eAlerts
-
Proposed Meaningful Use Stage 2—What it Means to the Anesthesia and Pain Communities
Abby Pendleton, Esq., The Health Law Partners, P.C., Southfield, MI
Stephanie P. Ottenwess, Esq., The Health Law Partners, P.C., Los Angeles, CAOn March 7, 2012, the Centers for Medicare and Medicaid Services (CMS) published its Notice of Proposed Rule Making (NPRM, or proposed rule) for Stage 2 user requirements for the Medicare/Medicaid Electronic Health Record (EHR) Incentive Program (“meaningful use,” or MU) in the Federal Register. 77 FR 13698.1 There is a three pronged focus to the Stage 2 criteria: standardizing data formats to dramatically simplify how information is both captured and shared across disparate IT systems in order to be better able to coordinate care with other physicians; ensuring that patients be able to access and easily download their healthcare records and images for their own use; and expanding the scope of tracked quality metrics to include specialists and to reflect and improve specific patient outcomes as well as care coordination.

Although subsequent to the final rule establishing Stage 1 MU criteria CMS repeatedly assured the medical community that the needs of specialists would be addressed in the Stage 2 requirements, the Stage 2 proposed rule still falls short for certain specialists including anesthesiologists. Indeed, although CMS itself boasts that the Stage 2 criteria have greater applicability to many specialty providers with the addition of objectives with respect to:
- Imaging results and information accessible through certified EHR technology;
- Capability to identify and report cancer cases to a State cancer registry; and
- Capability to identify and report specific cases to a specialized registry (other than a cancer registry), these objectives are not generally applicable to anesthesiologists or pain specialists.
The proposed Stage 2 criteria establish that anesthesiologists and pain physicians are still stuck in the unenviable position of being required to demonstrate they are meaningful users of Certified EHR Technology – a difficult, if not impossible proposition for most – or face Medicare or Medicaid payment adjustments starting in 2015. As such, this article attempts to boil down the voluminous 455 page NPRM, highlight the changes that have been made to Stage 1 criteria and identify the similarities and differences between Stage 1 and 2 Meaningful Use. On the basis of the majority of this reading audience, the focus is exclusively on the proposed changes to the Medicare version of the EHR Incentive Program for eligible professionals (EPs)2.
Background
On July 13, 2010, CMS issued the final rule defining the meaningful use of EHR that specified the Stage 1 criteria EPs, eligible hospitals and critical access hospitals must meet in order to qualify for an incentive payment, calculation of the incentive payment amounts, and other program participation requirements. The final rules implemented the EHR incentive program requirements under the Health Information Technology for Economic and Clinical Health Act of 2009 (HITECH Act), the health care information technology provisions enacted as part of the American Recovery and Reinvestment Act of 2009 (ARRA). Under the EHR incentive program, Medicare and Medicaid incentive payments totaling as much as $27 billion from 2011 to 2021 will be available for payment to EPs and eligible hospitals for the “meaningful use of certified EHR technology.” The HITECH Act provisions are designed to serve the dual goals of improving health care through increased efficiencies and improved care decisions, while also stimulating economic recovery.
EPs who qualify for Medicare incentives can receive up to $44,000 per EP over a five-year period, while EPs who meet Medicaid patient volume requirements and qualify for Medicaid incentives can receive incentives of up to $63,750 per EP over six years. (EPs who qualify for both incentive programs must choose one.) In the Stage 1 final rule, CMS indicated that the Medicare and Medicaid EHR Incentive Programs would consist of 3 different stages of meaningful use requirements, with each stage requiring increasing use of EHRs and electronic information exchange. The three stages are:
- Stage 1 (which began in 2011 and remains the starting point for all providers): “meaningful use” consists of transferring data to EHRs and being able to share information, including electronic copies and visit summaries for patients.
- Stage 2 (to be implemented in 2014 under the proposed rule): “meaningful use” focuses on advanced clinical processes, including standards such as online access for patients to their health information and electronic health information exchange between providers.
- Stage 3 (expected to be implemented in 2016): “meaningful use” focuses on demonstrating that the quality of health care has been improved.
Stage 2—Anesthesiologists and Pain Physicians Must Still Comply
In the Stage 2 NPRM, there were no proposed changes to the hospital based eligible professional definition, and thus most anesthesiologists will continue to fall within the definition of an EP. Notably, however, CMS does ask for comment on situations where EPs who are classified as hospital-based and working in specialized hospital units have independently procured and utilized EHR technology that is completely distinct from that of the hospital. The focus of the comments should be on whether specialized hospital units are using stand-alone EHR technology as opposed to using the facilities and equipment of the hospital. This situation could be applicable to anesthesia groups, especially those that include pain specialists who have their own pain clinics where they are using stand-alone certified EHR technology.
Transitioning From Stage 1 to Stage 2 Meaningful Use
In the NPRM, CMS proposes a continuation of the existing paradigm in which an EP enters the program at Stage 1, regardless of the year of entry, and spends two years in each stage before proceeding to the next. Importantly, however, CMS proposes an extension of Stage 1, giving providers an additional year for implementation of Stage 2 criteria. Thus, those EPs who successfully participated in 2011 will have until 2014 to move into Stage 2. The reasoning behind this extension is to allow the needed time for vendors to develop and providers to implement certified EHR technology that can meet the new Stage 2 requirements. The additional time to achieve Stage 2 objectives is critical given the higher performance thresholds of Stage 2. With proposed regulations coming out now and final regulations expected this summer, it would have been nearly impossible for EPs to start Stage 2 by January 1, 2013. Certainly, this additional time will give providers the opportunity to emphasize quality over quantity in meeting meaningful use objectives.
In Stage 1, EPs are required to meet, or qualify for an exclusion to, all of the 15 core objectives and 5 out of the 10 menu measures for a total of 20 objectives. In the proposed rule, CMS proposes to maintain the same core and menu measures structure of meeting or qualifying for an exclusion of a total of 20 objectives but increases the number of core objectives to 17 and requires that EPs meet 3 of the 5 menu objectives. CMS is also proposing that, beginning in 2014, meeting exclusions from individual menu set measures will not reduce the total number of menu set measures that need to be reported. In other words, EPs will need to report on 5 of 10 menu set measures, regardless of whether they qualify for exclusions. However, those EPs qualifying for more than 5 exclusions will need to report on all of the menu set measures that are possible to report as well as the remaining exclusions.
