year demonstration, the RACs identified more than $1.03 billion in improper payments. The vast majority of this amount, $992.7 million, constituted alleged overpayments. According to CMS, factoring in the underpayments returned to providers and suppliers ($37.8 million), the claims overturned on appeal ($46 million), the amounts improperly recouped and returned to providers upon re-review ($14 million) and the operating costs of the demonstration program ($201.3 million), the RAC program was successful in returning $693.6 million to the Medicare Trust Funds. CMS estimates that the RAC demonstration program cost approximately 20 cents for each dollar returned to the Medicare Trust Funds.1

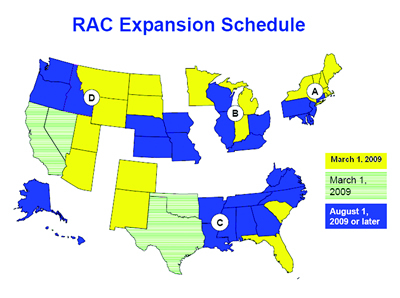
Section 302 of the Tax Relief and Health Care Act of 2006 made the RAC program permanent, and required its expansion nationwide by no later than 2010. CMS is actively moving forward with this expansion. According to its most-recently published “Expansion Schedule,” CMS planned to expand to 23 states by March 1, 2009, and the remaining states by August 1, 2009 or later.2
On October 6, 2008, CMS announced the names of the RAC vendors for the permanent program, and identified the initial states for which each will be responsible:
- Diversified Collection Services, Inc., of Livermore, California is the RAC for Region A, including Maine, New Hampshire, Vermont, Massachusetts, Rhode Island and New York;
- CGI Technologies and Solutions, Inc. of Fairfax, Virginia is the RAC for Region B, including Michigan, Indiana and Minnesota;
- Connolly Consulting Associates, Inc. of Wilton, Connecticut is the RAC for Region C, including South Carolina, Florida, Colorado and New Mexico; and
- HealthDataInsights, Inc. of Las Vegas, Nevada is the RAC for Region D, including Montana, Wyoming, North Dakota, South Dakota, Utah and Arizona.3
More information is available from the CMS RAC website: www.cms.hhs.gov/RAC.
Before the permanent RACs begin auditing, the RACs announced they would hold “Town Hall”-type outreach meetings, at which the RACs and CMS representatives would meet with Medicare providers and suppliers. According to recent conversations this office had with Commander Marie Casey, Deputy Director of the CMS Division of Recovery Audit Operations, Medicare providers and suppliers in the first 23 states can expect automated reviews (electronic review of claims data records that do not involve a review of medical records) to begin at any time. Complex reviews (where medical records are requested) will begin for coding issues in September 2009, and medical necessity reviews will begin in January 2010.
CMS compensates RACs on a contingency fee basis, based upon the principal amount of collection from (or the amount repaid to) a provider. This fee arrangement provides incentive to the RAC to aggressively review and deny claims, including claims that the RAC alleges to be not “medically necessary,” an area containing much subjectivity, and a category of denial often highly disputed by the provider.4 RACs are permitted to attempt to identify improper payments resulting from any of the following:
- Incorrect payments;
- Non-covered services (including services that are not reasonable and necessary);
- Incorrectly coded services; and
- Duplicate services.5
When performing coverage or coding reviews of medical records, nurses (RNs) or therapists are required to make determinations regarding medical necessity, and certified coders are required to make coding determinations. The RACs are not required to involve physicians in the medical record review process. However, the RACs must employ a minimum of one FTE contractor medical director (CMD) (who must be a doctor of medicine or doctor of osteopathy) and arrange for an alternate CMD in the event that the CMD is unavailable for an extended period. The CMD will provide services such as providing guidance to RAC staff regarding interpretation of Medicare policy.
Although the RACs have fairly broad discretion in determining which claims to review, CMS has prohibited the RACs from looking at certain categories of claims. For example:
- The permanent RAC program will begin with a review of claims paid on or after October 1, 2007. This first permissible date for claims review is the same for the RAC reviews in all states, regardless of the actual start date for a RAC in a particular state. However, as time passes, the RACs will be prohibited from reviewing claims more than three years past the date of initial determination (defined as the initial claim paid date).
- RACs are not permitted to review claims at random. However, RACs are authorized to use “data analysis techniques” to identify claims likely to be overpayments, a process called “targeted review.” In the demonstration program, the “targeted review” resulted in certain categories of providers and certain types of claims being subject to more scrutiny than others.6
2. IMPACT OF RAC AUDITS
Over the course of the three-year demonstration, the RACs identified and collected $992.7 million in overpayments and ordered repayment of just $37.8 million in underpayments to Medicare providers and suppliers.7 Thus, approximately 96 percent of the alleged improper payments identified were overpayments, as opposed to underpayments.
3. PREPARING FOR A RAC AUDIT
Medicare providers, including anesthesiologists and pain management physicians, should begin to prepare now for the RACs and increased Medicare auditing activity. Although providers cannot prevent RAC audits from happening, they can prepare for increased claims scrutiny and RAC activity by dedicating resources to:
- Internal monitoring protocols to better identify and monitor areas that may be subject to review (i.e., reviewing compliance guidance documents such as RAC Evaluation Reports, the OIG Work Plan and OIG compliance guidance, and dedicating resources to monitoring compliance risk areas);
- Responding to record requests within the required timeframes;
- Implementing an effective compliance program in accordance with OIG guidelines, and/or strengthening procedures currently in place.
