eAlerts
-
Anesthesiologists and the World of ASCs: A Different Value Proposition
Stanford Plavin, MD
Technical Anesthesia Strategies and Solutions, Atlanta, GA
As the business of anesthesia continues to evolve and the disruptions to our profession and our identities morph, the role of the physician anesthesiologist in the ambulatory surgical center (ASC) realm is ripe with opportunity. ASCs and office-based surgery centers have a vast array of business ownership models and infrastructures that provide the anesthesiologist the chance to impact the delivery and profitability of these models on so many levels in addition to provision of our anesthesia services.
ASC environments present many different challenges for the “typical” anesthesiologist, leading us to the following list of ten top reasons (in reverse order of importance) why anesthesiologists don’t always succeed in this practice setting:
- Everyone is replaceable...it's not like it is a hospital group!
- But the in-network rates are too low. I don’t want to participate in the plans with which the ASC contracts.
- Marketplace consolidation and entitlement...I am part of the hospital network.
- Lack of self-awareness.
- Goals are not aligned with facility and ownership of the center.
- Inconsistencies among providers and skill sets.
- Inflexibility and obstructionist nature of provider.
- Lack of emotional investment in the center.
- Not customer-centric and consumer driven.
- It’s just outpatient and it’s easy… “I’m almost ready for retirement.”
The bridge between success and failure is Communication, which raises at least the following three questions:
- How does the anesthesia group identify the needs specific to each ASC or practice site?
- What can a group or provider do in order to tighten up the relationship?
- How do we learn to engage the facility and the ownership group?
We as providers always seem to feel that we are doing an excellent job but sometimes we lack the insight and data necessary to properly evaluate our performances. This is a potential death knell. Physicians by nature are traditionally challenged to be humble. Our personalities tend to see ourselves as loved and liked by all of those around us. Little do we know, this is typically not the case; and in the ASCs, which are smaller practice settings, our character flaws and technical shortcomings tend to be magnified.
How do we identify what our customers need? We must first identify our customers and unfortunately this seems to be changing on a regular basis. In the ASC realm, who are the decision makers and are they our customers? This varies as well depending upon the ownership and governance structure of the facility. There are tools available to us that we should strongly consider.Surveys and executive summaries are not inexpensive if properly constructed— but they provide tremendous insight and analysis regarding the needs and wants of our various customers.
Carefully constructing the survey is of the utmost importance. Take the time and resources necessary to ensure that you will get the information needed to provide the answers that you want. It does the practice no good to spend a ton of money and energy to survey your customers if you aren’t going to take the time and energy to identify the “value proposition.”
Consider the following when putting together a target survey: evaluating the anesthesiologists and care team, communication, preparation/facilitation, services provided, business relationship and overall satisfaction which targets a number of key components.
Also, leave opportunities to identify unique characteristics and those items which are both positive and negative about your practice and practitioners. Please provide this survey to your own group of providers and discuss the findings as they relate to those of your customers.
Statistics and data analysis. After completing your assessment and survey, what is next? Take the time to carefully analyze the information and put together a summary of your data points. Identify and prioritize the areas of strength as differentiators and, more importantly, identify your areas of weakness and vulnerability.
Extracting the data and information and putting them into a context to be shared amongst your colleagues is of paramount importance. This can truly define your strategic plan moving forward.If constructed correctly, surveys and summaries can help one identify the value proposition of their customers. You can see the criteria that most correlate to the overall satisfaction of your segmented customer base and compare that to what you as the group may have identified as of importance. The results will likely surprise you.
Investing in oneself and stepping outside of the comfort zones that we traditionally have as providers will enable us to identify opportunities for ourselves.
In the world of ASCs, the microscope is powerful and the lights are bright. We cast a big shadow; it is challenging to overcome poor outcomes and quality or to hide that one provider who just doesn’t fit the mold. Be part of the solution and the team; put together a strategy for your practice which can make you as indispensable as possible. Nothing is a panacea, but look for the perioperative solutions that can define your value proposition.
Our scope of services should begin before a patient even sets foot inside of a facility; take them through the full operative/ procedural course and provide a postoperative piece that can be tied to our service line.
I have identified the following P Factors, a nomenclature that puts the “P” into value proposition:
- Patient: patient-centered care
- Perioperative: seek to have an impact in all three components (pre/ intra/post)
- Process: identify areas that we can impact and impart
- Professionalism/Personality
- Procurement: consider an ancillary component to add to your product line
- Performance: affect outcomes, satisfaction, throughput
- Profitability: a likely result of the previous factors
The factors required for success in the ASC environment are numerous and require constant evaluation and are ever-changing. No one P-factor alone is any guarantee of success or failure. The above is merely an introduction to those ideas and offerings that you need to consider embracing in order to define your own value proposition and the unique qualities that you can offer as a practice.
Stanford R. Plavin, MD has been actively involved in the ASC arena for 18 plus years as a practicing anesthesiologist serving as past president of the Georgia Society of Ambulatory Surgical Centers and currently an Ambulatory Surgery Center Association board member. He practices in Atlanta, GA as a co-founder of Ambulatory Anesthesia of Atlanta and can be reached at splavin@technicalanesthesia.com. -
The Only Constant In Healthcare Is Change
The specialty of anesthesiology, and indeed all of health care, is somewhere in the middle of its long transition away from a volume-driven cottage industry. Details of the destination are not yet clear, but one change of which we can be confident is the shift away from in-hospital care toward outpatient settings. Nearly two-thirds of procedures are now performed on an ambulatory basis. With the advent of more and more minimally invasive techniques— not to mention ever-safer anesthesia—that proportion will continue to grow.
Stanford Plavin, MD gives us a window into the mindset necessary for anesthesiologists to succeed in the ambulatory surgical center (ASC) environment, where “the microscope is powerful and the lights are bright” and where even the identity of our customers is changing. “What do the ASC’s customers want?” he asks in Anesthesiologists and the World of ASCs: A Different Value Proposition. Dr. Plavin recommends surveys to identify their satisfaction with the anesthesiologists and nurses and with the services provided. Surveys can help to identify the strengths and weaknesses of the ASC and point toward the factors that contribute the most heavily to success, in the process giving direction to the practice’s strategic plan. The results of well-executed surveys will often come as a surprise.
“Succeeding” takes on a different meaning when used in the context of leadership transitions. That is the meaning used in Jody Locke’s article Lack of Succession Planning: Problem or Symptom. To meet the challenges of all the changes driving the practice of medicine in general and anesthesiology in particular, solid leadership is imperative. It cannot be left to chance; hence the need for succession planning. The traditional culture of many anesthesia practices is more like that of “professional fraternal organizations” than that of enterprises that take active charge of their own future. Leadership involves long-term responsibility for the actions of others, something that is not emphasized in training. Any organization that hopes to continue even after the departure of current leaders must engage in succession planning. Succession planning starts with three fundamental questions: (1) how does the group identify good potential leaders? (2) How does it ensure their preparation for the role? And (3) how does the organization manage continuity when a leader is replaced? Every group should be exploring these and the other questions raised by Mr. Locke.
