eAlerts
-
Journey to Quality: Quantum Clinical Navigation System
Ruth D. Morton, Ph.D.
Vice President, Anesthesiologists Associated Inc.
Background
More than ten years ago Southeast Anesthesiology Consultants (SAC) Chairman and CEO Richard L. Gilbert (MD, MBA) faced a challenge—making sure surgeons recognized that anesthesiology providers were not the cause of delays and cancellations in the OR. While surgeons could provide only anecdotal cases it was clear that having all the data was essential. This led his group to start a methodical process of incident-based data collection on every case. The process of tracking every patient and measuring the causes of cancellations and delays allowed SAC to prove that the anesthesiologists were rarely the cause of the problem. Not only could the group pinpoint the causes of delays and cancellations but also the system facilitated further opportunities for improvement. This marked the start of the group’s “journey to quality.”
A few years later the Institute of Medicine published To Err is Human, which revealed that as many as 98,000 hospital patients die each year from preventable medical errors (Institute of Medicine, To Err is Human: Building a Safer Health System, 1999). The publication captured the attention of SAC members, and they saw opportunities for improving care provided through their practice. Near that time the group decided to send Dr. Gilbert to an MBA program, where he learned about quality improvement methodologies such as Six Sigma and the Deming Cycle. He worked with his group to apply these quality concepts and tools to their practice. Together they defined metrics, tested them, and refined a data collection tool, resulting in a patient focused and systems oriented approach to quality improvement.
Along with the data collection tool and the software to store and report the data, SAC developed the infrastructure to support their journey to quality. They:
- created a Continuous Quality Improvement (CQI) Committee (at each site and corporate-wide) that reviews results,
- selected a Quality Director who oversees the overall process and facilitates its coordination,
- hired and placed QA nurses at high volume locations who work seamlessly in the hospital environment, function as members of the anesthesia department, monitor the data-input process and collect data on patient satisfaction,
- initiated email alerts that go to practitioners when they’ve exceeded thresholds on quality indicators, or to practitioners, or to the CQI Committee and department chief upon critical events (i.e. stroke or cardiac arrest), and
- developed educational materials, interventions, and mentoring processes that help providers learn better and safer techniques and protocols.
Results
Today SAC, a 75+ member group that practices in North Carolina, South Carolina, and Virginia, is proud of their investment in quality improvement and the results they have achieved throughout their journey. Their CQI software is now called the Quantum Clinical Navigation System™ (Quantum CNS). The patent-pending process includes a 50-indicator checklist that tracks patient satisfaction, OR efficiency, practitioner performance, and clinical outcomes along the Perioperative care continuum. “Ultimately”, says Dr. Gilbert, “doctors and nurses want to deliver outstanding care, and this helps them do it. The Quantum Clinical Navigation System™ provides real time positive and negative feedback loops to individual providers to improve their practice. In addition, the data collected in aggregate across the group is analyzed and along with evidence based medicine, provides the foundation for a systems approach to decreasing medical errors. Our focus has been on demonstrable quality customer satisfaction and efficiency; this has given us the ability to quantify and continually improve. It drives our practice and supports the growth of our business.” He adds: “The real mileage comes from the group taking the information to implement system-wide best practices.”
Tangible
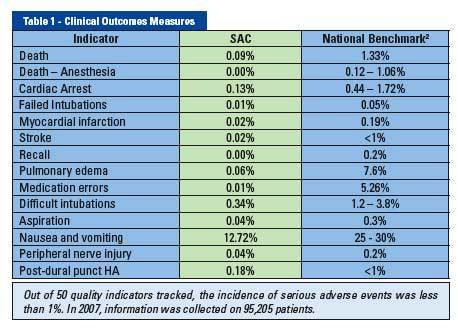
2 National Benchmarks from the IOM Report, MEDLINE, and Evidence-Based Practice of Anesthesiology
By implementing this system, SAC has achieved consistently high results for patient satisfaction (patient satisfaction scored in the high nineties over the last 8 survey years) and consistently exceeded national benchmarks for error reduction and improved outcomes (see Table 1).