Pursuant to the “Update to the Evaluation of the 3-Year Demonstration,” published in January 2009, “Future improper payments can be avoided by analyzing the RACs’ service-specific findings.”8 Looking to the results of the RAC demonstration program is not particularly illustrative or educational for anesthesia providers and pain management physicians, however. This is because:
- The vast majority of RAC claim denials in the demonstration program involved Part A hospital claims. Eighty-five percent of the claims reviewed in the RAC demonstration program were inpatient hospital claims (e.g., short stays and DRG coding issues);
- Six percent of the claims were inpatient rehabilitation facility claims; 4.25 percent of the claims were outpatient hospital claims;
- Two and one-half percent of the claims were physician claims;
- One and three-quarters percent of the claims were skilled nursing facility claims; and
- One percent of the claims involved DME, ambulance, lab and other services.
Although the historical information regarding RAC denials is not particularly illustrative to anesthesiologists and pain management physicians, there is other program guidance identifying areas of increased claims scrutiny. For example, each year the OIG publishes a Work Plan setting forth various projects to be addressed during the upcoming fiscal year, to which the RACs may look to identify potential areas for their audit activities. In 2008, the OIG Work Plan identified interventional pain management procedures as procedures likely to undergo claims scrutiny for medical necessity. The OIG noted that interventional pain management is a growing specialty, and Medicare paid nearly $2 billion for interventional pain management procedures in 2005.
In addition to the OIG Work Plan, in September 2008, the OIG issued a report on “Medicare Payments for Facet Joint Injection Services.” The report stated that the OIG had found that 63 percent of facet joint injection services allowed by Medicare in 2006 did not meet Medicare program requirements, resulting in $96 million in improper payments.
Although the information from the RAC demonstration program does not provide specific guidance for the anesthesia and pain management industries in terms of strategic planning for the permanent program, taking into account other available guidance, anesthesia and pain groups are well advised to strengthen their compliance programs to ensure that certain anesthesia and pain management focus areas are enhanced. For example, groups should ensure that:
- Each provider is only capturing allowable anesthesia time and that appropriate documentation exists to support the recorded start and end times;
- Compliance with the medical direction requirements is satisfied, including enhancing documentation practices to demonstrate such compliance;
- Documentation practices are improved with regard to separately payable services such as invasive monitoring lines and post-operative pain services;
- Documentation practices are improved with regard to medical necessity documentation in connection with the performance of monitored anesthesia care cases;
- Documentation practices are improved with regard to medical necessity documentation in connection with the provision of chronic pain management procedures; and
- Documentation practices are improved with regard to medical necessity documentation relative to the provision of evaluation and management services.
4. WHAT TO EXPECT IF YOU ARE AUDITED BY A RAC
RACs engage in two types of claim reviews to identify improper payments: “automated review” and “complex review:”
An “automated review” is a review of claims data without a review of the records supporting the claim. Generally speaking, RACs may conduct automated reviews only in situations where there exists both (a) a certainty that the service is not covered or is incorrectly coded, and (b) a written Medicare policy, article, or coding guideline applicable to the claim. RACs also may use automated review, even if there is no specific Medicare policy, article or coding guideline on point, in some “clinically unbelievable” situations9 or when identifying duplicate claims and/or pricing mistakes.10 According to Commander Marie Casey, Deputy Director of the Division of Recovery Audit Operations at CMS, automated reviews of providers in the first 23 states can be expected to begin at any time.
On the other hand, a “complex review” consists of a review of medical or other records, and is used in situations where there is a high probability (but not a certainty) that a claim includes an overpayment.11 In summary, the RAC “complex review” process is as follows:
- RACs are authorized to: (a) visit the provider’s location to view and/or copy medical records or (b) request that the provider mail, fax, or otherwise securely transmit the records to obtain medical records necessary to conduct claim reviews. To “securely transmit” medical records means to send those records “in accordance with the CMS business systems security manual – e.g., mailed CD, MDCN line, through a clearinghouse).12
During the RAC demonstration program, some providers were overwhelmed by the volume of records requests received from the RACs. In the permanent program, CMS imposed limits on the number of records RACs may request per 45-day period.13 For physicians, such as anesthesiologists and pain management physicians, this record request limit is as follows:
- Solo Practitioner: 10 medical records per 45 days
- Partnership of 2-5 individuals: 20 medical records per 45 days
- Group of 6-15 individuals: 30 medical records per 45 days
- Large Group (16+ individuals): 50 medical records per 45 days.14
It is essential that providers timely respond to RACs’ requests for medical records. If a RAC does not receive requested medical records within 45 days, it is authorized to render an overpayment determination with respect to the underlying claim.15 If the provider appeals this type of denial, “the appeals department may, at CMS direction, send the claim to the RAC for reopening under certain conditions…”16 However, the Carrier or Intermediary is not required to send the claim to the RAC for reopening. Thus, providers failing to timely respond to RACs’ medical records requests could lose appeal rights with respect to these claims.