Another form of change occurring with considerable frequency is the merger of anesthesiology groups. We are happy to welcome Will Latham, MBA, CPA back to these pages and to include his guide to the merger process, Anesthesia Group Mergers: Strategies for Success. This article is a keeper for any group going through a merger today—or possibly in the future. The 14 steps and the list of key issues addressed in the typical merger process can serve as a roadmap, especially when they are read in conjunction with the “pitfalls to avoid” such as “dueling attorneys”—attorneys representing the party that has engaged them, seeking the best deal for that party. The quest for advantage may torpedo the entire negotiation process. The need to advocate for the combined (post-merger) entity should be in the consciousness of every party interested in the merger’s going forward.
Jerry Ippolito, MBA, MHSA outlines an important avenue for adapting to changing hospital relationships in Chronic Pain Management: An Overlooked Opportunity to Financially Partner with Your Hospital & Preserve Your Contract. While many hospital administrators do not think of pain medicine as an attractive source of revenue, this can be very-shortsighted. Mr. Ippolito shows how “comprehensive pain management programs that are strategically positioned, energetically developed and well run can attain strong profitability within a relatively short time.” In fact, anesthesiologists contemplating setting up independent chronic pain practices ought to factor in the potential damaging effects of “denying the hospital the opportunity to generate additional revenue.”
What about making the best possible decisions to manage your anesthesia practice here and now? Some change in our professional lives is driven by internal, not external forces; improved financial reporting should be considered by any group that has less than total confidence in its reporting systems (and perhaps by others as well). Gregory Zinser gives a rundown of the essential financial reports, and of the format of those reports, that will “facilitate review, understanding and discussion” in his article Numbers Don’t Lie, but…
Also in this issue of the Communiqué are articles by regular staff contributors Darlene Helmer (The Trend Toward Code Consolidation) and Joette Derricks (Reviewing Anesthesia and Pain Management 2014 CERT Data to Improve Documentation and Revenue). In these two articles, Ms. Helmer and Ms. Derricks continue their mission of presenting current information that will keep readers abreast of changing codes and documentation requirements.
We hope to see many of you at the Advanced Institute for Anesthesia Practice Management (AIAPM) which we are presenting jointly with Tulane University Health Sciences Center and Medical Business Solutions, LLC at the Cosmopolitan Hotel in Las Vegas on April 17 through 19, 2015. If you are unable to attend, please watch your electronic mailboxes in July for highlights from the talks—and plan to join us for the next AIAPM in April 2016. As always, it will be our privilege to continue expanding the specialty’s practice management knowledge base whether face-to-face or through these pages.
With best wishes,
Tony Mira
President and CEO -
Chronic Pain Management: An Overlooked Opportunity to Financially Partner with Your Hospital & Preserve Your Contract
Jerry Ippolito, MBA, MHSA
President, OR Efficiencies, LLC, Naples, FLAs anesthesiology’s private practice setting continues to change, the financial landscape appears more threatening than ever. More and more private practice groups are having to defend their longstanding hospital contracts to requests for proposals (RFPs). Relationships between anesthesia groups and their aligned hospitals, which have spanned decades, are being undermined by deteriorating medical practice and hospital finances. Hospitals are issuing RFPs and subsequently awarding contracts to national anesthesia practice management companies—akin to Home Depot coming into the community and forcing out the Ace Hardware store. In order to survive and effectively defend their contracts, private practice anesthesiology groups must strategically refocus and realign their relationships with partner hospitals. Anesthesiology groups must go into the hospital board room bringing value and presenting opportunities to assist hospitals to increase income— NOT simply ask for a larger stipend! An effective chronic pain management program is driven by anesthesiology, can add millions to a hospital’s bottomline and can easily offset anesthesiology stipends required to support the traditional hospital anesthesia program.
In the frequently heard and paraphrased words of one of our esteemed colleagues:
“Medicine is a Science; Surgery, Anesthesiology, and Nursing are disciplines; Healthcare is a Business” – Amr Abouleish, MD (UTMB)
As a growing number of hospitals face negative profit margins, and the true financial ramifications of the Affordable Care Act are yet unrealized, hospitals’ finance leaders are examining ways to expand revenue generating services. An effectively developed and comprehensive chronic pain management program can contribute millions of dollars to a hospital’s bottom-line revenue.
The Institute of Medicine reported that chronic pain affects 116 million adults in the U.S. The American Academy of Pain Medicine has indicated that the financial impact of chronic pain on the US economy is greater than diabetes, heart disease and cancer combined. As the population ages, yet remains physically active, the demand for pain management services will continue to grow. Many hospital administrators consider pain management a poor source of revenue. In fact, however, leading hospitals have found that comprehensive pain management programs, that are strategically positioned, energetically developed and well run can attain strong profitability within a relatively short time. Specifically, these programs can:
- Contribute large amounts to the hospital’s bottom line. In a mature practice employing one pain physician, annual revenue from facility fees alone can range from $2.5 million to $3 million. Revenue from professional fees represents another $1 million. Overall program profitability can and will range from three to four times the physician’s income.
- Generate sizable ancillary revenue from hospital services that support the pain practice, such as physical therapy, radiology, lab and behavioral medicine.
- Establish a new source of referrals for surgical services—such as orthopedic surgery and neurosurgery—that are independent of traditional referrals from primary care physicians and can generate additional OR revenue.
- Support key relationships with surgeons, anesthesiologists and other physicians.
While these financial results are within reach for most organizations, creating a strong pain management center takes careful planning and effective execution. Eight key characteristics are shared by the most effective and profitable programs:
- Demographic and Market Opportunity: Typically a population of 25,000 nongovernment-insured patients is required to support a successful one physician chronic pain practice. This number can vary depending on payer mix and payer contracts. In many markets, there is an opportunity to absorb market share beyond existing need. Survey primary care physicians and surgeons (especially orthopedic surgeons) on where they refer patients requiring pain management. A hospital-based program that offers comprehensive pain services has an opportunity for competitive differentiation and growth.
- Strategic Location: Pain management has a strong “consumer” dynamic, so convenience and ease of access are important. Ideally, a pain management program will be located in the hospital’s outpatient department or ambulatory surgery unit, accessed by an entrance separate from the main hospital entry.
- Reimbursement: In most instances, a hospital-based fee schedule provides the highest level of reimbursement. However, locating the pain center on the hospital campus is not the only option. According to Centers for Medicare & Medicaid Services (CMS) guidelines, an offsite facility can be reimbursed under the hospital- based fee schedule if it is within 35 miles of the hospital proper and meets other requirements that usually include the center operating under the hospital’s license. A pain center could also be located in a non-hospital based ambulatory surgery center (ASC). Planners should carefully analyze reimbursement under an ASC fee schedule and verify the impact on revenue. It needs to be recognized that CMS is beginning to review their criteria for hospital-based reimbursement programs. CMS has realized that the existing criteria are not an incentive to contain/reduce costs, nor an incentive to move patient care services to lower cost, non-hospital, ambulatory settings.