In addition to exceeding national benchmarks, SAC’s efforts have tangibly paid off in an 8-10% reduction in its medical malpractice rates in each of the past two years. They have used the lower complication rates reported by Quantum to demonstrate cost savings to managed care companies supporting better reimbursement rates for the Group. The value the group has shown helped them win business with hospitals that are focused on CMS initiatives and on attracting surgeons. Dr. Gilbert notes that approximately 65% of hospital revenue and profit is from the OR. Although anesthesia is small in terms of cost to the hospital, it is a lynchpin to its overall success. And surgeons want skilled anesthesiologists in the OR. As reported in the Clinical Advisory Board Essay, 57% of responding surgeons scored “availability of skilled anesthesiologists” as extremely important, among the top three attributes of 47 possible (Clinical Advisory Board Essay: The State of Hospital-Physician Relations, 2003, p.54). SAC has the data to prove their skills.
Intangible
While the group’s journey to quality has resulted in economic gain for all stakeholders, the journey for individual practitioners has intangible rewards, as well. Overall, providers are pleased with getting rapid and detailed results (data are collected real-time, not by claims data or retrospectively) so they can take timely and effective action. For example, a new group member exceeded a threshold shortly after he started practicing with the group. His high incidence of wet taps was captured by the Quantum Clinical Navigation System™. The provider was then mentored by a skilled peer who taught him better technique. The physician recognized the technique issues, and was glad to get help and support that was provided in a positive manner. Improved epidural outcomes were also captured by Quantum and tracked for continual assessment. Quality Director Janet Beck notes that the use of Quantum Clinical Navigation System™ resulted in timely identification of the issue, intervention, and ultimately behavior change. Without a mechanism for early intervention, the physician may have improved his technique over time, but it would have taken longer and affected more patients.
Another example of an intangible reward was at a location having lower scores for labor pain control in OB. A team including the department chief, QA nurse, and the quality director analyzed the data and found differences between anesthesia providers. This led to the physicians at the location (those with higher and lower scores) talking among themselves. Their collaboration and teaming led to lower scoring doctors recognizing the differences in how they were treating labor pain. The care team also found out that nursing staff needed to better educate the patients on use of the IV pain medication control. Subsequently, the patient satisfaction scores went up significantly in only three months for that location.
Hospital Partnership
In an era when hospitals are under the pinch to achieve quality measures, they ask for quality anesthesia practitioners who can help them achieve certain CMS-SCIP, JCAHO, and IOM initiatives. Southeast Anesthesiology’s use of their Clinical Navigation System™ has given them a head start in providing necessary data for hospitals where they practice. With the trend toward transparency of outcomes, data from Quantum has helped SAC partner with hospitals to deliver outstanding care. And, Quantum CNS has been a vehicle for providing evidence that stipends paid to the group are worth it for the hospital.
Data from use of Quantum CNS has helped physicians and hospitals implement best practices such as:
- standing orders for pain control
- process improvements to minimize central line infection
- early eye protection protocol to prevent corneal abrasion
- implementation of obstructive sleep apnea protocol
- improved labeling to reduce medication errors
- clinical initiatives to reduce anesthesia recall
- protocols to improve control of labor pain
- protocols to lower the incidence of post op nausea and vomiting
Educational Approach
Quality Director Beck believes that Southeast’s leadership in educating physicians is one of the keys to the success of the quality program at SAC. She emphasizes:
- the quality process and the cycle of quality improvement,
- peer review and its importance, and
- Pay for Performance — why it is coming and how to prepare.
Ms. Beck indicates that data generated through use of Quantum CNS is used by SAC in an educational way. Improvement is achieved through learning—the use of mentors, educational materials, and processes. For example, they have created educational modules for sleep apnea and preoperative beta blocker administration. The data is not used for punitive purposes. If a threshold is exceeded and the system sends an automatically generated alert that a practitioner is not following a protocol, the individual is given a set of educational slides to review. Or, in the case of an individual with low patient satisfaction scores related to communication skills, the physician may attend a series of educational communication sessions, and scores are monitored for a time following the educational sessions. Ms. Beck relays that it is “very gratifying for individuals to see improvement on their measures.”
Over the years of their journey to quality, there have been challenges. The initial challenge was inertia – the usual phenomena of resistance to change, even when the change is considered good. Then practitioners doubted the completeness of the data until they understood that it was not just sampling. A third challenge was getting providers to change behavior based on the data. And, a final challenge was getting members to believe the improved results. A sound scientific approach combined with a positive, non-punitive educational environment successfully guided the practice through these challenges. Continuing the education of nurses, CRNAs, and anesthesiologists, with Quantum CNS providing data to drive the practice, has successfully led the group members to see themselves as a “high performance practice.”
Quantum CNS Available to Anesthesia Groups and Hospitals
In 2008, SAC entered into an agreement with Anesthesia Business Consultants to make Quantum CNS available to ABC’s existing billing clients and to promote it to anesthesia groups and hospitals nationwide.