Almost all of the Stage 1 core and menu objectives have been retained for Stage 2. However, multiple Stage 1 objectives have been combined into more unified Stage 2 objectives, with a subsequent rise in the measure threshold that providers must achieve for each objective that has been retained from Stage 1. According to CMS, this eliminates unnecessary accounting and reporting burden for providers by recognizing that, for providers who have been Stage 1 meaningful users already, recording these data in structured form has become a normal part of their delivery of health care. Stage 2 follows most of the existing Stage 1 core and menu objectives while adding new objectives for patient access to health information and increasing expectations for healthinformation exchange and data transfer, among other changes. Certain areas and elements in the Stage 2 rule may benefit EPs aiming for, and currently on the way to, meaningful use, whereas others may represent challenges.
Changes to Stage 1
There have been five (5) specific changes to existing Stage 1 objectives and measures including computerized provider order entry (CPOE); vital signs; test of health information exchange; e-copy and online access; and public health objectives. Some of the proposed changes are optional for EPs beginning in 2013 and mandatory in 2014 and beyond. The following chart describes the changes and their effective dates:
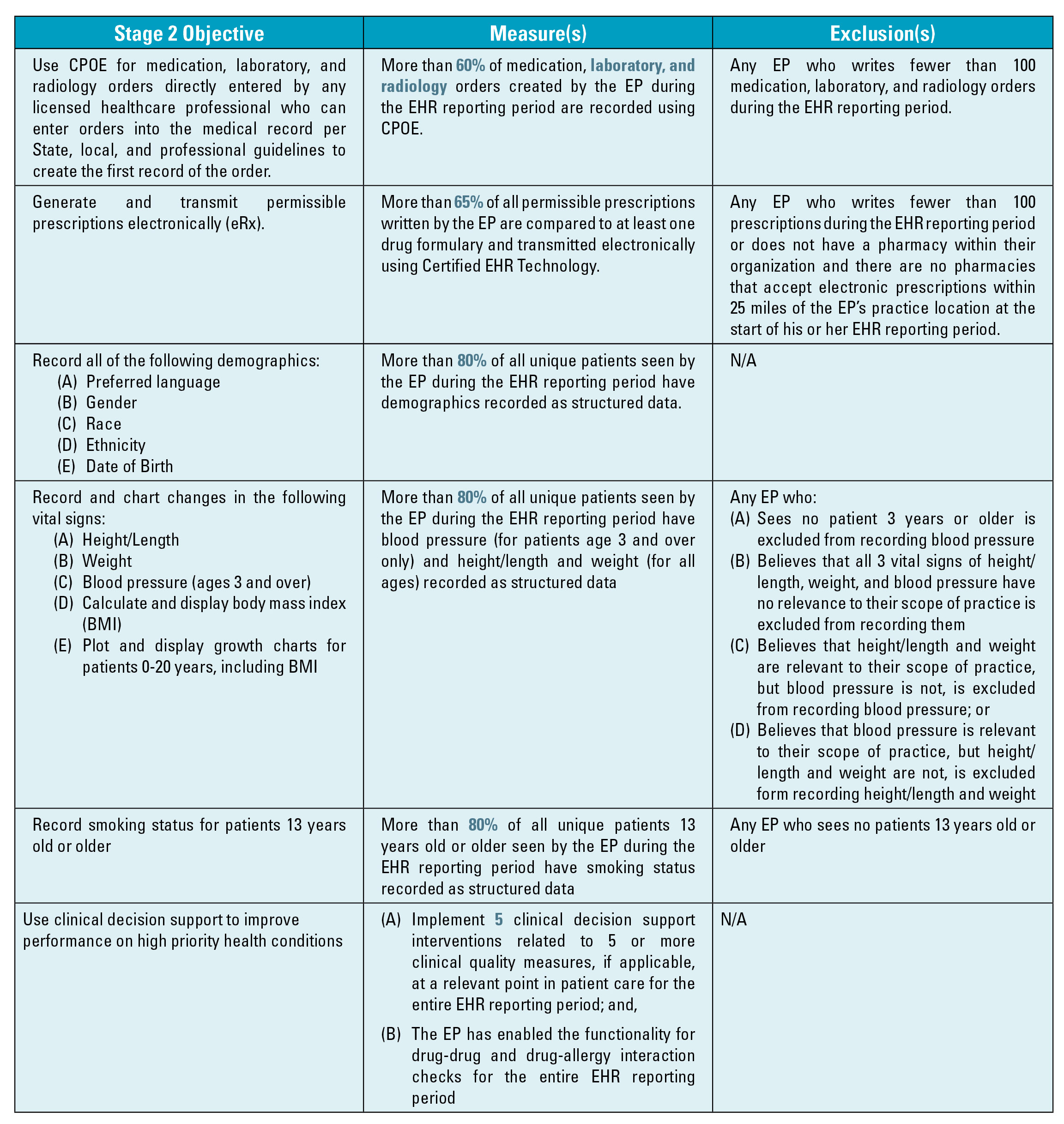
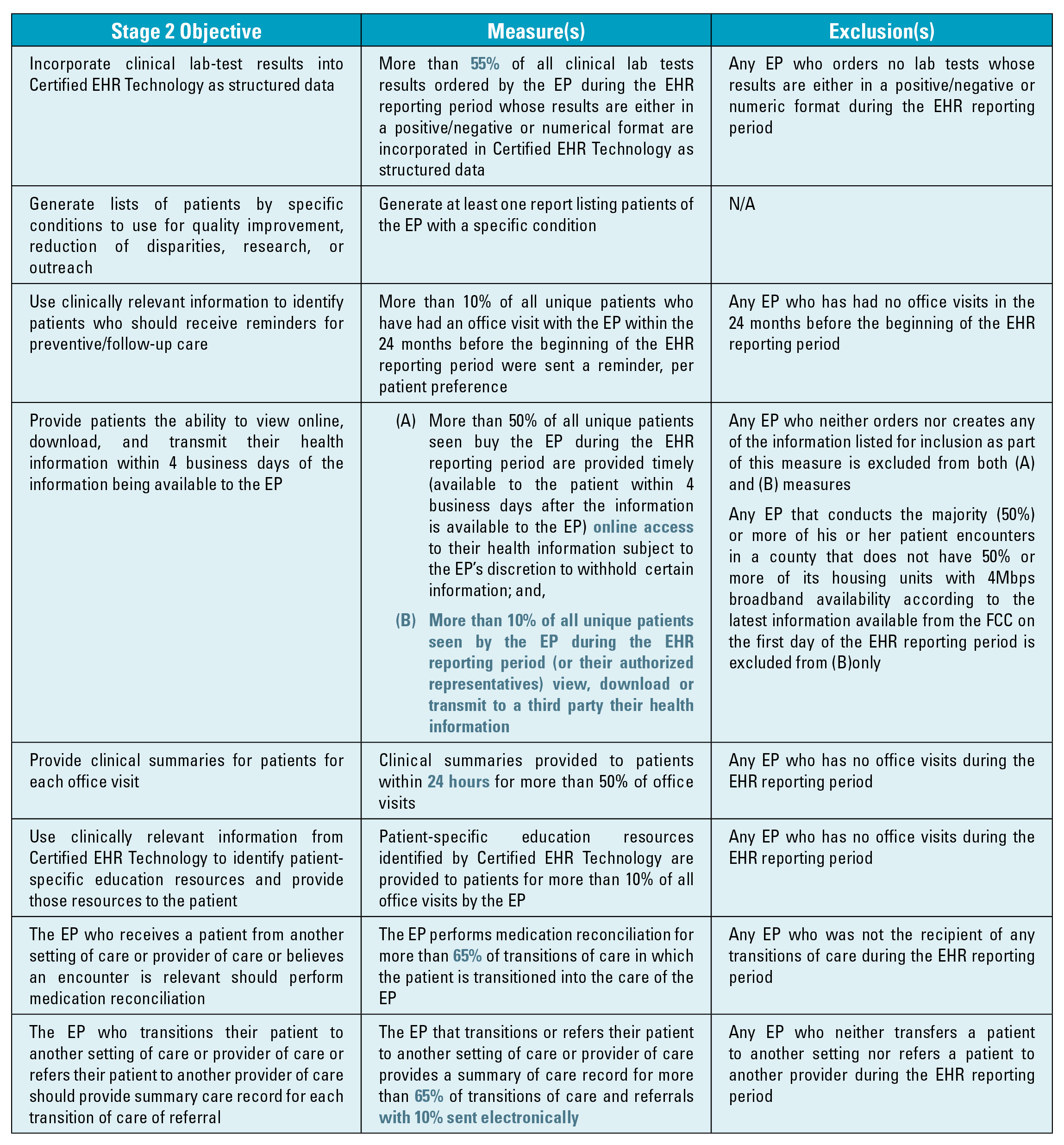
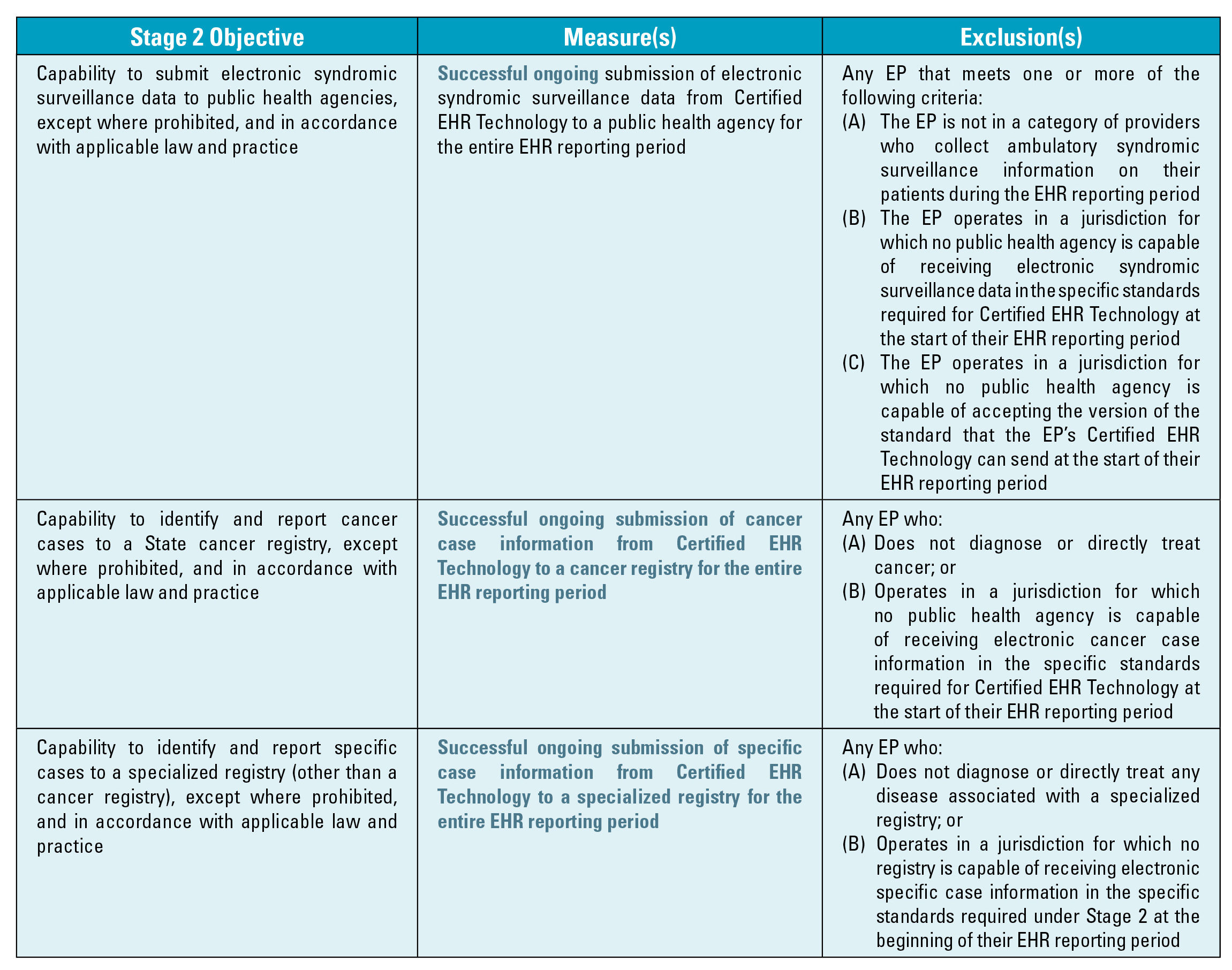
Proposed Stage 2 MU Objectives and Measures
The following table shows the proposed 17 mandatory objectives, measures and exclusions (where available). Changes from Stage 1 or new provisions are highlighted. This table is followed by a table containing the five menu set objectives.
Clinical Quality Measures
Just as in Stage 1, CMS proposes that EPs be required to report on 12 specified clinical quality measures (CQM) in order to qualify for incentive payments. CMS proposes, however, to eliminate CQMs as a meaningful use core objective and instead make reporting CQMs an inherent component of the definition of “meaningful EHR user.” The end result is that CQMs must still be reported in order for the EP to qualify as a meaningful EHR user.