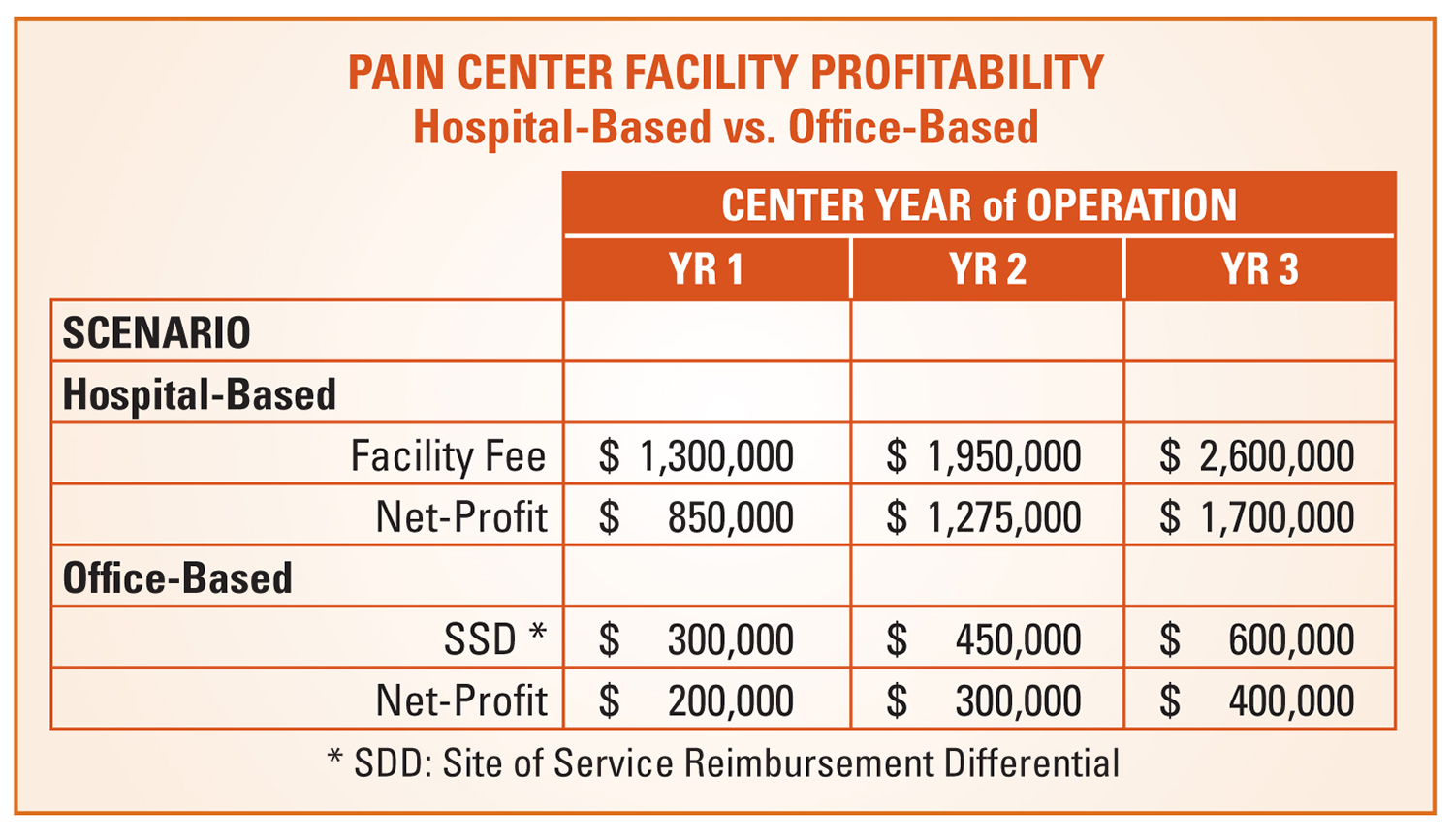
Anesthesiologists may be inclined to develop a private office-based center that is independent of the hospital. There are two significant reasons to put that idea aside: - Office-based services do not receive a facility fee but only a small site-of-service differential (SSD) which is a premium reimbursement payment for professional service fees. This financial comparison is demonstrated in the example provided under the heading “Hospital-Based Versus Office-Based Reimbursement” on page 13.
- Developing the center based location, and denying the hospital the opportunity to generate additional revenue (even worse, potentially diminishing existing hospital revenue sources) will only contribute to the deterioration of your group’s relationship with the hospital. This will NOT be a value-add for your group.
- Comprehensive Scope of Services to Optimize Reimbursement: A full spectrum approach to pain management is not only critical to connecting with patients, but it is also important to the financial success of a pain management program. Procedures provide the greatest reimbursement for both the physician and the facility. Common pain management procedures include:
- Nerve blocks
- Trigger point injections
- Epidural injections
- Fluoroscopy procedures
- Stimulator insertions
- Patients’ evaluation and management (E&M) visits reimburse both the professional and facility fee at reduced or nominal levels. The pain physician receives nominal reimbursement for E&M services and the facility fee, which the hospital benefits from, is reduced or potentially denied unless visits are conducted by a licensed professional such as a nurse (RN), a physician assistants (PA) or a certified nurse practitioner (CNP). Typically, in instances where the non-physician professional cannot bill independently (e.g., RNs) that professional must be employed by the facility (not the physician/anesthesia practice) in order for the facility fee to be paid. Moreover, even in states where PAs and CNPs can bill independently, some payers will deny payments for these professionals’ E&M services. These reimbursement nuances for E&M visits simply exemplify the reimbursement variability involved in collecting for pain management services. Hospitals and anesthesia practices must fully understand and negotiate pain management services payer contracts on a payer-by-payer basis. Where payer contracts are not specifically negotiated, payers can and will pay what they want to, and payers believe it is their duty to deny claims unless specifically provided for in contracts.
- Sizable hospital revenue can be generated from the referral of patients to support services that are an integral part of a comprehensive program, such as:
- Physical therapy for patients suffering from joint pain,
- Nutritional counseling for overweight patients with back pain and,
- Behavioral counseling for patients who require lifestyle changes to progress and sustain relief. Tracking referrals to these services helps validate the ROI of the pain program.
- Well-trained, Strongly-motivated Physicians: To provide comprehensive services, an anesthesiologybased pain program should be led by an anesthesiologist who is fellowship- trained in pain medicine. The most successful pain centers are built around an anesthesiologist who is boarded in both anesthesiology and pain management. It is also important that the anesthesiologist have an entrepreneurial attitude, a strong work ethic and a financial incentive because practice volume drives hospital and program revenue. Successful programs use a productivity- based compensation plan. One possibility is to offer a guaranteed base salary during the first year, with compensation increasing to a higher incremental percent of collections in year two and three.