Small to large anesthesia practices and hospitals can avail themselves of the benefits of this CQI software without investing the time or money to develop it. It can be purchased as a package with their ABC billing services, or as a stand-alone service through licensing and per case fees. Dr. Gilbert states that critical mass is not necessary to implement Quantum CNS and infrastructure needs are limited. From a user perspective, it does not take much time to learn or to enter the data. However, what is necessary is the commitment from group or hospital leaders to embrace the journey to quality.
Quantum CNS is currently in use at Carolinas Healthcare System in North Carolina, Sentara Hospital System in Virginia, and Community Health Systems in South Carolina. The system, designed by clinicians for clinicians, has been field tested at these sites, which range from tertiary-care medical centers to rural hospitals.
Why Might Oher Hospitals and Anesthesia Groups Want to Use Quantum CNS?
Among other reasons, Gilbert writes that “Every health care provider in America wants to assert that he or she provides high-quality services. The proof is in the results. Also, it is clear that pay for performance is here to stay. Embracing a rigorous CQI program that integrates a systems approach to clinical care, quantifies key metrics, and communicates them effectively can position medical groups to turn the potential threat of pay for performance into an opportunity.”(MGMA Connexion, September 2006, page 24)
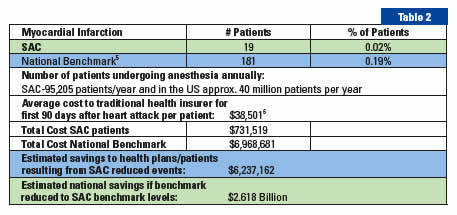
Return on Investment
The return on investment for a program such as this benefits all parties including patients, providers, hospitals, and managed care companies. Savings on just one indicator alone—Myocardial Infarction—of the 50 indicators in Quantum CNS are calculated in Table 2.
5 Chung, Dorothy and Stevens, Robert, Evidence-based Practice of Anesthesiology, page 379.
6 NBER Working Paper No. 6514, nber.org/digest/Oct 98, National Bureau of Economic Research
High-Performance Healthcare
The use of Quantum’s Clinical Navigation System™ creates an environment where medical professionals and institutions can achieve true high-performance healthcare – the reason behind the journey to quality. On the journey, you can reduce medical errors, change clinician behaviors, enhance quality of care, run more efficient OR operations, maximize managed care reimbursement, and even lower malpractice insurance premiums. And, Quantum CNS paves the path toward Pay for Performance.
For more information
To get more information and to explore how you can start or continue your journey to quality using Quantum CNS, contact Anesthesia Business Consultants at 517.787.6440, Extension 4113.
-
Taking Control
Tony Mira
President and CEO, ABCAs I suggested in my last column, the summer should be a time to rest up and plan your strategy for the balance of the year. There must be a reason why Halloween comes in the fall. This is often the time when some unforeseen circumstance or sequence of events seems destined to undo all our best laid plans for the year. Certainly the recent events on Wall Street bear testament to the truth of this.
It has always been my belief that we always have a choice. We can complain about the unanticipated complications that are the source of such frustration to so many of our clients or we can choose to take control of our circumstances. While this is often easier said than done, experience has taught me that every cloud does, indeed have a silver lining if you are willing to look for it. Take our business. As I constantly tell our employees when they grumble about how hard it is to get paid properly from certain payors: “If it were easy our clients wouldn’t need us!”. The same can be said for providing a comprehensive anesthesia or pain service. If it were easy, the hospitals wouldn’t need you! As is the case for us, the key is to remind administration just how complicated it is and to make it clear why and how the service you provide is the most appropriate for their needs.
I can only hope that some of the very timely and insightful articles in this issue of the Communiqué will help you accomplish this noble goal. We have been interested in Dr. Gilbert’s approach to quality management for quite a while and consider ourselves fortunate that Southeast Anesthesia Consultants has chosen to partner with ABC in the distribution of the Quantum product, because it embodies the spirit of taking control of your own destiny in the operating room. Certainly no one has more insight into the challenges of hospital contracting that Mark Weiss, Esq. and we are grateful to him for his sage advice and guidance. By the same token, Abby Pendleton, Esq. lays out exactly what you need to know if you want to take control of billing compliance and ensure that your practice is never compromised by non-compliant documentation and billing. As important as these previous articles are, be sure to pay special attention to Paul Kennelly’s discussion of ways to make your relationship with your billing service work consistently. His insights and suggestions only underscore our rationale in making him part of our team. After all when it comes to the service business there is nothing more important than setting realistic expectations and staying in communication. We are also glad, once again, to be able to include comments by Shena Scott. We are great believers in and supporters of the MGMA and its AAA. An MGMA membership is definitely a good way to maintain the upper hand in managing your practice. No matter how interesting all the other parts of this issue may be, Karin Bierstein’s review of locums rules is especially timely and relevant.