- Once requested medical records are received, the RAC will conduct its review of the claim. In conducting reviews, RACs are required to comply with National Coverage Decisions (“NCDs”), Coverage Provisions in Interpretive Manuals, national coverage and coding articles, Local Coverage Decisions (“LCDs”), and local coverage and coding articles in their respective jurisdictions.17 The RACs also are authorized to develop internal guidelines to assist their reviewers to conduct claims reviews consistently with NCDs and LCDs.18
- Generally speaking, a RAC must complete complex reviews within 60 days from receipt of the requested medical records.19 Following its review, the RAC will issue a letter to the provider setting forth the findings for each claim and notifying the provider of its appeal rights. Alleged overpayments identified by RACs may be appealed through the uniform Medicare appeals process.
According to Commander Casey, complex reviews regarding certain coding issues are planned to begin in September 2009. Complex reviews regarding issues of medical necessity will begin sometime after January 1, 2010.
5. HOW TO APPEAL CLAIMS DENIED BY A RAC
RAC denials are subject to the standard Medicare appeals process set forth in 42 C.F.R. Part 405, subpart I.
A. Stage 1: Redetermination
The first level in the appeals process is redetermination. Providers must submit redetermination requests in writing within 120 calendar days of receiving notice of initial determination. There is no amount in controversy requirement.
B. Stage 2: Reconsideration
Providers dissatisfied with a carrier’s redetermination decision may file a request for reconsideration to be conducted by a Qualified Independent Contractor (QIC). A QIC is a Medicare contractor tasked to complete the second level of appeal (reconsideration level of appeal). This second level of appeal must be filed within 180 calendar days of receiving notice of the redetermination decision. There is no amount in controversy requirement.
Importantly, the QIC reconsideration is an “on-the-record” review, contrary to an in-person hearing review. In conducting its review, the QIC will consider evidence and findings upon which the initial determination and redetermination were based plus any additional evidence submitted by the parties or the QIC obtains on its own.Of particular note, providers must submit a full and early presentation of evidence in the reconsideration stage. When filing a reconsideration request, a provider must present evidence and allegations related to the dispute and explain the reasons for the disagreement with the initial determination and redetermination. Absent good cause, failure of a provider to submit evidence prior to the issuance of the notice of reconsideration precludes subsequent consideration of the evidence. Accordingly, providers may be prohibited from introducing evidence in later stages of the appeals process if such evidence was not presented at the reconsideration stage.
C. Stage 3: Administrative Law Judge Hearing
The third level of appeal is the Administrative Law Judge (ALJ) hearing. A provider dissatisfied with a reconsideration decision or who has exercised the escalation provision at the reconsideration stage may request an ALJ hearing. The request must be filed within 60 days following receipt of the QIC’s decision and must meet the amount in controversy requirement. ALJ hearings can be conducted by video-teleconference (VTC), in-person, or by telephone. The regulations require the hearing to be conducted by VTC if the technology is available; however, if VTC is unavailable or in other extraordinary circumstances the ALJ may hold an in-person hearing. Additionally, the ALJ may offer a telephone hearing.
D. Stage 4: Medicare Appeals Council Review
The fourth level of appeal is the Medicare Appeals Council (MAC) Review. The MAC is within the Departmental Appeals Board of the U.S. Department of Health and Human Services. A MAC Review request must be filed within 60 days following receipt of the ALJ’s decision. Among other requirements, a request for MAC Review must identify and explain the parts of the ALJ action with which the party disagrees. Unless the request is from an un-represented beneficiary, the MAC will limit its review to the issues raised in the written request for review.
E. Stage 5: Federal District Court
The final step in the appeals process is judicial review in federal district court. A request for review in district court must be filed within 60 days of receipt of the MAC’s decision.
6. STRATEGIES FOR APPEALING CLAIM DENIALS
Once a provider receives a claim denial made by a RAC, it is important that the provider aggressively pursue appealing the denial through the Medicare appeals process. Experienced healthcare legal counsel can assist providers with appeals to ensure all available substantive challenges and legal theories are utilized. Experienced counsel will submit an appeal brief/position statement that advocates the provider’s position.
7. CONCLUSION
Medicare providers, including anesthesiologists and pain management physicians, should be ready for increased Medicare auditing activity as the RAC program expands nationwide. Providers should make efforts now to evaluate their compliance with Medicare policy. Should a provider be subject to a RAC or other Medicare audit, effective strategies are available that can be successfully employed in the appeals process to challenge claim denials.
Abby Pendleton and Jessica L. Gustafson are partners with the health care law firm of The Health Law Partners, P.C. The firm represents hospitals, physicians, and other health care providers and suppliers with respect to their health care legal needs. Pendleton and Gustafson specialize in a number of areas, including but not limited to: Recovery Audit Contractor (RAC), Medicare, Medicaid and other payor audit appeals, healthcare regulatory matters, compliance matters, reimbursement and contracting matters, transactional and corporate matters, and licensing, staff privilege and payor de-participation matters. They can be reached at apendleton@thehlp.com and jgustafson@thehlp.com.