- Focused Marketing: Use a two-pronged marketing approach to target patients and referring physicians. Patient marketing efforts should focus on active baby boomers and position pain management as “a medical alternative to surgery.” The pain physician needs to make personal visits to referring physicians to introduce him or herself and market the practice. The pain physician can also develop referrals through lectures to the hospital medical staff and informational luncheons organized for community physicians and their office personnel.
- Efficiency and Optimized Throughput: The pain physician should focus his or her time on performing procedures and consulting with new patients. With the exception of some longer procedures, a pain physician should be able to see one patient every 15 minutes. In a mature practice, a PA will be able to handle most follow up E&M visits. These volume and throughput requirements call for an enhanced office layout. Three exam and procedure rooms are typically not enough. Most programs require five or six rooms to maintain patient flow for both the physician and the PA.
- Effective Billing and Collections: The first important step is to negotiate satisfactory contract rates for key procedures with your organization’s top nongovernment payers. Absent contract rates, payers generally reimburse pain services at the lowest possible level and as previously indicated, payers believe it is their job to deny claims. Further, it is paramount for both the anesthesia group and hospitals to engage professionals highly experienced and effective in the discipline of chronic pain billing as:
- Optimized billing and collections are critical to a center’s financial success, and
- Chronic pain programs continue to be highly scrutinized by both payers and the OIG with regard to billing fraud.
Hospital-Based Versus Office-Based Reimbursement
The example in the table above indicates both the level of a pain program’s potential profitability and the differences of profitability depending on the center’s facility base. The example summarizes a pro-forma developed for a major southeastern health system’s chronic pain management program. Hospitals have found that comprehensive pain management programs that are strategically located, energetically developed and well run can attain strong profitability within a two to three year period.Financial projections were based on the following assumptions:
- A single anesthesiologist pain practice supported by a PA;
- Payer-mix skewed towards “government- pay” at below average reimbursement levels due to the prevalence of military health plans in the market (most successful programs will demonstrate even higher levels of profitability);
- Professional revenue and physician compensation are the same under both scenarios, and
- Profitability does not reflect any allocations of indirect costs, or additional revenue, from ancillary service volume (radiology, physical therapy, etc.) and surgical referrals.
Summary:
We are in an anesthesia environment where individual practices find it increasingly necessary to ask hospitals for higher and higher financial stipends as a result of anesthesia program deficits. These deficits can, and do, easily approach one million dollars or more. An aggressive and proactive anesthesiology group, that is sincerely interested in financially partnering with its aligned hospital, can offset anesthesia program deficits by assisting hospitals to develop new programs and additional sources of revenue. Development of an effective chronic pain management program is only one of these opportunities.
Jerry Ippolito, MBA, MHSA is President of OR Efficiencies, LLC, Naples, FL. OR Efficiencies, LLC is a management consulting firm specializing in assisting hospitals and ASCs to improve their perioperative services and anesthesiology programs. Mr. Ippolito can be reached at ippolito.orefficiencies@gmail.com. -
Anesthesia Group Mergers: Strategies for Success
Will Latham, MBA, CPA
President, Latham Consulting Group, Inc., Chattanooga, TNIn today’s anesthesiology environment, all groups are trying to size up their best option to survive and thrive into the future. Some try to go it alone and others sell out to practice management firms, while others seek or are forced into hospital employment.
Another option that many groups are considering is merging with other anesthesiology groups.
Why are anesthesiology groups considering mergers? Mergers:
- Allow them to maintain a higher level of autonomy than any other option,
- Prevent the groups from being played off against each other by hospitals or managed care companies,
- Build clout,
- Create the ability to hire needed management expertise, and
- Allow them to move towards economies of scale.
In addition, today’s healthcare environment is influencing many hospitals to merge or join systems. When hospitals integrate they often want to work with a single anesthesiology group to cover all their facilities. When this happens, many anesthesiology groups consider merging before the hospital system chooses winners and losers.
In order to be successful, medical groups that embark on a merger effort should know the answers to the following questions:
- What does it mean to merge?
- What are the costs and risks associated with merging?
- How does a merger process typically work?
- What are the key issues usually addressed in a merger process?
- Who participates in the merger process?
- How do we get started?
This article presents strategies for pursuing a successful merger based on working with more than 135 practices representing more than 1,300 physicians on merger-related projects.
What Is a “Merger”?
For the purposes of this article, a merger occurs when separate anesthesia groups become one group. Mergers may come about in many ways (via a true merger of groups, an asset purchase or a consolidation transaction—your attorney and accountant will help you decide which option to choose), but result in the combined organization exhibiting the following characteristics:
- One separate professional corporation or limited liability partnership is formed (or separate practices combined) and there is one tax identification number and single provider number.
- All physicians enter into an employment agreement with this organization.
- All employees from the previously independent practices become employees of the new entity.
- Operations are conducted by the new entity which bills and collects for physicians’ services in its own name.
- The combined entity owns the funds and revenues created by the work of its physicians.
- The merged group holds any exclusive provider agreements.
- Physicians typically contribute all assets from the predecessor organization. However, there are options where assets (such as real estate) can be kept in separate entities and leased to the merged practice.
- Benefit plans are standardized.
- Physicians become subject to one governing entity.
What are the Costs and Risks of Merging?
While there are significant benefits to be gained, there are also costs and risks:
- Work: Putting a merger together requires a significant amount of work and time from both the physicians and their administrative staff. Mergers often take six to twelve months to complete, and there are many issues to be discussed and decisions to be reached.
- Costs: Professional costs (attorneys, accountants, consultants) are significant. While professionals will often provide ballpark estimates at the beginning of the process, these estimates can change depending on the ability of the merger participants to negotiate and reach conclusions.
- Compromise: Many significant changes may be required by all involved. It is not feasible to merge and keep everything the way that it was. Some level of operational integration will be required and this requires compromise.
- Loss: Some individual physicians may not wish to merge and may leave the group. They may not like specific decisions that change their work life and/or limit their options (for example, when many practices merge they implement non-compete provisions in their employment contracts—this is unacceptable to some physicians). While the goal of the merger should be to keep all the physicians in the group, it may not be achievable.
- Failure: A merger might not be achieved. Anecdotal evidence indicates that 50 percent of all merger processes do not end in a merger. In some instances, this is a positive development as groups may turn out to not have the same long-term goals. In other situations, the lack of a disciplined effort to reach a decision often results in people becoming frustrated with the lack of progress and dropping out.
- Outsiders: External stakeholders might be uncomfortable with the merger. For example, hospital management may not be enthusiastic about a merger between hospital-based physicians.
Even with these costs and potential negatives, many anesthesiology groups believe that the potential benefits far outweigh the identified risks and decide to move forward with a merger process.
How Does a Merger Process Typically Work?
Merger processes involve a number of discrete yet inter-related steps. The general process is typically one of:
- Getting comfortable with each other,
- Understanding each other’s philosophy of practice,
- Discussion and negotiation of key merger issues,
- Developing Agreements in Principle,
- Closing the merger, and
- Implementing operational integration plans.