I know there was a time, at least so many older anesthesiologists like to say, when they could show up, provide good care, and go home at the end of the day knowing that they had made a difference in patients’ lives and a good living. Many now complain that they feel frustrated on both counts. Change tends to have that effect on all of us; we long for the good old days. As is so often said, very often the beliefs and strategies that got us to where we are today will not get us to where we need to be tomorrow. It can be a hard reality to accept and so we persevere by analyzing the trends and anticipating the future. The good news is you are never alone. As this collection of articles should clearly attest there are lots of good ideas; you just need to make sure they are your good ideas.
Please let us know if we have hit the mark with this collection of practical tips and professional advice. I have long submitted that being committed students of this industry is the only thing that makes us successful in this business. Let us learn together and continue to share the insights and best practices that distinguish the most successful strategies for continued success in the ever-changing and always challenging business of healthcare.
Thanks for your continued support.
-
Working with Your Billing Service—A Practice Administrators View
Paul Kennelly
Regional Director, Practice Services, Anesthesiologists Associated Inc.As a practice administrator I had a narrow view of the internal working of our billing service. Like many, my focus was on monthly collections and the standard benchmarks. Some Groups operate with an understanding that billing boils down to a charge entry and collections. It was not until I joined a billing company as Director of Practice Services did I begin to appreciate that the billing and collection function is not that simple. To maximize revenue, and enjoy consistent / stable collections, both the group and billing company must work closely together.
Technology left its mark on anesthesia billing with electronic scanning of charge data and correspondence and the development of sophisticated billing software that can monitor multiple aspects of the practice. But at the end of the day, billing and collection is a people intensive business with technology providing advanced tools to make the process more efficient and cost effective. Medical practice billing is like few other industries dealing with multiple payers, complex rules, and a lack of standardized payment methodologies among Health Plans make successful billing and collection a never-ending marathon. What other industry allows payers to deeply discount or unilaterally deny services simply because they do not think the procedure was necessary? Where else would you find rules allowing payers to send your professional services payment directly to the customer (patient) while at the same time lowering your fee just because you do not have contract with them? All this leads to what might seem like an obvious point… anesthesia groups need to have a close working relationship with their billing agent.
Expectations. The word conjures all manner of images, but establishing and managing expectations is the cornerstone to long-term success. If the group is switching billing services, establishing clear expectations for both parties is critical. Too frequently a lack of understanding of the goals and objectives lead to misunderstandings and dissatisfaction. If the relationship is new, this frank and candid conversation should happen before the deal is finalized and if the relationship is seasoned, practices and billing companies should annually revisit the scope of services, performance, and measures of success.
The reality of today’s anesthesia reimbursement environment illustrates another critical component of a successful relationship…contracting. Whether the group does its own health plan contracting or has the billing service do it, there must be a close partnership between the parties. Too many practices focus on the conversion rate and while it is true the bulk of their revenue comes from anesthesia services it is important to establish strategies for non-timed procedures (flat fees), physical status modifiers, qualifying circumstances, and OB epidurals. A billing service that can help a practice assess these areas, incorporate them into the contract’s reimbursement schedule, and track them for proper payment provides an invaluable service to the practice. Clarity of purpose and agreement on these important issues helps develop a contract portfolio designed to maximize all sources for payer reimbursement.
As noted earlier, the most sophisticated billing software is no substitute for hands-on account receivable management. Here too the interdependence between practice and billing company is vital. For anesthesia billing, the old adage, “Garbage in – garbage out” is not a cliché, but a reality. Some group responsibilities include:
- Notifying the billing service of new hire well in advance of their arrival provides ample time to meet the myriad of credentialing requirements for commercial and government carriers. Credentialing can take 4-6 months and waiting to the last minute only means delay in payment or possible outright denial of services.
- Notification of a change in the group’s billing rate. Failure to tell the billing agent of a rate increase means charges are understated resulting in rebilling and delay in payment.
- Changes in contract rates. Without telling your billing company of a rate change from a health plan, they will have no way to accurately monitor over/under payments.