For EPs, Stage 2 proposes a set of clinical quality measures beginning in 2014 that align with the existing quality programs such as measures for the Physician Quality Reporting System (PQRS) and the CMS Shared Savings Program. A major burden for providers to date has been the checkerboard of clinical quality measures that HHS programs ask providers to report. Hopefully, private payors will also adopt these measures for their quality programs since they will be already incorporated into certified electronic health records. If this occurs, it would radically reduce the complexity and burden of quality reporting for providers, and thereby increase clinicians’ focus on improvement.
The Stage 2 changes for clinical quality measures include an enhanced objective and associated measure to use clinical decision support to improve performance on high-priority conditions. This is a move from a requirement to use one decision support “rule” relevant to a specialty orclinical support “interventions” associated with high-priority health conditions. There is also a specific requirement to link each decision support intervention to one or more of the clinical quality measures reported on by a provider. Additionally, the objective to “exchange key clinical information” from Stage 1 was enhanced to provide a summary of care when a patient transitions from, or is referred to, a healthcare professional. These changes are intended to enhance the value of the clinical decision support and data exchange objectives.
The proposed rule also outlines a process by which EPs would submit CQM data electronically after their first year of Stage 1 participation, which, according to CMS, is aimed at the goal of reducing the associated burden of reporting on quality measures for providers. CMS has proposed two different approaches of CQM reporting: aggregate-level electronic reporting as a group or through existing quality reporting systems and is soliciting comments on these approaches.
Payment Adjustments
Medicare payment adjustments are required by statute to take effect in 2015. CMS proposes that any Medicare EP or hospital that demonstrates meaningful use in 2013 would avoid payment adjustment in 2015. Also, any EP that first demonstrates meaningful use in 2014 would avoid the penalty if they meet the attestation requirement by October 1, 2014. This means that the EP must begin the 90 day EHR reporting period no later than July 2, 2014. Notably, CMS is proposing new exceptions to these payment adjustments. This proposed rule outlines three categories of exceptions based on:
- Availability of internet access or barriers to obtaining IT infrastructure;
- A time-limited exception for newly practicing EPs who would not otherwise be able to avoid payment adjustments;
- Unforeseen circumstances such as natural disasters that would be handled on a case-by-case basis.
EPs would be required to submit an application to CMS for an exclusion to apply. The applications would need to be submitted not later than July 1 of the year before the payment adjustment year.
CMS is also soliciting comments on additional criteria for exceptions. Most important to specialists such as anesthesiologists, CMS specifically discussed the possibility that the combination of three barriers that are common to the specialties could constitute a significant hardship. The three barriers include:
- Lack of direct interaction with patients;
- Lack of need for follow-up care for patients; and
- Lack of control over the availability of Certified EHR Technology.
CMS made it a point that they do not believe that any one of these barriers taken independently constitutes a significant hardship but considered whether any specialty may nearly uniformly face all three barriers. Clearly, this is an excellent opportunity for the anesthesia community to convince CMS during the comment period that this exclusion should apply, in large part, to anesthesiologists.
Conclusion
Pursuant to the Stage 1 final rule and the proposed Stage 2 rule, the majority of anesthesiologists and pain physicians will fall within the definition of an EP and, as such, must either demonstrate they are a meaningful user of Certified EHR Technology or face Medicare payment adjustments starting in 2015. In the Stage 2 NPRM, CMS did open the door, ever so slightly, for specialists to make their case that they should not be included in the Medicare and Medicaid EHR Incentive Programs or be subject to the payment adjustments.
There is a 60-day public comment period, until May 7, 2012, which the Anesthesia Community would be well served to aggressively continue in its efforts to convince CMS that they should be excluded from the meaningful use requirements and payment adjustments. Comments can be made at www.regulations.gov. ABC will be submitting a letter. The importance of the comment period cannot be stressed enough as the general consensus is that the final rule, expected to be released this summer, is likely to mirror, in large part, the proposed rule. The Communiqué Spring 2012 P Page 11
Abby Pendleton, Esq., is a founding partner of The Health Law Partners, P.C. and has been practicing healthcare law since 1996. She regularly provides counsel to healthcare providers and organizations in a number of areas, including but not limited to: compliance, Recovery Audit Contractors (“RAC”), Medicare and other payor audits, fraud and abuse, reimbursement matters, and HIPAA Privacy and Security, and physician staff privilege and licensure matters. Ms. Pendleton also specializes in legal issues impacting billing and management companies, anesthesia and pain management providers, hospice providers and mental health agencies. Contact her at (248) 996-8510 or apendleton@thehlp.com.
Stephanie Ottenwess is a partner of The Health Law Partners, P.C. where she practices healthcare law representing providers and suppliers in healthcare litigation, providing counsel regarding fraud and abuse, compliance and reimbursement matters; and is consulted by both healthcare facilities and practice groups for her critical evaluation of any issue affecting risk management, including EHR adoption. Contact her at (248) 996-8510 or sottenwess@thehlp.com.
1 The HHS Office of the National Coordinator for HIT (ONC) issued a companion rule identifying updates to the standards and criteria for the certification of EHR technology. Whereas CMS has regulatory purview over implementation of the EHR Incentive Program, including requirements for participants, incentives, etc., ONC has regulatory authority over the HIT certification program, including the certification criteria, standards, and implementation specifications for products used by program participants.
2 Eligible professionals under the Medicare EHR Incentive Program include: (1) a doctor of medicine or osteopathy;(2) a doctor of dental surgery or dental medicine; (3) a doctor of podiatry; (4) a doctor of optometry; and (5) a chiropractor. Hospital-based eligible professionals are not eligible for incentive payments. An eligible professional is considered hospital-based if 90% or more of his or her services are performed in a hospital inpatient (Place Of Service code 21) or emergency room (Place Of Service code 23) setting. Only a small minority of anesthesiologists provide 90% or more of their services on an inpatient basis. Outpatient procedures performed in the hospital or in an ambulatory surgery center are excluded from the 90%.
-
Helpful and Not So Helpful Implementations of Health Information Technology
This issue of the Communiqué is a keeper. On pages 6 through 10 you will find tables that lay out clearly the Electronic Health Records (EHR) incentive program’s Stage 1 Meaningful Use objectives, the recently proposed changes to Stage 1, and the potential Stage 2 objectives, measures and exclusions as proposed by CMS in March. The objectives, translated into measures, are capabilities that your EHR must have in order for you to qualify for the incentive, which is non-negligible at a maximum of $44,000 per physician, or to avoid the penalty for non-compliance. Even though the proposed changes discussed in the Meaningful Use article by Abby Pendleton, Esq. and Stephanie Ottenweis, Esq. are likely to be different in some respects when CMS issues the final regulation later in the year, it is worth familiarizing yourself with the proposals because understanding the final versions will be that much easier.