The specific steps of the merger effort are generally as follows:
- Friendship and Courting: Prior to any substantive discussions, members of each practice often make contact with each other via informal means. Typically they talk about shared interests, the benefits of merging and generally how the merger might work. Unfortunately, they also tend to avoid talking about any issues which might involve conflict. While avoiding issues of conflict at this point can keep the ball rolling, the issues which involve potential conflict must be resolved for a merger to occur.
- Commitment to Move Forward: At some point the groups agree that they should get down to brass tacks and look at the merger in a more formal manner. At this point they may engage someone to serve as a facilitator of the process. Such a facilitator could be a consultant, attorney or accountant.
- Antitrust Review: Depending on the local market, one of the first steps is to engage an attorney to conduct an antitrust review. While the details of such a review are beyond the scope of this article, the groups should seek experienced legal counsel in this area if there are any concerns about creating significant market power.
- Confidentiality, Non-Competitive Use, No-Shop Agreement: In order to protect their rights and the confidentiality of information, the groups should have their attorney draft an agreement in which each group agrees to:
- Confidentiality: Both groups agree to keep the other group’s information confidential.
- Non-Competitive Use: The groups agree to use the information obtained from the other group only for the purposes of merger negotiations.
- No-Shop: In this part of the agreement the groups agree to not seek offers from or negotiate offers with others for a period of time (say, three to six months). While the no-shop provision is optional, we believe that is critical when anesthesiology groups negotiate a merger for three reasons:
- Groups that are looking to merge are typically trying to remain independent in order to retain as much autonomy as possible. If one or more of the groups are looking for a buy-out, that is antithetical to the goal of retaining autonomy. Groups hoping for a buy-out should pursue being acquired rather than a merger.
- The time and dollars spent on the merger process come directly from the groups involved (as opposed to being paid for by investors). Once again, if a group is involved in acquisition negotiations, one has to wonder if it is worth risking the time and dollars on the effort to merge with them.
- If the groups don’t agree to a no-shop agreement it will be difficult for them to make the compromises necessary in a merger negotiation (because they may believe there is another alternative that may not require that particular compromise).
- Merger Committee Appointment and Empowerment: Unless the practices are very small, it is wise to appoint a Merger Committee to do the bulk of the discussion and negotiation effort in the merger. It is desirable that the rest of the physicians empower this group to discuss and negotiate on the key merger issues. Typically this committee includes one to three individuals from each of the groups.
- Gather/Organize Data: In order to improve the efficiency and effectiveness of the merger discussions, a significant amount of information must be gathered from each group. Such information may include practice documents and financial information. In addition, it is typically appropriate to have each physician and administrator interviewed or surveyed to identify any merger concerns that they may have.
- Merger Negotiation Meetings: Using the information gathered in the preceding step, the Merger Committee meets to discuss, negotiate and reach Agreements in Principle related to the key merger issues (discussed in the next section of this article). There are two basic approaches to how this process may be conducted:
- For groups that have already had significant discussion or are very knowledgeable about each other, a Merger Retreat (typically two to two and one-half days) can be used to finalize most Agreements in Principle.
- For groups that need more in-depth discussion and negotiation, a series of meetings are held during which Agreements in Principle are made. This is the more typical situation. During this effort other professionals (such as accountants, attorneys, benefits consultants, etc.) are involved as needed.
- Letter of Intent: Once the major Agreements in Principle have been made, the groups typically execute a Letter of Intent in which they agree to merge under the negotiated terms unless certain events occur. Once this document is signed, the attorneys, accountants and group management begin working in earnest to close the merger and develop plans for integration.
- Perform Due Diligence: During this step, the attorneys and accountants review a number of practice-related documents to identify any issue that might impact the merger from a legal, financial or tax perspective.
- Create Merger Documents: Once the Letter of Intent has been signed, the attorneys will draft several documents, including:
- Merger Agreement (the primary purpose of this document is to require each group to make full disclosure about its activities).
- New Entity Corporate Documents.
- New Entity Shareholder Agreement (Buy-Sell).
- New Entity Physician Employment Agreements.
- Other needed documents.
- Financial: At the same time the legal work is being performed, the accountants will be developing the financial information needed to close the merger and will be working with the attorneys to propose the best corporate form for a combined group. Depending on how the groups come together, the accountants may assist with cash flow forecasting.
- Develop Operational Integration Plan: The work we have discussed up to this point is focused primarily on the organizational, financial and legal aspects of the merger. Once the groups are on track to merge, an operational integration plan must be developed. This is normally prepared by the administrative management team selected.
- Merge: The merger occurs when all papers are signed and all are committed to move forward.
- Implement Operational Integration Plan: The operational integration plan is implemented.
What Are the Key Issues Usually Addressed in a Merger Process?
The key merger issues are different for any particular merger. However, typical key issues include:
- Overall practice philosophies
- Governance
- Physician compensation system, retirement plans, benefits
- Physician contract issues
- Buy-in/buy-out
- Value of capital contribution/ownership
- Call/workload
- CRNAs, anesthesiologist assistants: mid-level utilization and protocols
- Administrative management
- Billing and collections
- Personnel
- Relationships with professional service providers (attorneys, accountants, etc.)
- Operational infrastructure
As noted earlier, it is essential that those facilitating the negotiations capture the Agreements in Principle related to each of these issues. This information is critical for several reasons:
- It clarifies the actual agreements made (oral agreements can be remembered differently by different people).
- It can be used to communicate the agreements to those who are not on the Merger Committee.
- It will be used by the attorneys, accountants and administrative management to close the merger and implement activities related to the combined group.
Who Participates in the Merger Process?
Medical practice mergers involve a number of individuals and advisors to complete the process.Naturally, the physicians in the practices are key to the success of any merger. They approve the final agreements. In many cases they should be interviewed individually to identify their specific concerns or key issues that must be addressed in the merger process. They should also be questioned about drop dead issues that need to be resolved.
As noted earlier, a Merger Committee should be established to negotiate the merger. In mergers of small practices typically all physicians are on the committee. For larger practices each group is usually represented by one to three physicians. If a subset of the physicians from any one group is on the committee, they should be empowered to speak for the others.
In most mergers, the practice’s administrative management is involved. They help with data-gathering, are often involved in negotiations, and are very involved in operational integration of the merger.
Many practices use a merger facilitator to organize the merger effort. The role of this individual is to serve as the objective third party who organizes the process and keeps efforts on track.
The facilitator sets the format and process for analyzing and discussing issues, and facilitates the negotiation meetings.
Once substantive Agreements in Principle have been reached, attorneys become heavily involved in the process. They advise the practices about various structural issues related to combining the organizations, develop merger agreements and other legal documents, perform due diligence and provide legal guidance on other issues.
Accountants are involved in forecasting the financial implications of the merger, providing guidance on tax and accounting issues, and preparing financial information needed to close the merger.
In some mergers others are involved, such as third party appraisers (if the merger involves real estate or other special assets) and benefits consultants.