- New payer contracts. Failure to notify the billing company of a new contractual relationship results in false-positive underpayments and could distort the group’s payer mix numbers, because the payer is now in another payer category. Billing services use contracted and non-contracted payer information to help determine the groups expected payments. Incorrectly classified payers alter payer mix information.
The need for communication is not limited to the physician group. Billing services have a role to play as well such as:
- Notifying the practice of new programs such as the Physician Quality Reporting Initiative (“PQRI”). The billing company should help explain such programs and assist the physicians in reporting and tracking their performance.
- Ensuring groups know about changes in health plan reimbursement strategies. The fervor over the medical necessity of GI anesthesia is a good case in point.
- Providing an impact analysis of reimbursement changes in government programs such as Medicare and Medicaid.
- Notification of health plans that consistently pay claims incorrectly. This includes chronic overpayments which represent a potential liability to the practice. Its one thing to recover a large underpayment from a Plan, but an entirely different matter to refund a large overpayment without knowing it was lurking in the mist.
Lastly there is the matter of day-to-day practice management issues. Whether the practice employs an administrator or not, life can be far more enjoyable if you share the load. Over the years, national firms such as Anesthesia Business Consultants (“ABC”) recognized the need to help physicians manage their practices. It is an unfortunate fact of life for anesthesia practices that the day-to-day aspects of group practice are increasingly demanding and complex. Issues such as the demand for more OR coverage without commensurate compensation, governance issues, shareholder/partnership track, retiring group members, compensation plans, call coverage, and downward pressure on hospital stipends are no fun to address after a long day in the operating room. A billing service with seasoned practice administrators provides an invaluable asset to the practice. What is truly unique about this model is that practice management departments operate inside the billing company, and as such have an opportunity to help resolve issues and recognize trends early. Cynics will say that billing company practice managers do not have the best interest of the physicians at heart, but reputable billing companies realize that strong practice management departments can strengthen the relationship with the physicians. It is this ombudsman approach that helps the practice manager ensure the billing service stays focused on their core competency and also ensures that the practice provides critical information to the billing company allowing both parties to meet expectations.
-
Positioning Your Group For Exclusive Contracting Success
Mark F. Weiss, J.D.
Advisory Law Group, A Professional Corporation Los Angeles, CA, Santa Barbara, CAWoody Allen quipped that eighty percent of success is showing up. That may well be true, but simply showing up is not enough: Success requires thorough preparation and positioning.
Yet many anesthesia groups think that they’ll have a successful negotiation of an exclusive contract, or even more so, a successful renewal negotiation of their existing exclusive contract, without much preparation other than having been in place at the facility for a number of years.
I admit that it might be possible to achieve mediocre results without proper preparation. I don’t know about you, but my clients are looking for spectacular results.
Thorough preparation requires far more than reviewing the current agreement and doing a few months, even six to nine, of planning. It requires an integrated series of thoughts and actions to position the group for an optimal result.
Achieving a highly favorable exclusive contract, for example, financial support in the multi-million dollar a year range, requires developing a strategy that unfolds tactics over a multi-year period. It requires coordinating exclusive contracting strategy with overall strategy. And it requires coordinating various contracting sub-strategies, and their ensuing tactics, with the group’s exclusive contracting strategy.
There’s a common misperception that negotiation is like chess, but that’s far from the case. If you must think it’s like a game, then it’s more like three dimensional tic-tac-toe, a set of three boards stacked one on top of another. The moves occur in at least all three dimensions of physical space. I say “at least,” as negotiation also involves a fourth dimension, time, as well as a fifth dimension, the mind of your opposition.
In fact game theory is flawed in application to complex, real life negotiation: Game theory requires that there be a set of rules. Negotiation often plays out, like life in general, with rules being broken and with new rules being made up all the time.
Let’s look at two case studies, both real-life situations, one in which a group takes the path well traveled toward the precipice and the other in which a group seeks to control its destiny.
We’ll call the first group the Jones Group. Pursuant to an exclusive contract, it has been providing all anesthesia services at a large community hospital for over a decade. Jones Group does not receive any stipend support from the hospital. Its physicians’ incomes have been slipping for several years.
For more than a year, Jones Group’s leaders have been meeting with the hospital’s administration in an attempt to get stipend support. They have been stonewalled and then told outright that the hospital will never pay a stipend for anesthesia services. Nonetheless, they continue to provide services as usual and to argue, in essence, that since groups at other hospitals receive stipends, they should, too.