1 The Medicare Recovery Audit Contractor (RAC) Program: An Evaluation of the 3-Year Demonstration,” at p. 15, June 2008, available at www.cms.hhs.gov.
2 RAC Expansion Schedule, available at www.cms.hhs.gov.
3 Id. Note that the RAC Expansion Schedule indicates the four RAC regions, labeled A, B, C and D.
4 In a significant change from the demonstration program, under the permanent RAC program, if a provider files an appeal disputing the overpayment determination, and provider wins this appeal at any level, the RAC is not entitled to keep its contingency fee, and must repay CMS the amount it received for the recovery. RAC Statement of Work, available at www.cms.hhs.gov.
5 RAC Statement of Work, available at http://www.cms.hhs.gov/RAC/10_ExpansionStrategy.asp#TopOfPage.
6 Id.
7 “The Medicare Recovery Audit Contractor (RAC) Program: An Evaluation of the 3-Year Demonstration,” at p. 15, June 2008, available at www.cms.hhs.gov.
8 tp://www.cms.hhs.gov/RAC/Downloads/AppealUpdatethrough83108ofRACEvalReport.pdf.
9 A “clinically unbelievable” situation is one where “certainty of noncoverage or incorrectly coding exists but no Medicare policy, Medicare articles or Medicare-sanctioned coding guidelines exist.” In these cases, the RAC may ask CMS to approve automated review. However, unless CMS specifically approves an issue for automated review, the RAC must use complex review to make such determinations. See “Statement of Work for the Recovery Audit Contractor Program” at p. 18, available at www.fbo.gov.
10 Id. at pp. 17-18.
11 Id.
12 Id. at p. 11.
13 Id.
14 See “RAC Medical Record Request Limits,” available at www.cms.hhs.gov
15 See “Statement of Work for the Recovery Audit Contractor Program” at p. 13, available at www.fbo.gov.
16 Id. at p. 20 (emphasis in original).
17 Id. at p. 16.
18 Id. at p. 17.
19 Id. at p. 19.
20 Id. at p. 22.
-
Identity Theft Programs: What Every Anesthesia practice Should Consider Doing Now
Neda Mirafzali
The Health Law Partners, P.C.NEWSFLASH: As of July 29, 2009, the Federal Trade Commission (“FTC”) extended its August 1 deadline to enact the commonly referred Red Flags Rule (16 C.F.R. Part 681) to November 1.
Come November 1, anesthesia practices, among other entities, will be responsible for ensuring patients’ identity protection under the provisions of the Red Flag Rule. Constituting 5% of all identity theft, medical identity theft has gained greater political attention and media coverage; thus, the Red Flags Rule should come at no surprise. According to the FTC, medical identity theft occurs when an individual seeks medical services using another’s name and insurance information. It is not until victims check their credit history or are denied insurance coverage for a medical service for having reached their policy limit that they realize their identity has been stolen and their credit history crushed, taking years to revitalize. Additionally, erroneous medical entries are recorded in the victim’s name producing a fictitious medical history. The recent extension is to give the FTC additional time to “redouble its efforts to educate [entities] about compliance with the ‘Red Flags’ Rule and to ease compliance by providing additional resources and guidance to clarify whether businesses are covered by the Rule and what they must do to comply.” The FTC announced that, in the future, it would make available additional resources and compliance guidance for low-risk entities.What is the Red Flags Rule?
In short, the Red Flags Rule requires particular entities to develop and implement reasonable policies and procedures “appropriate to the size and complexity of the entity” to guard against identity theft. As part of the Fair and Accurate Credit Transactions Act of 2003 (“FACT”), financial institutions and creditors must have anti-identity theft programs in place. According to the FTC, “red flags” are any factors that could indicate identity theft, including identification, detection, and response to patterns, practices, or specific activities. Under the Red Flags Rule, the FTC requires financial institutions and creditors to do the following:
- Identify relevant patterns, practices, and specific forms of activity that are “red flags” signaling possible identity theft and incorporate those red flags into the Identity Theft Prevention Program;
- Detect red flags that have been incorporated into the Identity Theft Prevention Program
- Respond appropriately to any red flags that are detected to prevent and mitigate identity theft; and
- Ensure the Identity Theft Prevention Program (“Program”) is updated periodically to reflect changes in risks from identity theft.
Who Has to Comply with the Red Flags Rule?
The FTC declared that the Red Flags Rule requires each financial institution and creditor that holds any covered account, “to develop and implement an Identity Theft Prevention Program…for combating identity theft in connection with new and existing accounts.”
For physician practices, the relevant definition is that of a creditor. A creditor, as defined in the regulation, is a “person who regularly extends, renews, or continues credit; any person who regularly arranges for the extension, renewal, or continuation of credit; or any assignee of an original creditor who participates in the decision to extend, renew, or continue credit.”
A covered account, as defined in the regulations, is an account “that involves or is designed to permit multiple payments or transactions…and any other account…for which there is a reasonably foreseeable risk to members or to the safety and soundness of the federal credit union from identity theft….”
How Does the Red Flags Rule Apply to Physician practices?