The Meaningful Use article, just as importantly, describes the bind in which the EHR incentive program places anesthesiologists and pain physicians. The Meaningful Use requirements are heavily oriented toward primary care, office-based practices and it is close to impossible for anesthesiology and pain medicine professionals to meet them even if they have invested in their own EHRs or AIMS. Not only do our physicians not qualify for the incentive; they are also subject to the financial penalties that begin in 2015. To the best of our knowledge, there is no EHR technology that meets all the requirements for certification for use by anesthesiologists.
We know that there are efforts underway either to make the Meaningful Use requirements applicable to specialists or to exempt them from the penalties. Meanwhile, anesthesiologists and pain physicians can do something to help themselves. Like other proposed regulations, this one is open for public comments, which the law requires CMS to consider. In the Notice of Proposed Rulemaking published in the Federal Register on March 7, CMS specifically invited comments on (a) how to treat physicians working in specialized hospital units who are using stand-alone, independently procured certified EHR technology and (b) a possible exemption for specialists who can demonstrate three obstacles to Meaningful Use: (1) lack of direct interaction with patients, (2) lack of need for follow-up care for patients and (3) lack of control over the availability of certified EHR technology. The deadline for the submission of comments to CMS is May 7, 2012. We encourage readers to write to CMS, and we refer those who wish to do so both to Ms. Pendleton’s and Ms. Ottenweis’s article and to the ASA Washington Office.
For the first time in ABC’s 32-year history, we will be submitting comments to CMS urging an exemption for anesthesiologists and pain physicians whose practices do not reasonably allow for compliance with the Meaningful Use requirements. Our own OneSourceAnesthesia information platform and our partnerships with other clinical software providers give us unique insight into the systems barriers to demonstrating Meaningful Use.
In The AQI: Present and Future, Anesthesia Quality Institute Executive Director Richard P. Dutton, MD, MBA updates us on multiple developments. The National Anesthesia Clinical Outcomes Registry (NACOR) is growing as hoped. It now has data from 4,500 anesthesiologists and 3,500 nurse anesthetists working in 1,100 facilities. As of April 1, NACOR includes more than 4 million cases. This number will double by the end of 2012. NACOR is the single most significant database for comparative and internal clinical anesthesia benchmarking. Questions that NACOR will help users to answer include case duration, case numbers and differences in postoperative nausea and vomiting between inpatients and outpatients, to name just a few.
Are you one of the 4,500 or 3,500 professionals contributing data? You should be. The advantages of participation, present and planned, continue to expand. The AQI is now partnering with ASA to create interactive modules for the Maintenance of Certification in Anesthesiology Practice Performance Assessment and Improvement requirements. In October 2011, it launched the Anesthesia Incident Reporting System (AIRS). Individual reports of near misses and other rare events are de-identified and protected from discovery. The aggregated data enable the anesthesia community to identify emerging risks to patient safety more rapidly and will be the basis for an important new teaching tool, a national mortality and morbidity conference to be published as a regular column in the ASA NEWSLETTER.
The AQI is also an unequaled resource for investigators in the field of anesthesiology Comparative Effectiveness Research (CER). As Dr. Dutton explains in his article, “The development of sophisticated statistical methodology for risk adjustment and propensity scoring has made it possible to advance scientific knowledge through the retrospective study of large clinical data sets.” The AQI is looking for collaborators for CER projects.
If you submit claims to Medicare and other payers electronically – and you all do – you can automate the upload of data to the AQI with relative ease. AQI staff are ready to work with you whatever claims software you may be using. ABC is proud of our AQI Preferred Vendor status and we encourage every client who has not already asked us to submit their information to NACOR to do so.Our own staff member Arne Pedersen, MBA, FACMPE once again shares his considerable business expertise in Planning for Payor Negotiations. AAA Leadership Committee member Franc Galinanes walks readers through the subject Knowledge is Power: Why Anesthesiologists Need to Capture, Analyze and Use Data. This issue also contains one more contribution from Neda Mirafzali, Esq., who discusses why Anesthesiologists Should Beware of HIPAA Audits
As always, we hope that these articles will be informative and helpful, and we invite your comments, questions, suggestions and proposals for future issues.
With best wishes,
Tony Mira
President and CEO -
Planning for Payor Negotiations
Arne Pedersen, MBA, FACMPE
Director of Client Services, ABCEvery year, the time comes to begin looking at one or a set of payor contracts. A multitude of questions abound regarding appropriate rates, term length, and whether or not to participate or stay on panel. These are all good questions to raise. But are these the only questions to ask? This article seeks to explore the value of planning for payor negotiations.
As a backdrop to the planning, it is important to remember the value of strategic planning as described by Sun Tzu:
The general who wins a battle makes many calculations in his temple where the battle is fought. The general who loses a battle makes but few calculations beforehand. Thus do many calculations lead to victory, and few calculations to defeat: how much more no calculation at all! It is by attention to this point that I can foresee who is likely to win or lose.1
The point is primarily to ensure that a group can position itself for the best value in a given payor contract. There is an old saying in contract negotiations, “Everything is negotiable.” This is important to keep in mind when planning for payor negotiations. Finally, the approach to planning is also important. This should represent the consistent methodology to make decisions for the group. Two good examples include the McKinsey strategic problem-solving model2 and the decision-making model found in Pedersen’s book, Lead with Intent3.
A general plan for negotiations follows along a path similar to the following stages of negotiations:
Identify?Research?Options?Execution
IdentifyIn reviewing a contract for negotiations, it is important to understand what the main issues are for the group. This lays the groundwork for the research and ultimately, the group’s contractual objectives. Secondly, it is very important to note the termination provision of the current contract. There are times when it makes sense to terminate before the group negotiates. There are several issues to be brought up in the Identify phase including money, claims submission time, term and termination provisions, conflict resolution provision, and audit provisions to name a few. Again, focusing on the critical issues for the group will drive the process and ultimately the final deal.
Intuitively, the conversion factor is a big deal for most groups. This is the one part of the money that impacts a greater percent of anesthesia providers. Another area of money to focus on is the OB rate. It depends upon the practice if this is of major importance or not. The area demographics will drive that. There are schools of thought on OB rates. One focuses OB on a flat rate while the other is base plus time, with a cap. Again, the group needs to identify what makes sense for them. The last area of money is the flat fee schedule. The flat fees impact chronic pain practices primarily as well as nerve blocks (femoral and sciatic), arterial lines, CVP, TEE, and Swan-Ganz catheters to name a few.