Even though only a few months remain on their current exclusive contract, they insist on continuing the same course of action: presenting yet another proposal to the hospital demonstrating that similarly situated groups receive stipend support.
The presentation of evidence that other groups receive support and data concerning the discrepancy between the group’s physicians’ earnings and those of the market are central to the issue of a fair market value analysis, which is a key issue in the context of arriving at the amount of stipend support. However, it is wholly ineffectual as the sole strategy to move the hospital off its position of refusing to discuss financial support at all. The hospital continues to refuse to budge. The group has done nothing to position itself. The negotiation is over.
Let’s contrast this with the experience of the second group, which we’ll call the Smith Group. Pursuant to an exclusive contract, it, like the Jones Group, has been providing all anesthesia services at a large community hospital for over a decade.
For several years, Smith Group received a token amount of medical director stipend support at a level that might buy a domestic luxury car. The hospital was not interested in discussing any other stipend support. Its physicians’ incomes were slipping and doctors were leaving the group.
Working with Smith Group we implemented a multi-year process of positioning the group to obtain a strengthened bargaining position leading to greater independence and increased financial support. Elements of the process included acquisition of data and intelligence, control of publicity, creating bargaining leverage, framing the issues, and emasculating potential competitors.
Through taking the time and exerting the effort to develop an overall strategy, align specific elements of contracting strategy back with that overall strategy, and implementing tactics at each of the group, medical staff, community, and administration levels, we positioned Smith Group such that the renewal brought it millions of dollars per year of stipend support over a multi-year term.
Continuing with the car analogy, Smith went from the level of a Cadillac to seven Ferrari 599s, with change to spare. Yes, Smith Group invested significant dollars to accomplish this result, but the return on investment was 1,100%.
Achieving spectacular contracting results requires that you take a holistic approach: What’s the best negotiating strategy? In reality, there is no independent negotiating strategy; it’s but a part of a larger, overall group strategy. Contracting strategy is inexplicably linked to governance strategy, to the way in which the group relates to non-owner physicians, to the compensation plan, to the patient experience, to the manner in which it contracts with third parties, to the way in which it gathers billing data, and on to every other element of its business existence.
Returning to the example of the Smith Group, it began implementing this Strategic Representation™ process in respect of its next renewal a few weeks after it signed the current exclusive contract.
This process has no relationship to the usual “benchmarking to best practices.” Far too many groups are oblivious to the opportunities and, as a result, benchmarking leads to the mediocre.
The specialty of anesthesiology is facing severe challenges: increasing commoditization, competition from independent para-professionals, and downward reimbursement, to name but a few. A “benchmarking” lemming still goes over the cliff, he just gets there a bit faster than some of the others. Success, even survival, lies in running in the other direction.
Mark F. Weiss is an attorney who specializes in the business and legal issues affecting anesthesia and other physician groups. He holds an appointment as clinical assistant professor of anesthesiology at USC’s Keck School of Medicine and practices nationally with the Advisory Law Group, a firm with offices in Los Angeles and Santa Barbara, Calif. Mr. Weiss provides complementary educational materials to our readers. If you would like to reach Mr. Weiss, please contact him directly at markweiss@advisorylawgroup.com.
-
The Value of MGMA AAA Membership
Shena J. Scott, MBA, FACMPE
Executive Director, Brevard Anesthesia Services, PA, Melbourne, FL and Immediate Past President, MGMA AAAAs a 17-year veteran of anesthesiology practice administration and past president of the Anesthesia Administration Assembly of the Medical Group Management Association (MGMA AAA) I am often asked by physicians and those new to the field, “what is MGMA and what is the value of MGMA membership?”
To answer this question, I go back to 1991 when I was not only new to anesthesia but also new to medical group practice administration. With a background in business and finance and no medical group experience whatsoever, I was recruited to the forward thinking group where I still work because they saw on the horizon that medicine was about to become more of a business. The 18-physician group had an office manager with lots of anesthesia billing experience but no business background. Anticipating the office manager’s retirement within a few years, they wanted to hire someone with a business background, figuring that the “medical group management” part could easily be learned. And what a learning experience it has been, and continues to be, thanks largely to MGMA AAA.Knowing nothing about medical group practice management, let alone anesthesiology practice management, I was fortunate to have stumbled across MGMA AAA very early on. With three months in my new job (where I was just beginning to understand what a CRNA was) under my belt, I headed off to their conference in Scottsdale, where I found one of the most welcoming groups of people I had ever met. I was immersed in anesthesia specific content and engulfed by a group of people willing to share their wisdom and experiences. I left that three day meeting with a spinning head, a handful of business cards and a whole new group of friends, whom I often called upon whenever I became stumped. From that day forward, I have missed only one MGMA AAA meeting. Today, these meetings have a different feel for me because I am now one of the “old timers.” Yet I continue to learn many new things every single year, not only from the meeting content but also from my colleagues, who are now my friends. And now I have an opportunity to “give back” to others who sit where I sat back in Scottsdale.