Though many physicians question the reasons why this applies to their practices, the FTC insists that the Red Flags Rule applies to physician practices. Physician practices that accept insurance or allow payment plans are considered creditors as they allow deferred payment until physicians render the services and collect the insurance and other applicable payment owed. As a result, physician practices are subject to the Red Flags Rule.
Even with this definition, however, many physician practices do not agree that they are creditors under the definition of creditor. Thus, the FTC provides examples of why it believes a physician practice is a creditor. For example, a physician practice is a creditor if it “regularly bill[s] patients after the completion of services, including for the remainder of medical fees not reimbursed by insurance.” This language would cover most, if not all, anesthesia practices. Additionally, if a physician practice allows patients to set up a payment plan, the physician practice would be considered a creditor and would, therefore, be subject to the Red Flags Rule.Not all physician practices are required to adopt the Red Flags Rule. Those physician practices that require full payment prior to rendering services are not creditors and are not subject to the Red Flags Rule. Merely accepting credit card payments does not render a physician practice a creditor.
The American Medical Association (AMA) does not agree with the FTC’s position asserting that such position is not “consistent with the intent or scope of the enabling legislation….” To date, the AMA’s protests have not been successful. This is further highlighted by the FTC’s new publication entitled, “The ‘Red Flags’ Rule: What Health Care Providers Need to Know About Complying with New Requirements for Fighting Identity Theft” (www.ftc.gov).
How Can Anesthesia practices Comply with the New Regulations?
Generally, anesthesia practices (“practices”) rely on their respective hospital or facility to gather information on admitted patients. It is important that anesthesia practices check that the hospital or facility has an Identity Theft Program in place that complies with the requirements of the Red Flags Rule and any other applicable state law. practices should coordinate with the facility to adopt applicable portions of the facility program into the practice’s program to assist in meeting its Red Flags Rule obligations.
Administrative Responsibilities
The regulations require certain administrative action and oversight. For example, prior to implementing a program, the practice must have its Board of approve the proposed program. Also, practices must designate a person to be involved in oversight of the program and education of staff. Furthermore, the regulations require that covered creditors take steps to oversee that their service providers, like billing and management companies, conduct business according to the procedures designed to mitigate the risk of identity theft. Accordingly, practices should contact their billing companies and request a copy of their policies/procedures on this topic. As stated above, there are four parts to complying with the Red Flags rules: identifying red flags, detecting red flags, responding to red flags, and ensuring an updated program. Notably, all protocols adopted in compliance with the Red Flags Rule must be in writing.
Identify and Detect
There is no complete enumeration of approved ways to identify medical identity theft. However, the FTC has provided examples of warning signs to look for. Practices should be aware of suspicious documents, suspicious personally identifying information, suspicious activities, and notices from victims, law enforcement, or insurers of possible identity theft. The FTC suggests physician practices ask the following questions:
- Has the new patient given you identification documents that look altered or forged?
- Is the photograph or physical description on the ID inconsistent with what the patient looks like?
- Did the patient give you other documentation inconsistent with what he or she has told you?
- Did the patient give you information that is inconsistent with what is on file?
- Is mail returned repeatedly as undeliverable while the patient still shows up to appointments?
- Does a patient complain about receiving a bill for a service that he or she did not get?
- Is there an inconsistency between a physical examination or medical history reported by the patient and the treatment records?
If one answers “yes” to any of these questions, it would be beneficial to ask for additional information from that patient to ensure the individual’s identity matches the claimed identity. Again, since the practice will likely rely on facility personnel to obtain documentation in the admission process, the practice should ensure that the facility requests and verifies patient identification and resolves any discrepancies as they arise prior to rendering the actual service. In such cases, the practice’s written program should refer to the facility’s written procedures for this verification process and should attach such written procedures.
Respond
After a red flag has been identified and detected, the practice should follow a procedure to respond to the red flags. Responding to red flags could include a plan for gathering documents if there is an incident, a process for reporting the incident to the appropriate personnel, and guidelines to follow for appropriate action (i.e. stopping the admission and billing process, notifying the person whose identity was used, notifying the authorities, assessing the impact on the practice, etc.). In the case of an anesthesia practice, for those flags detected in the facility admission process, the practice would be relying on the facility to take action and coordinate with the practice. Again, the practice’s written program would need to record that the facility’s procedures for identifying and responding to issues have been adopted by the practice. For those issues identified after the service has been rendered, but during the billing process, the practice would need to make sure that the billing process has been halted and that appropriate action is taken.
This must be included in the practice’s written program.
Ensure
While this program is in place, it is important for practices to continuously update the practice’s procedures to ensure that they are consistent with most recent updates and developments surrounding medical identity theft.
State law
In addition to addressing the FTC regulations, practices should also check state law for any requirements related to this topic. For example, some states have enacted laws protecting social security numbers. State law requirements can easily be incorporated into the practice’s written Identity Theft Program. The local or State medical society is a good place to begin researching state law.
Summary
Though there are no criminal ramifications for failing to comply with the Red Flags Rule, there are financial penalties for non-compliance, including a $2500 fine for each known violation. For those practices who need assistance in developing their written program, a qualified healthcare law firm can help. For additional guidance, please visit the FTC website at www.ftc.gov and the FTC’s guidance to healthcare providers, www.ftc.gov/bcp/edu/pubs/articles/art11.shtm.