The language of the contracts tends to go largely unnoticed by groups. There are some specific areas that might be of interest such as claims submission time, term of the contract including renewals, termination provisions, conflict resolution, how under and over payments are handled, and audits in particular. Again, a review of the practice will help to identify the areas of importance. When it comes to contractual language, it is a good idea to have outside counsel to help review and negotiate as necessary.
Research
All good decisions and negotiations begin with research. The first step of identification is important because it drives the focus on gathering the data points for the negotiations. It is important to understand the size and scope of the practice as well as the yield per unit and case. With the growing trend of high deductible health plans, you should analyze payments from the health plan only, not the patient portion. This will determine the actual yield from the payor. While deductibles and co-payments are a growing part of the financing of healthcare, this article is not going to focus on them. A separate article will better serve that purpose.
Another aspect of research is the review of the practice. This includes the internal business process for getting the finalized anesthesia records from the facility to the billing office or company and ultimately to the payor for payment. Take the time during the research phase to audit both the payor and the practice to understand the working relationship better. This will help when working on the mutual trust required in negotiations.
One final point to make in the research phase is how the data is pulled and prepared for presentation. It is important to help to make the case, or argument, for an increase.
OptionsFrom the findings in the research phase, it is time to develop the options for the negotiations. One critical error made in negotiations is the definition of the pie. Is it set in stone, or is there way to recast it? In Getting to Yes, Fisher and Ury discuss the concept of inventing options.4 While planning for the actual negotiations, ask questions and look for ways to brainstorm on mutual gain between the parties. Decide exactly what the practice needs and wants. There is a difference between the two and the distinction should become perfectly clear during the course of negotiations.
Another item to consider in this phase is the contractual language. In particular, this is the time decide which provisions match the actual business functions of the relationship and which do not. It is also important to note that many payors put their updates and provider manuals online and expect participating providers to read them (or not to read them, but to sign anyway). Recalling our earlier suggestion to engage legal counsel regarding language, that professional will now be able to help the group with the contract and the trends of a particular payor especially if that legal counsel works with other anesthesia groups in the area.
The final aspect of this phase is the decision on roles. This includes who will participate in the negotiations as well as what role the person will play.
Execution
With all of the planning completed, the group is now prepared to begin negotiations. One of the key tenets to negotiation is building trust.5 An easy approach to starting correctly is to meet and talk about the impending negotiations and act cordially with one another. In the first meeting, it is also good strategy to present the group’s case for the opening offer. Building the case might rely on national and regional data from the ASA on commercial payment rates. It might also include any quality measurement efforts in which the group is engaged. It is important to leverage available information to help build the case. The opening offer comes at the end of the case building. The payor representatives will guard their reaction to the presentation and offer. Realize that they do come in prepared as well.
During the early phase of the negotiations, it is not unusual to have several different counter-offers. In addition, look at the pie. Is it set in size or can it grow? How else can the parties slice up the pie for their mutual benefit? Does a group have to accept a standard type of offer? Or, can that offer be more creative? The planning phase has already provided the base line that the group will accept.
Once an offer is accepted, it is time to celebrate. It is easy to overlook celebration if there has been an adversarial relationship. However, it is important because of the emotional investment made prior to, during, and after the negotiations. It helps both parties to celebrate a win. In the end, the contract must be a win for both parties or it is not a winning contract.6
Arne Pedersen, MBA, FACMPE, serves as Director of Client Services for ABC. He is a Fellow of the American College of Medical Practice Executives. His distinguished background includes serving as a former Anesthesia Group Administrator, an expert on leadership, and a Bronze Star Medal recipient from the Persian Gulf War. Mr. Pedersen authored the book, “Lead with Intent” a comprehensive, yet practical leadership bible with a vision of training leaders. Mr. Pedersen serves an adjunct professor at the University of Notre Dame in the Executive Education Certificate Program and teaching Performance Management.
1 Sun Tzu, The Art of War,
2 Rasiel, Ethan M. and Paul N. Friga, The McKinsey Mind, McGraw-Hill 2001, pp. xv-xvii
3 Pedersen, Arne, Lead with Intent, IBJ 2007, pp. 73-74
4 Fisher, Roger and William Ury, Getting to Yes, Penguin Books 1991, pp. 57-80
5 Id., pp. 18-19
6 Id., pp. 147-148 -
The AQI: Present and Future
Richard P. Dutton, MD, MBA
Executive Director, Anesthesia Quality Institute, Park Ridge, ILThe Anesthesia Quality Institute was chartered in 2009, and it began collecting case data in the National Anesthesia Clinical Outcome Registry (NACOR) on January 1, 2010. NACOR was designed to harness the power of the Information Age by aggregating and analyzing large quantities of data. Unlike traditional registries that depend on a trained abstractor to examine medical records and pull out the facts of interest, NACOR accumulates data by direct reporting from the electronic health records (EHR) that are in use every day, including administrative systems such as the ABC billing software and clinical support systems such as ePreop. As anesthesia practices become increasingly digital — driven by the “meaningful use” requirements of the federal government discussed elsewhere in this issue of the Communiqué — even larger quantities and types of data will be available. The barrier is no longer the creation of digital records; it is now the enormous challenge of putting this mass of information to work. Here’s how the AQI is moving forward:
NACORMore than 150 anesthesia groups now participate in NACOR, representing 38 states and a broad range of practice types and styles. About 100 of these groups are submitting clinical data, providing information on every case, every day. NACOR now includes information from 4,500 anesthesiologists and 3,500 nurse anesthetists, working in 1100 facilities. Medium sized community hospitals (100-500 beds) represent the largest group of facilities and contribute the greatest number of cases, but NACOR also includes large and small community hospitals, university medical centers, specialty hospitals, attached and freestanding ambulatory surgery centers, pain clinics and office-based practices (Figure 1). As of April 1, NACOR includes more than 4,000,000 cases. NACOR has doubled in size in the past four months, and will double again by the end of 2012. Perhaps even more important, NACOR is growing in depth as well as breadth. More than 85% of cases submitted now include some kind of process or outcome measure and 20% include detailed clinical information from an Anesthesia Information Management System. The ability to link patient risk factors and intraoperative anesthetic decisions to long-term outcomes is the key analytic step that will power improvements in care. In a nutshell, this is the mission of the AQI.