In 1991, the MGMA AAA conference was about the only time we could get together to network and share experiences. Individual phone calls in between helped “fill in the gaps.” In today’s world, however, in addition to the yearly meeting (which continues to be the glue that solidifies the network), MGMA AAA also offers anesthesiology specific Webcasts, an email forum (which is getting ready to morph into an enhanced social networking tool that will dramatically expand its possibilities), anesthesia specific surveys, a page devoted to anesthesiology on the MGMA Web site, periodic anesthesiology-specific e-newsletters, and collaboration with/ support to the American Society of Anesthesiologists (ASA) in key legislative and other efforts.
In addition, MGMA also offers an annual conference which focuses more on general professional development and medical group practice management, a magazine called MGMA Connexion, a Government Affairs office that devotes its energies specifically to medical issues, a variety of surveys and other products and services which are available both for sale and through the library, and a certification body in the form of the American College of Medical Practice Executives (ACMPE). Many of these services are included in the basic membership price. Surveys are free if you participate. Surveys in which you do not participate, as well as other books and resources, are sold to members at a significantly reduced price. Also, Members receive discounted registrations to MGMA events.
I often tell people who are new to anesthesiology administration, physicians included, that the MGMA AAA email forum alone is worth the price of the membership. Aside from the MGMA AAA email forum, there are also many other email forums that members can participate in, such as financial management, information technology, human resources, payer contracting, etc. Back in 1991, the MGMA AAA email forum was not available, but today it is the lifeblood of ongoing networking. For a person new to anesthesiology administration, it is priceless. Yet, even as a 17-year veteran, there are many times when I encounter something that I have not seen before. I could spend a lot of precious time researching it myself, or I can just throw it out there on the email forum and get feedback from others who have already had the experience. The generosity of information sharing is just as prevalent on the email forum as it is during annual meetings. Many of the physician leaders of ASA, as well as nationally recognized anesthesiology attorneys and consultants, participate as members on the MGMA AAA email forum and provide relevant and helpful insight.
One of the things I have found over the years is that it is amazing how similar the issues are that we all face. Large practice, small practice, employed CRNAs, non-employed CRNAs, no CRNAs, outside billing company, in-house billing — many of the issues we face are the same. We all have to negotiate contracts with managed care companies and our hospitals; we all face recruiting and scheduling issues in a tight market; we all face budgetary pressures, coding and billing issues, the list could go on. Some of us have pain clinics, some are in academic practices, and of course there are regional issues as well. Some people ask for advice/feedback about specific vendors, others post “articles of interest” to the anesthesiology community. There is no question too technical or too basic for this group, and the wealth of information that is readily available, even to the most seasoned administrators and physicians, is endless.
The new social networking tool, MGMA Member Community, will only enhance these capabilities, as it will allow sub-groups to form by area of interest, region, group size, or just about any other common characteristic a member wants to identify. People will be able to start a “pain blog,” for example, or a “Florida blog,” or even a “pain Florida blog,” where they can post questions and items of interest specific to that topic. For those who are familiar with Facebook and My Space, this is the general idea of how it will function.
Another significant development over the last several years is the addition of anesthesiology specific survey information. For years, MGMA has published the Physician Compensation and Production Survey, which reports anesthesiology-specific and pain management specific compensation data, and is a critical reference for many anesthesiologists as they negotiate support for non-compensated services with their facilities. In recent years, MGMA AAA has worked with the survey department to put together the Cost Survey for Anesthesiology and Pain Management in collaboration with ASA. That survey breaks down data in a number of ways (e.g. by staffing model) that are specific to anesthesiology and provides valuable statistics that cannot be found elsewhere, like revenue or units per anesthetizing location. In 2006, a pain management section was added and the 2009 survey will feature a section specifically for academic anesthesiology practices. More on this will appear in a future article when the surveys are getting ready to come out, but remember, if you want to obtain a free copy, you can do so simply by being a member and participating.Another way to add value to your membership is to become board certified (or have your medical practice administrator do so), and then a fellow, through ACMPE. MGMA offers a wealth of resources to support the Body of Knowledge for Medical Practice Management required to pass the exams. Studying this Body of Knowledge to take the exams provides an opportunity to expand knowledge that stays with you, and brings value to your professionalism and your practice as you apply it to your day-to-day responsibilities. Becoming a fellow involves in-depth research of a topic pertinent to the profession (you can choose an issue that your practice is facing, research it, write the paper, sharing your knowledge and becoming a fellow in the process). All of the fellowship papers are available as resources through the MGMA library. They span everything from human resource issues to financial management, risk management, business operations, and patient safety. This is another valuable tool available to members. Members of the college also receive quarterly summaries of new fellowship papers.