Neda Mirafzali is a third year law student at Michigan State University College of Law. She wrote her article while working as a law clerk at The Health Law Partners, P.C. The firm represents hospitals, physicians, and other health care providers and suppliers with respect to their health care legal needs.
-
Relevance of LLCs to Anesthesia Practice: How Well Do They Protect the Founders' Income?
Aaron H. Sherbin, Esq.,
Jaffe, Raitt, Heuer & Weiss P.C.
Andrew B. Wachler, Esq.,
Wachler & Associates P.C.Anesthesiologists may want to consider organizing their practice as a professional limited liability company (PLLC). The PLLC offers distinct advantages to other forms of business entities, while offering substantially the same limited liability benefits. This article will discuss how a PLLC provides limited liability to its owners, the nature of the tax treatment of a PLLC, the governance of a PLLC, and the admittance and withdrawal of a member of a PLLC.
PLLCs are governed by state statute. Most, but not all, states recognize and permit professionals to organize as a professional limited liability company. Certainly, any anesthesiologists interested in organizing as a PLLC should consult with their tax and legal advisor about whether or not their state permits PLLCs and how they are governed as well as how the PLLC and its members are taxed.Specific limited liability statutes will vary slightly from state to state. However, the following general rules apply throughout the country. In a PLLC an individual member is liable for his or her own negligent or wrongful acts as well as for those same types of acts committed by individuals under his or her control or supervision. For example, in a PLLC, an individual member would likely be responsible for his or her own medical malpractice or overpayment liability only to the extent that he or she performed or supervised the services at issue. In contrast, in a partnership, each partner would be liable for the negligent acts of all other partners. A PLLC’s liability is also limited in the sense that the member’s personal assets are protected against the debts and liabilities of the PLLC.
For federal tax law purposes, a PLLC is treated as a partnership. As a result, the PLLC does not pay an entity level tax; rather, the profits are generally allocated to the members of the PLLC pro rata and the members will report their share of the profits on their individual income tax returns. This tax treatment is in contrast to a C-corporation where the corporation pays a tax on the profits at the corporation level and the shareholders pay a second tax on any dividends distributed to them by the corporation.
As a partnership, PLLCs offer a tremendous amount of flexibility in ownership interest in the PLLC and in how profits and losses may be allocated among members. Also, there are no restrictions as to the type of owner or number of owners of a PLLC. S-corporations, on the other hand, offer some of the same tax benefits as a PLLC, but have limitations on who may be a shareholder as well as limitations on the number of shareholders. For instance, only citizens or residents of the United States can be a shareholder of an S-corporation. In addition, an S-corporation may have only one class of stock, and thus, allocating profits among its shareholders based upon some metric or formula that deviates from shareholdings is not permitted. The effect of having an ineligible shareholder or a second class of stock is that the corporation will lose its S-status and be taxed as a C-corporation which could potentially result in disastrous tax ramifications.
Generally, owners/members of a PLLC cannot be considered employees of the PLLC. They must be treated as self-employed and, as a result, distributions received by a member of the PLLC are subject to self-employment tax. This may result in a member paying slightly higher income tax on his or her share of the profits than the member would have had he or she received the distribution in the form of wages.
Since the PLLC offers incredible flexibility with regard to who can be a member and how profits and losses are allocated, the PLLC provides various options for the admittance or withdrawal of a member. However, there may be different tax consequences depending on the assets owned by the PLLC and how the buyout of a withdrawing partner is structured. A withdrawing member may have to recognize ordinary income (as opposed to capital gains) on the buyout proceeds received depending upon whether the PLLC has account receivables and inventory and whether the buyout of the member is by the PLLC itself or by the other members.
PLLCs are not required to have the rigid structure associated with corporations. In other words, PLLCs do not need to have officers and directors governing their operations. A PLLC can be managed by its members (or owners) or by managers who may be a select group of the members or non-members. A PLLC is typically governed by an operating agreement, which usually includes provisions regarding how and when members meet, the power of a member to bind the PLLC, the required vote of members, the treatment of profits and losses, how and when additional capital will be required and by whom, and what is to happen in the event of the death, disability, retirement or termination of employment of a member. Members of a PLLC can tailor their operating agreement to fit their particular practice.
In summary, PLLCs protect the founders’ personal assets as well as do other corporate forms such as professional corporations, but they offer flexibility and tax advantages that may not be available with other forms. Before deciding on a corporate form, anesthesiologists should consult with experienced legal counsel and accountants.
Andrew B. Wachler is the principal of Wachler & Associates, P.C. Mr. Wachler has been practicing healthcare and business law for over 25 years. He graduated Cum Laude from the University of Michigan in 1974 and Cum Laude from Wayne State University Law School in 1978. Mr. Wachler is a member of the State Bar of Michigan, Health Care Law Section, American Bar Association, Health Care Law Section, Member of “The Health Lawyer” Editorial Board and the American Health Lawyers Association. Mr. Wachler can be reached at awachler@wachler.com.