While the AQI has many stakeholders, and receives numerous requests for data and analysis, the most important reporting we do is back to our participating practices. Each group contributing data to NACOR can log in to the AQI Reporting Server at any time to see both their information and how it stacks up against national benchmarks. The “data map” for a typical practice report is shown in Table 1 on page 12. Each element is presented as an individual graph and table, which the practice can slice and dice using drop-down boxes and filters to produce custom displays, down to the level of individual facilities,surgical case types, and providers. At the highest level, data from NACOR allows the practice to understand its own performance and track it over time. At a more granular level, access to this data allows practice managers and researchers to find information specific to whatever administrative, business, quality or scientific questions are most relevant to them. This might include the average duration for a particular kind of case, the difference in postoperative nausea and vomiting between inpatients and outpatients, or the number of cases done per provider per month at a new facility.
AIRSA second AQI registry, launched in October 2011, is the Anesthesia Incident Reporting System, or AIRS. This is a national collection of unusual occurrences, near misses, and serious adverse events, collected confidentially direct from the bedside. Any anesthesia provider can contribute to AIRS, simply by accessing the website at www.aqiairs.org. Reporting to AIRS is legally protected from discovery by the AQI’s status as a federally-designated Patient Safety Organization. Aggregated data from AIRS is used to identify emerging risks to patient safety at an earlier point in time than traditional mechanisms such as FDA surveillance or the Anesthesia Closed Claims project. Aggregation of rare events nationwide will provide early warning of new risks, and a mechanism for addressing them. De-identified cases from AIRS provide teaching material for a regular column in the ASA NEWSLETTER, a national-level morbidity and mortality conference that allows the many to learn from the experience of the few.
MOCA-PPAIAI
The newest AQI project is our partnership with ASA to create interactive modules for the Maintenance of Certification in Anesthesiology (MOCA) Practice Performance Assessment and Improvement (PPAI) requirements. Every participant in MOCA now has to make an assessment of their own practice – including clinical data from real patients – demonstrating a quality management problem that they have measured, addressed with new policies or practice, and then re-measured. The ASA modules will provide an easy-to-use format for doing this, focusing on the clinical issues that face us every day, such as monitoring in patients with sleep apnea or perioperative management of blood sugar. The AQI is providing a registry to collect and protect the clinical data entered by MOCA participants, and a reporting feature that will make it easy to document comparisons to national benchmarks and improvement in outcomes over time. For anesthesiologists in practices that participate in NACOR, the AQI will go a step further. We will soon be piloting a voluntary program that helps providers identify the cases they need to collect for their MOCA-PPAI project. In the long run this system will even auto-populate much of the required data.
Pain
Helping anesthesiologists in pain management practice keep track of their long-term outcomes is an important future goal of the AQI. This is a substantially different challenge than collecting data from perioperative care, which consists of easily defined events. Instead, pain management is a dynamic process that may extend over many years. Fewer standard definitions exist for good and bad outcomes, and electronic health records in this area are less sophisticated than in the operating room. Working with experts from the American Society for Regional Anesthesia and Pain Management (ASRA) we have laid out a template for data and definitions. The challenge now is to build those into existing EHRs in such a way that the data can be periodically transferred to the AQI without creating an undue burden of reporting for individual clinicians.
Research
Comparative Effectiveness Research (CER), defined as assessment of medications and techniques in a real-world practice setting, is increasingly recognized as an important approach to expanding scientific knowledge. This is because the artificial conditions of a highly-controlled prospective randomized clinical trial (RCT) may not adequately represent the real patients who will be exposed to a new product, creating the potential for unanticipated consequences once the product is approved for use. Further, the cost of performing a good RCT makes including large numbers of patients prohibitively expensive. In a very safe specialty such as anesthesiology, traditional scientific approaches will not have the statistical power to identify rare complications, or to show differences in safety between different approaches. In CER very large sets of data — such as those collected in NACOR — are analyzed to identify outcome differences resulting from common practice decisions in which there is natural variability in approach (e.g. the choice between regional and general anesthesia for lower-extremity orthopedic procedures). Other research topics of interest might be the rate of anaphylaxis to anesthetic drugs, the variation in surgical time associated with resident training, or the impact of quality management feedback on the occurrence of postoperative nausea and vomiting. The development of sophisticated statistical methodology for risk adjustment and propensity scoring has made it possible to advance scientific knowledge through the retrospective study of large clinical data sets. The AQI is positioned to facilitate this kind of research, and is actively seeking collaborators for future projects.
The AQI is growing rapidly in both size and scope, and is collecting more clinical practice information ever day. The challenge of the future is to turn this data into improvements in our practice that lead to better outcomes for our patients. We want your data, we want your ideas for reporting and research, and most of all we want your participation. You can learn more about the AQI at our website: www.aqihq.org.
Richard P. Dutton, MD, MBA is Visiting Professor of Anesthesiology, University of Maryland School of Medicine and AQI Executive Director. To contact Dr. Dutton or the AQI, visit www.aqihq.
-
Anesthesiologists Should Beware of HIPAA Audits
Neda Mirafzali, Esq.
Clark Hill, PLC, Birmingham, MIThe acronym “HIPAA” has become a household name since the enactment of the Health Information Portability and Accountability Act of 1996, which, among other things, established rules for protecting and securing patients’ health information. In fact, it is not uncommon to hear about breaches of patient information costing healthcare providers and suppliers six and seven figure civil monetary penalties or settlements. Typically, such settlements and penalties have arisen out of patient complaints that the privacy of their protected health information (PHI) has been compromised. However, beginning November 2011, patient complaints will not be the only way in which the Department of Health and Human Services (HHS) Office of Civil Rights (OCR) will learn about non-compliant entities.
Section 13411 of the American Recovery and Reinvestment Act of 2009, which established the Health Information Technology for Economic and Clinical Health (HITECH) Act, requires the Secretary of HHS to “provide for periodic audits to ensure that covered entities and business associates” comply with the requirements of the HIPAA Privacy Rule, Security Rule and Breach Notification Rule (collectively, the HIPAA Rules). To achieve this end, the OCR has engaged, under a $9.2 million contract, KPMG, LLC (KPMG) to conduct performance audits of covered entities in the form of a pilot audit program. The pilot will include up to 150 audits of covered entities to ensure compliance with HIPPA. The pilot program will conclude in December of this year.
Who Will be Audited
During this pilot program, covered entities of all sizes will be audited. According to the OCR, it “will audit as wide a range of types and sizes of covered entities as possible; covered individual and organizational providers of health services, health plans of all sizes and functions, and health care clearinghouses may all be considered for an audit.” Business associates will not be audited during the pilot, but will be included in future audits. A covered entity is defined as (i) a health plan, (ii) a healthcare clearinghouse, or (iii) a healthcare provider transmitting any health information in electronic form. As such, anesthesiologists, anesthesia groups, CRNAs, ambulatory surgery centers, physician offices and clinics electronically transmitting any health information are eligible to be audited by the OCR.