Pitfalls to Avoid
There are many challenges that will need to be overcome when trying to merge two or more medical groups together. Here are a few pitfalls to avoid:
- Dueling Attorneys: Most have heard the aphorism that “one attorney in a small town starves, but two attorneys in the same small town make a nice living.” We have come across many cases where merger negotiations have bogged down or fallen completely off the track because the practices involved their attorneys in the negotiation process or tried to use the attorneys to negotiate for them. This is often because they spend so much time representing their client’s position and interests that it increases the likelihood that the two practices will not reach common ground.
- Naturally attorneys should review any agreements in principle, prepare merger documents, and be involved in the due diligence aspect of the merger. But care must be taken that there is someone representing the interests of the combined entity as opposed to the interests of each individual practice. This task usually falls to the merger facilitator.
- Lack of a Planned, Controlled Approach: More merger efforts are abandoned because they drag on and on than are terminated because of a disagreement over a particular issue. It is therefore essential that those involved use an organized, systematic approach to negotiating the merger.
- Lack of Full Disclosure: Full disclosure between the practices is critical for two reasons:
- Physicians won’t merge their practice with another unless they have significant knowledge about how the other practice is organized and operates.
- Unlike mergers in other industries where whoever is bought out leaves, when medical practice mergers are complete all (or at least most) of the physicians are still there, trying to live together in a new organization. To improve prospects for harmony, it is imperative to avoid surprises after the merger. Therefore, it is best to fully disclose information early on during the merger negotiations instead of waiting for it to be discovered in the due diligence process.
- Lack of Recognition that Changes Will Be Needed: In any merger, changes will be needed to make the combined organization work. If members of either practice are not open to such changes and compromises they should not embark on the merger negotiation process, as they will be disappointed in the outcome.
- Inability to Compromise: Upon beginning negotiations, each physician typically has his or her own viewpoint, opinion and expectations for the outcome. Each physician typically recognizes that there are a number of benefits to be gained from a merger (or they would not have initiated the merger negotiations to begin with), but during the heat of negotiations they often lose sight of the benefits to be gained and focus only on that they are not getting exactly what they want. When this occurs, whoever is facilitating the merger negotiations must be vigilant to remind the physicians of the benefits of the merger. The facilitator should always ask the question, “Are you willing to give up all the benefits of the merger over this one issue, or can compromises be made?”
- Talking but Not Deciding: In our experience, many physicians tend to be conflict avoiders. This hinders the ability to move a merger forward because when the groups come upon an issue where they don’t fully agree, they back away from it and start talking about other, less important issues. This can cause the negotiations to go on and on without making true progress. An objective third party is often needed to help the groups overcome this limitation and make the compromises necessary to merge.
Conclusion
These are challenging times for anesthesiologists and almost all groups are working hard to determine how to best move forward. Anesthesiology group mergers represent one of those options.
All anesthesiology group mergers have their challenges. However, in today’s rapidly changing healthcare environment, mergers continue to be an important option for anesthesiologists wishing to gain strength while retaining a significant level of autonomy.
Will Latham, MBA, CPA, President, Latham Consulting Group, Inc. Latham Consulting Group helps medical group physicians make decisions, resolve conflict, and move forward. For more than 25 years Mr. Latham has assisted medical groups in the areas of strategy and planning, governance and organizational effectiveness, and mergers, alliances and networks. During this time he has: facilitated over 900 meetings or retreats for medical groups; helped hundreds of medical groups develop strategic plans to guide their growth and development; assisted over 130 medical groups improve their governance systems and change their compensation plans; and advised and facilitated the mergers of over 120 medical practices representing over 1,200 physicians. Latham has an MBA from the University of North Carolina in Charlotte and is a Certified Public Accountant. He is a frequent speaker at local, state and national, and specialty-specific healthcare conferences. Mr. Latham can be reached at (704) 365-8889 or wlatham@lathamconsulting.com. -
Numbers Don’t Lie, but…
Gregory R. Zinser
Vice President, Anesthesia Business Consultants, Jackson, MIWe’ve all heard the saying “numbers don’t lie,” and while that may be true, if you aren’t looking at the RIGHT numbers presented in a way you can understand, they can be misleading.
For any type of business, the underlying purpose of a reporting system is to provide timely and accurate information to be used by leadership as a basis for making decisions. In most groups, there is no shortage of information in terms of volume, but are you really getting all information you need in a format you can understand? Unfortunately, there is no standard frame of reference. One set of reports may seem adequate until you see a different approach. For most groups, it is difficult to optimize your reporting system and ask the right questions unless you have a member with both a background in financial analysis and time to devote to this task. The purpose of this article is to provide a general perspective on reporting, along with some specific ideas that may help you improve your current reporting system.
There are three common flaws in reporting systems:
- The sheer volume of information presented is overwhelming;
- The presentation format is confusing; and
- Important information is omitted.
Reports that contain huge amounts of information in a confusing format can divert attention from the important information that is not included. They become tools of mass distraction, rather than the essential monitoring and early warning systems they should be.
Report packages should include all information needed to make decisions relating to the clinical, operational and financial aspects of the practice—no more and no less. Collecting information is not time consuming. Reporting all of the available information is not difficult. The real time and work of creating great reports is in the distilling of the detail and design of reports that facilitate review, understanding and discussion. Simply put, great reports will generate the right questions.
The following guidelines are applicable to all types of reports:- All amounts should be shown in whole dollars;
- All primary statements should be condensed to fit on one page, using a font size that can be easily read (sub-reports can be used to provide additional detail as necessary);
- All line item titles should provide a clear and concise description of amounts presented; and
- Statements should be available no later than 30 days after the end of a reporting period.
Essential financial reports in most practices would include the following:
- Narrative – All report packages should be accompanied by a narrative that first explains the purpose of each report in the package; lists all underlying assumptions (e.g., accrual vs. cash basis); highlights any key variances or trends in the figures for each statement; and, if applicable, states recommendations for further action to be taken. This narrative is the difference between simple accounting and useful interpretation and analysis. It is also the difference between having an accountant and an advisor. Any accounting service can produce the numbers, but it takes insight and skill to analyze and interpret the data.
- Balance Sheet – Shows all major categories of all assets and liabilities for the most recent month end, the previous month end, and the most recent fiscal year end.
- Income Statement – Shows all major categories of revenue and expenses for the most recent month end, current year to date, year to date actual at the same time last year, current year budget year to date, and a column showing the variance between current year to date actual and budget. In order to fit this statement on one page, all expenses deducted from individual physician compensation are shown as one total, as are all overhead expenses. The subschedule for the former is a simple listing of the detail on one page with all of the same column headings. The subschedule for the overhead expenses is the Overhead Rate Analysis described in Figure 1 on page 15.
- Overhead Rate Analysis (see Figure 1) – Shows all major categories of overhead expense for the current month, and year to date. Year to date figures are compared to year to date budget, and a variance column is also shown. The total annual budget amounts are also shown for each line item. The actual overhead percentage is computed for each of the three major categories of overhead expenses (billing and collection fees, management fees and all other expenses), and is compared to budget and to amounts assessed for overhead year to date. Variances from budget and/or the assessed overhead rate are clearly shown.