Aaron H. Sherbin is an attorney with Jaffe, Raitt, Heuer & Weiss, P.C. and is a member of the firm’s Tax and Estate Planning Groups. His practice areas include Federal Tax Law, Business Planning, Business Mergers and Acquisitions, Estate Planning, Estate Administration and Probate Litigation. Aaron earned his B.B.A. from the University of Michigan in 1985, his J. D., cum laude from Wayne State University Law School in 1988, and his LL.M in Taxation from New York University Law School in 1989. Mr. Sherbin can be contacted at asherbin@jaffelaw.com.
-
How Anesthesia Groups Thrive, Not Simply Survive
Mark F. Weiss, J.D.
Advisory Law Group, Los Angeles, CAYou’re building a house . . . well, your contractor is. He tells you that he’ll start by pouring the concrete foundation and then put on the roof, after which he’ll put up the exterior walls, followed by the chimney.
It’s easy to see the folly in building a home in that manner. But when an anesthesia group builds its practice in a similar manner, it usually goes without comment, even without notice.
“We need to address the issue of renewing our exclusive contract. It expires in July,” a partner says in May.
“We’re not able to retain our subcontractors. They’re leaving for better pay,” says another partner in August, after the exclusive contract has renewed.
“The surgeons are complaining about turnover time,” states a partner in September.
“We really need financial support from the hospital,” says a partner in October.
Just as in our analogy to home building gone awry, anesthesia groups often consider the instances of practice building, such as exclusive contracts, subcontracts and employment agreements, billing and collection activities, data management, and stipends, as separate projects, to be addressed on a piecemeal basis.The secret to anesthesia group success, in any economy, starts with the realization that these are not separate instances at all. In order for your group to thrive, they must be linked together with strategy.
The Strategic Group
In order to succeed at the highest plane, your group must become strategic on multiple levels. It must develop an overall business strategy. It must then develop substrategies for each particular instance previously thought to be independent, e.g., an exclusive contracting strategy and a data management strategy, that are consistent with the group’s overall business strategy and which take into account the interrelationship among the various substrategies. Finally, just as the strategies are aligned, the tactics employed in furtherance of each of the particular substrategies must also be coordinated.
Leadership
Beyond the smallest of groups, two or three physicians, leadership cannot be by consensus or paralysis will set in. Successful groups must have leaders and leaders must be allowed the time required to lead and the ability to fail without fear of retribution.
Just as leaders need this freedom, group members are owed faithful performance: If your homebuilding contactor told you that he was too busy to pay attention to the organization of the job because he was spending all day hammering nails, you’d think about getting a new contractor. But most groups aren’t fazed when their “leader” essentially uses the same excuse, or when they guarantee the same result by tying his hands to a full share of patient care responsibility.
Give Me a Lever Long Enough . . .
Successful groups understand that they must create leverage. By having options to the deal, in respect of facility contracts, in respect of contracts with employed or subcontracted physicians, and in respect with their relationships with other third parties, they create tremendous negotiating leverage.
In particular, in connection with their exclusive contracting relationships, they avoid the most significant mistake a group can make: permitting the hospital to believe that the group’s mere existence turns on the hospital’s decision to grant or renew the exclusive contract.
Framing the Issues
Despite compliance issues, facts and budgets, emotion plays a leading role in decision making. Not only is telling the better story essential, choosing the theme of the story is required.
Relationships and negotiations, just like conversations, do not take place in a vacuum; they take place in a context or “frame.” Understand that there’s a battle on the meta level to frame the issues and that winning it can determine the outcome of the more observable conflict.
Touch Points
Successful groups understand that negotiation is not something that happens only in a boardroom. Each touch point with hospital administration, with other members of the medical staff, and with patients and their families is actually an element of the process of building support for your group’s positions. Everyday interactions impact upon the group’s image. In order to advance the group’s interests, you must control or influence as many of those touch points as possible.
It’s About Time
Although quick results in respect of certain elements of a group’s strategy are obtainable, achieving a transformational result for an existing group requires a long term view, optimally several years. After all, the goals are long term: group and member physician success. An understanding, in fact, an expectation that it will take time and effort to achieve those results is necessary and required.
But It’s Not About a Timeline
Progress in positioning your group to achieve maximum power in its relationships, and, therefore, in its negotiating posture, is not a linear process. As discussed above, the process involves an ongoing series of interrelated strategies and tactics. Each of these elements, once started, continue. In duality, each is both independent and dependent: Independent in that each element is focused on a particular goal; dependent in that each strategy and tactic supports the others in achieving the group’s overall business goal. Instead of the image of a timeline, picture instead an atom: Each of the electrons revolves independently, but they all revolve around the nucleus.
Beingness vs. “Gettingsomewhereness”
The problem most often preventing anesthesia groups from thriving is “beingness.” (No, this is not a metaphysical discussion.) They simply “are.” They exist to exist – to “serve” the hospital.
I suggest that the better route is for your anesthesia groups to exist to serve itself, to move from beingness to “gettingsomewhereness,” with that somewhere being of your own design.