What Audited Entities Can Expect
Although the OCR will begin with roughly twenty (20) audits to test and finalize the audit protocols, audited entities can expect the HIPAA audits to include a request for documentation, an on-site field visit and a report. Initially, the OCR is using the audit process to detect compliance with the HIPAA Rules and identify best practices, and to discover compliance risks and vulnerabilities.
Step 1: Notification Letter
The OCR will send entities written notification letters. Included in the notification letter will be a request for documentation evidencing their HIPAA privacy and security compliance efforts. The OCR provided a sample notification letter on its website.1 Included in the sample letter is the following language briefly advising the audited covered entity of what to expect:
In the attached letter, KPMG LLP requests certain information be provided by you in order to facilitate the audit process. Additionally, they provide contact information for the audit firm personnel responsible for conducting the audit. Please recognize that KPMG LLP is requesting and reviewing these documents solely as a contractor to OCR and on its behalf and pursuant to its audit authority. This letter serves to notify you that the audit shall begin within the next 30 to 90 calendar days from the date of this letter. The results of the audit firm’s work, including your management’s written response to any reportable findings will be presented in a final report to OCR.
Audited entities will have ten (10) business days in which to provide the requested documentation.
Step 2: Receipt and Review of Documentation and Planning Field Work
After KPMG receives the requested documentation from the audited entities, it will review the documentation and begin planning the audit field work—the on-site visit to the audited entity. Following KPMG’s review, audited entities should expect KPMG to notify them within thirty (30) to ninety (90) days prior to the on-site visit.
Step 3: On-Site Visit
KPMG will send auditors to conduct on-site field work of the audited entities. Audited entities can expect the field work to span between three (3) to ten (10) days, depending on the size of the entity, the complexity of the audit and the auditor’s need to access information and personnel. The on-site field work will include interviews with the covered entity’s leadership (e.g., the compliance officer, legal counsel, health information manager, medical records director, etc.), examination of the physical space and operations, consistency of the entity’s practice with its stated policies and observation of the entity’s compliance with the HIPAA Rules.
Step 4: Draft Audit Report
Within twenty (20) to thirty (30) days following the auditor’s on-site review of the audited covered entities, the auditor will prepare a draft audit report of its findings. The draft audit report will include information regarding the timeline and methodology of the audit, the best practices noted by the auditor, and any other information and data collected by the auditor. The draft audit report will also include specific recommendations to the covered entity to address compliance problems identified during the audit.
Step 5: Review of the Draft Audit Report
After receipt of the draft audit report from the auditor, audited entities will have ten (10) business days to review the draft audit report and provide the auditor their written comments, concerns and corrective actions taken to address any potential violations of the HIPAA Rules.
Step 6: Final Audit Report
The auditor will revise its draft audit report and submit a final audit report to the OCR. Final audit reports must include the following information:
- Identification and description of the audited entity, including the entity’s full name, address, EIN, and contact person;
- The methods used by the auditor to conduct the audit;
- A review and description of each audit finding, which should include the following:
- Condition: The defect or non-compliant status observed by the auditor, and evidence of each defect or non-compliant status;
- Criteria: A clear demonstration that each negative finding is a potential violation of the HIPAA Rules, including a citation to the specific rule that is potentially violated;
- Cause: The reason why the condition exists, including an identification of the supporting documentation used to determine such cause;
- Effect: The risk or non-compliant status that results from the auditor’s finding;
- Recommendations for the audited entity to address each finding; and
- Corrective actions taken by the audited entity, if any;
- Acknowledgement of any best practice(s) or success(es) of the audited entity; and
- The auditor’s overall conclusion.
Audited entities can expect the auditor to take up to thirty (30) business days to submit its final audit report to the OCR.
What Anesthesiologists Can Do
While the OCR is conducting a limited number of audits during this year, anesthesiologists generally are not exempt from inclusion in this pilot program. This pilot period provides anesthesiologists and anesthesia groups with an opportunity to establish HIPAA compliance policies or to revisit existing ones. For those entities that have not had their policies updated recently, this may serve as a good opportunity to have their policies reviewed and updated as well as internally reviewing compliance with their own policies. Moreover, this may be a prime time for anesthesiologists, anesthesia groups and their staff to be trained or re-trained on HIPAA, the necessary requirements for compliance with the HIPAA Rules and consequences for breaching the HIPAA rules.
Anesthesiologists should also familiarize themselves with new risks and vulnerabilities for breaches of patient information. For instance, one such new risk or vulnerability includes the appearance of patient information on social media sites. Anesthesiologists should familiarize themselves with the implication of social media sites and should educate their staff on the proper and improper use of social media in a professional healthcare setting. Another example of increased vulnerability is the use of portable storage (e.g., a flash drive or a thumb drive, laptops, etc.) devices to transport unencrypted patient information. Most breaches of patient information are unintentional. As such, anesthesiologists should be aware of existing and emerging risks and take measures to guard against such risks.
Lastly, anesthesiologists can expect HHS to issue new rules on breach notification this year, finalizing its Interim Final Rule issued in August 2009. Anesthesiologists should ensure that the new rules are incorporated into their compliance policies.
Conclusion
Most anesthesiologists will not be audited during this year; however, those that are can expect a request for information, an on-site visit and an audit report of the findings. Regardless of whether an anesthesiologist is audited, all anesthesiologists should take this opportunity to dust off their HIPAA compliance policies and ensure they reflect the most updated regulations that have been issued.
Neda Mirafzali, Esq. is an associate with Clark Hill, PLC in the firm’s Birmingham, MI office. Ms. Mirafzali practices in all areas of health care law, assisting clients with transactional and corporate matters; representing providers and suppliers in health care litigation matters; providing counsel regarding compliance and reimbursement matters; and representing providers and suppliers in third party payor audit appeals. She can be reached at (248) 988-5884 or at nmirafzali@clarkhill.com.
1 http://www.hhs.gov/ocr/privacy/hipaa/enforcement/audit/sample-ocr_notification_ltr.pdf





 If you submit claims to Medicare and other payers electronically – and you all do – you can automate the upload of data to the AQI with relative ease. AQI staff are ready to work with you whatever claims software you may be using. ABC is proud of our AQI Preferred Vendor status and we encourage every client who has not already asked us to submit their information to NACOR to do so.
If you submit claims to Medicare and other payers electronically – and you all do – you can automate the upload of data to the AQI with relative ease. AQI staff are ready to work with you whatever claims software you may be using. ABC is proud of our AQI Preferred Vendor status and we encourage every client who has not already asked us to submit their information to NACOR to do so. Identify
Identify Options
Options NACOR
NACOR AIRS
AIRS