The website, www.mgma.com, is constantly updated and provides access to all of the organization’s offerings. It has easy links for contacting legislators on pertinent issues. Government Affairs research and MGMA position papers on legislative issues are featured, as is information about products and services, upcoming conferences and leadership development seminars, specialty specific information pages, a member search feature to locate other members in your state or specialty, and many other offerings.
A final way to enhance the value of your membership is to give back in the form of volunteering. After many years on the MGMA AAA Executive Committee, today I reflect on all that I have learned and all of the new friendships I have developed—with other members and volunteers, vendors (like ABC, who has generously sponsored our keynote speaker for the last several years) who support our meetings and other ventures as well as making available to us their expertise, ASA leaders and staff, MGMA leaders and staff—and all the ways that I have been able to expand my horizons simply from devoting my time to a cause that is important to me and my profession. Life, truly is about continuous learning and taking advantage of all the benefits that are available to you. For anesthesiologists and anesthesiology administrators looking to excel in their professions, MGMA AAA offers a wealth of opportunity and is an invaluable resource, however you choose to participate.






 To answer this question, I go back to 1991 when I was not only new to anesthesia but also new to medical group practice administration. With a background in business and finance and no medical group experience whatsoever, I was recruited to the forward thinking group where I still work because they saw on the horizon that medicine was about to become more of a business. The 18-physician group had an office manager with lots of anesthesia billing experience but no business background. Anticipating the office manager’s retirement within a few years, they wanted to hire someone with a business background, figuring that the “medical group management” part could easily be learned. And what a learning experience it has been, and continues to be, thanks largely to MGMA AAA.
To answer this question, I go back to 1991 when I was not only new to anesthesia but also new to medical group practice administration. With a background in business and finance and no medical group experience whatsoever, I was recruited to the forward thinking group where I still work because they saw on the horizon that medicine was about to become more of a business. The 18-physician group had an office manager with lots of anesthesia billing experience but no business background. Anticipating the office manager’s retirement within a few years, they wanted to hire someone with a business background, figuring that the “medical group management” part could easily be learned. And what a learning experience it has been, and continues to be, thanks largely to MGMA AAA. Another significant development over the last several years is the addition of anesthesiology specific survey information. For years, MGMA has published the Physician Compensation and Production Survey, which reports anesthesiology-specific and pain management specific compensation data, and is a critical reference for many anesthesiologists as they negotiate support for non-compensated services with their facilities. In recent years, MGMA AAA has worked with the survey department to put together the Cost Survey for Anesthesiology and Pain Management in collaboration with ASA. That survey breaks down data in a number of ways (e.g. by staffing model) that are specific to anesthesiology and provides valuable statistics that cannot be found elsewhere, like revenue or units per anesthetizing location. In 2006, a pain management section was added and the 2009 survey will feature a section specifically for academic anesthesiology practices. More on this will appear in a future article when the surveys are getting ready to come out, but remember, if you want to obtain a free copy, you can do so simply by being a member and participating.
Another significant development over the last several years is the addition of anesthesiology specific survey information. For years, MGMA has published the Physician Compensation and Production Survey, which reports anesthesiology-specific and pain management specific compensation data, and is a critical reference for many anesthesiologists as they negotiate support for non-compensated services with their facilities. In recent years, MGMA AAA has worked with the survey department to put together the Cost Survey for Anesthesiology and Pain Management in collaboration with ASA. That survey breaks down data in a number of ways (e.g. by staffing model) that are specific to anesthesiology and provides valuable statistics that cannot be found elsewhere, like revenue or units per anesthetizing location. In 2006, a pain management section was added and the 2009 survey will feature a section specifically for academic anesthesiology practices. More on this will appear in a future article when the surveys are getting ready to come out, but remember, if you want to obtain a free copy, you can do so simply by being a member and participating.