Essential operational reports and performance measures in most practices would include the following:
- Net Collection Percentage – Measures how much of what is collectable is actually being collected. The only meaningful way to do this is based on actual results, which means it must be measured no sooner than six months in arrears to be sure that the collection cycle is completed. In addition, all data used for charges and adjustments should be by date of service, with collection amounts directly related to those charges. A sample calculation measuring net collection percentage for the six months ended June 30, 2014, is shown below:
Measurement date of March 1, 2015 for all dates of service from January 1 through June 30, 2014:
Charges $1,000
Contractual adjustments (550)
Other allowable adjustments (50)
Collectible charges $400
Actual collections through March 1, 2015 relating to dates of service from June 1 through June 30, 2014 = $370. Amounts in accounts receivable at March 1, 2015 considered collectible (net) = $20.
Net collections percentage for the six months ended June 30, 2014 = $370+$20/$400 or 97 percent. As is the case with most percentage measures, the statement that can be made about the inverse is just as important as the percentage itself. In this case, the remaining three percent has three components (all relating to dates of service from January 1 to June 30, 2014): 1) bad debt write-offs; 2) amounts in accounts receivable at March 1, 2015 not considered collectible; and 3) non-allowable write-offs such as untimely filing. - Days in Accounts Receivable – Measures how quickly accounts receivable are being collected by calculating the average number of calendar days elapsed from the date charges are posted to the final disposition of the account. Each of the most recent 12 months are shown by major payer category. Also shown for each major payer category is the performance target (if any) and ending AR, both gross and estimated net. A sub-report also shows the same information for more detailed payer categories.
- Accounts Receivable Aging – Classifies outstanding accounts receivable balances by current responsible payer into aging categories based on the date of posting. Accounts receivable balances are not re-aged as partial payments are received, and the aging should not include credit balances. Also shown is the self-pay component of total dollars in each major payer category; and for the four most recent months, the percentage of accounts over 120 days old as compared to the established target (if any). A sub-report also shows the same information for more detailed payer categories.
- Credit Balances in Accounts Receivable – A separate aging of credit balances in accounts receivable is shown by major payer category. A sub-report also shows the same information for more detailed payer categories.
- Collection Agency Performance – For each of the most recent three months and the most recent calendar year, this report shows the collection percentage of accounts transferred to collection agencies, net of collection agency fees. For each period reported, these reports will also show the aging of accounts transferred, the average time between transfer and collection and the total number and amount of accounts in collection agency “inventory” at the end of the reporting period, along with the aging of those accounts, both by date of service and by date of placement.
- Payer Mix Analysis – Designed to identify changes or trends in the group’s payer mix, which could impact the group’s overall reimbursement rate. Percentage of charges for each major payer category are shown for each of the most recent four quarters, and compared to the most recent 12-month average, and the previous 12-month average. A sub-report also shows the same information for more detailed payer categories.
- Productivity Report – This report shows base units, time units, total cases, base and time units per case and net collections per case and per unit, for each of the most recent 12 months and the most recent 12-month average. It is by date of service, and is reported one month in arrears to allow adequate time for processing of all charge tickets for each month.
- Average units per location (for multi-location practices) – Shows total units billed by date of service and average units per nonholiday weekday for each service location. Data is shown for each of the most recent 12 months, the most recent 12-month total, and the previous 12-month total.
Summary
Reporting systems are no more than management tools, and like any other job, you must have the right tools to effectively manage a medical group. If you don’t have complete confidence in your current reporting systems, consider working with your practice managers to challenge the need for certain reports, and design new ones that give you all of the information you need in a format you can use. The group and its leadership will benefit from both the process and the end result for many years to come.
Gregory R. Zinser, Vice President, has recently joined ABC and comes with a broad range of experience in healthcare finance and administration. Mr. Zinser’s recent experience includes four years as CEO of one of the nation’s largest anesthesia billing and practice management companies, and CEO of the management company for one of the nation’s largest anesthesia groups. With experience in all facets of anesthesia practice management, Zinser adds additional strength and depth to an ABC management team that has become the industry standard in terms of both responsiveness and quality of resources. He is a licensed CPA with an undergraduate degree in accounting with honors from the Ohio State University. Mr. Zinser can be reach at Greg.Zinser@AnesthesiaLLC.com

 How do we identify what our customers need? We must first identify our customers and unfortunately this seems to be changing on a regular basis. In the ASC realm, who are the decision makers and are they our customers? This varies as well depending upon the ownership and governance structure of the facility. There are tools available to us that we should strongly consider.
How do we identify what our customers need? We must first identify our customers and unfortunately this seems to be changing on a regular basis. In the ASC realm, who are the decision makers and are they our customers? This varies as well depending upon the ownership and governance structure of the facility. There are tools available to us that we should strongly consider. Extracting the data and information and putting them into a context to be shared amongst your colleagues is of paramount importance. This can truly define your strategic plan moving forward.
Extracting the data and information and putting them into a context to be shared amongst your colleagues is of paramount importance. This can truly define your strategic plan moving forward. Stanford R. Plavin, MD has been actively involved in the ASC arena for 18 plus years as a practicing anesthesiologist serving as past president of the Georgia Society of Ambulatory Surgical Centers and currently an Ambulatory Surgery Center Association board member. He practices in Atlanta, GA as a co-founder of Ambulatory Anesthesia of Atlanta and can be reached at
Stanford R. Plavin, MD has been actively involved in the ASC arena for 18 plus years as a practicing anesthesiologist serving as past president of the Georgia Society of Ambulatory Surgical Centers and currently an Ambulatory Surgery Center Association board member. He practices in Atlanta, GA as a co-founder of Ambulatory Anesthesia of Atlanta and can be reached at 
 The example in the table above indicates both the level of a pain program’s potential profitability and the differences of profitability depending on the center’s facility base. The example summarizes a pro-forma developed for a major southeastern health system’s chronic pain management program. Hospitals have found that comprehensive pain management programs that are strategically located, energetically developed and well run can attain strong profitability within a two to three year period.
The example in the table above indicates both the level of a pain program’s potential profitability and the differences of profitability depending on the center’s facility base. The example summarizes a pro-forma developed for a major southeastern health system’s chronic pain management program. Hospitals have found that comprehensive pain management programs that are strategically located, energetically developed and well run can attain strong profitability within a two to three year period. Jerry Ippolito, MBA, MHSA is President of OR Efficiencies, LLC, Naples, FL. OR Efficiencies, LLC is a management consulting firm specializing in assisting hospitals and ASCs to improve their perioperative services and anesthesiology programs. Mr. Ippolito can be reached at
Jerry Ippolito, MBA, MHSA is President of OR Efficiencies, LLC, Naples, FL. OR Efficiencies, LLC is a management consulting firm specializing in assisting hospitals and ASCs to improve their perioperative services and anesthesiology programs. Mr. Ippolito can be reached at 

 Medical practice mergers involve a number of individuals and advisors to complete the process.