Yes, plans go awry and no one can guarantee that there won’t be challenges to the strategy along the way. In fact, there will be countless small and major challenges thrust at you in countless ways. But the beauty of a strategic outlook consisting of interlocking processes is its flexibility while still guiding you to your envisioned future. The foundation may have to be shored up, the walls may have to be reinforced or allowed to sway to compensate for earthquakes, but you’ll end up with a house, not simply with a roof sitting on a slab of cement.
Mark F. Weiss is an attorney who specializes in the business and legal issues affecting anesthesia and other physician groups. He holds an appointment as clinical assistant professor of anesthesiology at University of Southern California’s Keck School of Medicine and practices nationally with the Advisory Law Group, a firm with offices in Los Angeles and Santa Barbara, CA. Mr. Weiss provides complimentary educational materials to our readers. Visit www.advisorylawgroup.com for his free newsletter. He can be reached by e-mail at markweiss@advisorylawgroup.com.
 Importantly, the QIC reconsideration is an “on-the-record” review, contrary to an in-person hearing review. In conducting its review, the QIC will consider evidence and findings upon which the initial determination and redetermination were based plus any additional evidence submitted by the parties or the QIC obtains on its own.
Importantly, the QIC reconsideration is an “on-the-record” review, contrary to an in-person hearing review. In conducting its review, the QIC will consider evidence and findings upon which the initial determination and redetermination were based plus any additional evidence submitted by the parties or the QIC obtains on its own. Come November 1, anesthesia practices, among other entities, will be responsible for ensuring patients’ identity protection under the provisions of the Red Flag Rule. Constituting 5% of all identity theft, medical identity theft has gained greater political attention and media coverage; thus, the Red Flags Rule should come at no surprise. According to the FTC, medical identity theft occurs when an individual seeks medical services using another’s name and insurance information. It is not until victims check their credit history or are denied insurance coverage for a medical service for having reached their policy limit that they realize their identity has been stolen and their credit history crushed, taking years to revitalize. Additionally, erroneous medical entries are recorded in the victim’s name producing a fictitious medical history. The recent extension is to give the FTC additional time to “redouble its efforts to educate [entities] about compliance with the ‘Red Flags’ Rule and to ease compliance by providing additional resources and guidance to clarify whether businesses are covered by the Rule and what they must do to comply.” The FTC announced that, in the future, it would make available additional resources and compliance guidance for low-risk entities.
Come November 1, anesthesia practices, among other entities, will be responsible for ensuring patients’ identity protection under the provisions of the Red Flag Rule. Constituting 5% of all identity theft, medical identity theft has gained greater political attention and media coverage; thus, the Red Flags Rule should come at no surprise. According to the FTC, medical identity theft occurs when an individual seeks medical services using another’s name and insurance information. It is not until victims check their credit history or are denied insurance coverage for a medical service for having reached their policy limit that they realize their identity has been stolen and their credit history crushed, taking years to revitalize. Additionally, erroneous medical entries are recorded in the victim’s name producing a fictitious medical history. The recent extension is to give the FTC additional time to “redouble its efforts to educate [entities] about compliance with the ‘Red Flags’ Rule and to ease compliance by providing additional resources and guidance to clarify whether businesses are covered by the Rule and what they must do to comply.” The FTC announced that, in the future, it would make available additional resources and compliance guidance for low-risk entities. Even with this definition, however, many physician practices do not agree that they are creditors under the definition of creditor. Thus, the FTC provides examples of why it believes a physician practice is a creditor. For example, a physician practice is a creditor if it “regularly bill[s] patients after the completion of services, including for the remainder of medical fees not reimbursed by insurance.” This language would cover most, if not all, anesthesia practices. Additionally, if a physician practice allows patients to set up a payment plan, the physician practice would be considered a creditor and would, therefore, be subject to the Red Flags Rule.
Even with this definition, however, many physician practices do not agree that they are creditors under the definition of creditor. Thus, the FTC provides examples of why it believes a physician practice is a creditor. For example, a physician practice is a creditor if it “regularly bill[s] patients after the completion of services, including for the remainder of medical fees not reimbursed by insurance.” This language would cover most, if not all, anesthesia practices. Additionally, if a physician practice allows patients to set up a payment plan, the physician practice would be considered a creditor and would, therefore, be subject to the Red Flags Rule. PLLCs are governed by state statute. Most, but not all, states recognize and permit professionals to organize as a professional limited liability company. Certainly, any anesthesiologists interested in organizing as a PLLC should consult with their tax and legal advisor about whether or not their state permits PLLCs and how they are governed as well as how the PLLC and its members are taxed.
PLLCs are governed by state statute. Most, but not all, states recognize and permit professionals to organize as a professional limited liability company. Certainly, any anesthesiologists interested in organizing as a PLLC should consult with their tax and legal advisor about whether or not their state permits PLLCs and how they are governed as well as how the PLLC and its members are taxed. Just as in our analogy to home building gone awry, anesthesia groups often consider the instances of practice building, such as exclusive contracts, subcontracts and employment agreements, billing and collection activities, data management, and stipends, as separate projects, to be addressed on a piecemeal basis.
Just as in our analogy to home building gone awry, anesthesia groups often consider the instances of practice building, such as exclusive contracts, subcontracts and employment agreements, billing and collection activities, data management, and stipends, as separate projects, to be addressed on a piecemeal basis.