Medical practice mergers involve a number of individuals and advisors to complete the process.
 Will Latham, MBA, CPA, President, Latham Consulting Group, Inc. Latham Consulting Group helps medical group physicians make decisions, resolve conflict, and move forward. For more than 25 years Mr. Latham has assisted medical groups in the areas of strategy and planning, governance and organizational effectiveness, and mergers, alliances and networks. During this time he has: facilitated over 900 meetings or retreats for medical groups; helped hundreds of medical groups develop strategic plans to guide their growth and development; assisted over 130 medical groups improve their governance systems and change their compensation plans; and advised and facilitated the mergers of over 120 medical practices representing over 1,200 physicians. Latham has an MBA from the University of North Carolina in Charlotte and is a Certified Public Accountant. He is a frequent speaker at local, state and national, and specialty-specific healthcare conferences. Mr. Latham can be reached at (704) 365-8889 or
Will Latham, MBA, CPA, President, Latham Consulting Group, Inc. Latham Consulting Group helps medical group physicians make decisions, resolve conflict, and move forward. For more than 25 years Mr. Latham has assisted medical groups in the areas of strategy and planning, governance and organizational effectiveness, and mergers, alliances and networks. During this time he has: facilitated over 900 meetings or retreats for medical groups; helped hundreds of medical groups develop strategic plans to guide their growth and development; assisted over 130 medical groups improve their governance systems and change their compensation plans; and advised and facilitated the mergers of over 120 medical practices representing over 1,200 physicians. Latham has an MBA from the University of North Carolina in Charlotte and is a Certified Public Accountant. He is a frequent speaker at local, state and national, and specialty-specific healthcare conferences. Mr. Latham can be reached at (704) 365-8889 or  The following guidelines are applicable to all types of reports:
The following guidelines are applicable to all types of reports: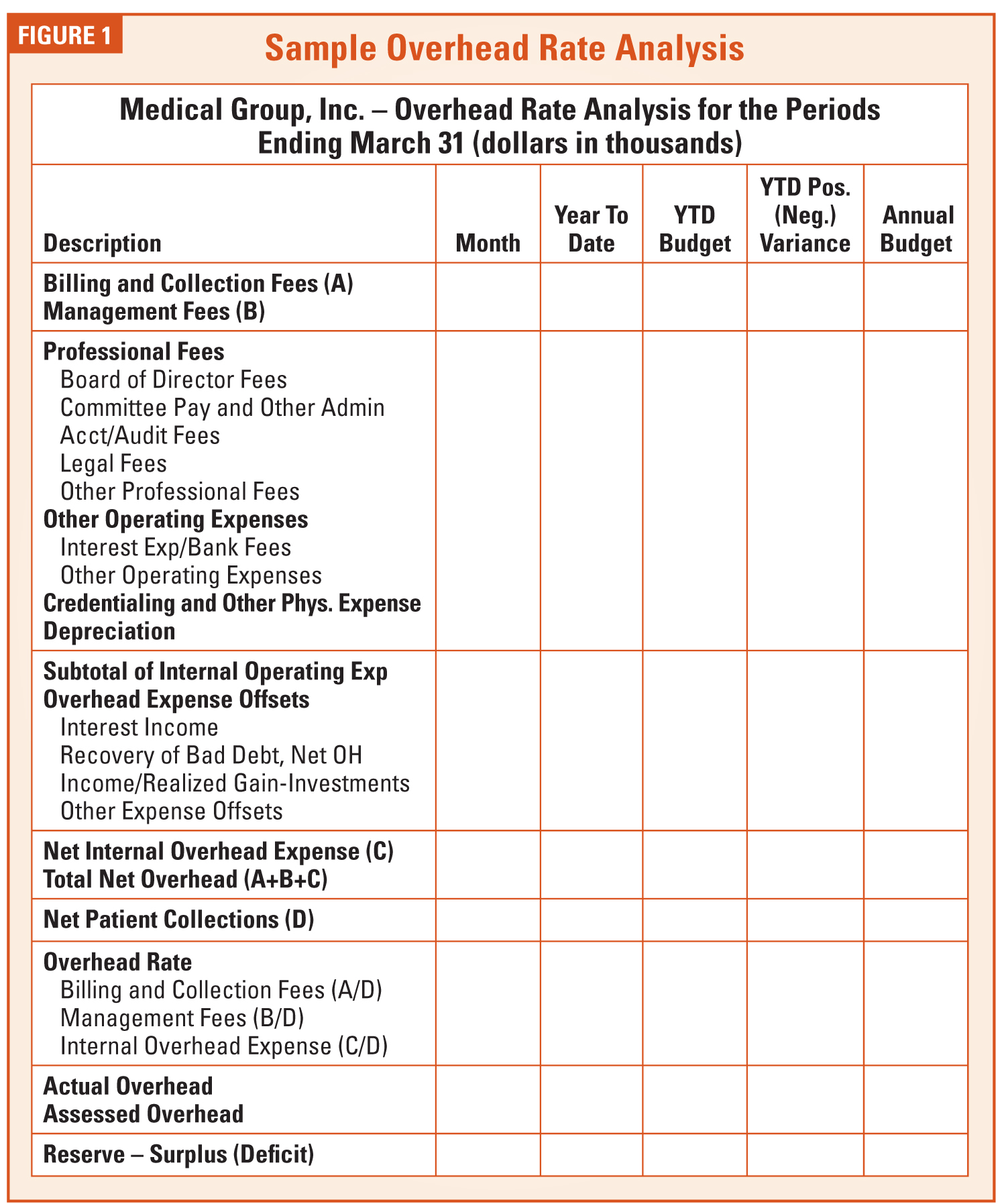

 Gregory R. Zinser, Vice President, has recently joined ABC and comes with a broad range of experience in healthcare finance and administration. Mr. Zinser’s recent experience includes four years as CEO of one of the nation’s largest anesthesia billing and practice management companies, and CEO of the management company for one of the nation’s largest anesthesia groups. With experience in all facets of anesthesia practice management, Zinser adds additional strength and depth to an ABC management team that has become the industry standard in terms of both responsiveness and quality of resources. He is a licensed CPA with an undergraduate degree in accounting with honors from the Ohio State University. Mr. Zinser can be reach at
Gregory R. Zinser, Vice President, has recently joined ABC and comes with a broad range of experience in healthcare finance and administration. Mr. Zinser’s recent experience includes four years as CEO of one of the nation’s largest anesthesia billing and practice management companies, and CEO of the management company for one of the nation’s largest anesthesia groups. With experience in all facets of anesthesia practice management, Zinser adds additional strength and depth to an ABC management team that has become the industry standard in terms of both responsiveness and quality of resources. He is a licensed CPA with an undergraduate degree in accounting with honors from the Ohio State University. Mr. Zinser can be reach at