eAlerts
-

THE FALL PERSPECTIVE
I hope that all of our loyal readers have had a nice summer. There is something about fall in Michigan that always takes me back to my college days. I love the cool, crisp weather and the beginning of a new football season. For many of my classmates Fall marked the end of the summer, but for me it ushered in the beginning of a new year of opportunity, the promise of interesting new discoveries, making new friends and, most of all, the satisfaction of gaining new insights and skills to make me more successful.
And so it is for ABC as well. Our staff has spent the summer settling into our newly renovated offices in downtown Jackson. Our purchase and restoration of the old Jacobsen’s department store building has proved to be an uplifting experience not only for our employees but for the community as a whole. You cannot help but feel good about an investment like this in a community like Jackson.
As the collection of articles in this issue of Communique clearly indicates, there is still much to learn about our ever-changing business and the specialty of anesthesia. Once again, we touch all the important bases, from the technical details of compliance and coding, to the legislative environment to the ongoing saga of anesthesia practice-hospital relations. Hopefully at least one of these thoughtful pieces will intrigue, fascinate, affirm or challenge you to look at your group or practice situation in a new way.
As many of you have already heard we have been especially fortunate this fall to have Karin Bierstein join our team. I think you will find her explanation for the transition quite intriguing. Not only do we consider her a tremendous asset and feel immensely grateful that she wanted to work with us, but we look forward enthusiastically to the insights and guidance she will give our people. We have always tried to be forward looking, to anticipate the next significant development and to make investments that anticipate our clients’ practice needs. I am thrilled that we can now do this at a whole new level.
Soon we will pack our bags to join many of you at the ASA annual meeting in San Francisco, the PGA in New York and the Practice Management Conference in Tampa which our very own Karin Bierstein planned with Committee Chair Robert Johnstone, M.D. Each hold a unique promise of new insight, increasing our professional network of resources and exploring aspects of practice management that we never realized were so critical to our survival and success. May we all find it a time of discovery, adventure and personal fulfillment.
I would like to personally thank you for your interest in our efforts on behalf of the specialty and your support for the various services we provide the community. As always, we welcome your comments and suggestions. With your input and Karin’s vision in addition to the publication management skills of Cortney Shepherd, these pages will soon take on a whole new look.
Sincerely,
Tony Mira,
President & CEO -
Compliance Corner: Get Ready for Increased Medicare Audit Activity As Recovery Audit Contractors Are Going Nationwide
Abby Pendleton, Esq. and Jessica L. Gustafson, Esq.
Wachler & AssociatesAs part of our desire to keep both clients and readers up to date, the Communiqué has been printing compliance information since its inception. In the Compliance Corner, we will now formally keep you abreast of the various compliance issues and/or pick out a topic that would be of interest to most of our readers.The financial pressure on hospitals, physicians and other healthcare providers, as a result of increased scrutiny of claims and audit activity by third party payors, will not end soon. To the contrary, as part of the Tax Relief and Health Care Act of 2006, Congress directed that the Medicare Recovery Audit Contractor (“RAC”) demonstration program expand to all 50 states by no later than 2010. CMS plans to aggressively move forward with this expansion. CMS has already announced the expansion of its program from three states to an additional nine states, with intentions for nationwide RAC auditing to take place by spring 2008, three-years ahead of schedule. Providers, including anesthesiology and pain management groups are well advised to prepare now for the expansion of the RACs and increasing Medicare audit activity.
RECOVERY AUDIT CONTRACTORS
The original three-year RAC pilot demonstration project was a result of Section 306 of the Medicare Modernization Act, which directed CMS to investigate Medicare claims payments using RACs to identify overpayments and underpayments. The pilot demonstration targeted the three states with the highest Medicare expenditures (New York, Florida and California), and has proven highly successful from the financial perspective of CMS and the RACs. The CMS RAC Status Document for FY 2006 reflects $303.5 million as total “improper” payments identified by the RACs for FY 2006, with a high percentage being linked to inpatient hospital claims.1The RAC process is designed to identify and recover overpayments (and underpayments) made by Medicare to providers. This process has ramifications that may significantly impact the financial status of providers. The current RAC experiences of many California hospitals highlights the significant impact the RACs will have on Medicare providers as the project goes nationwide. To date, providers have found the RAC process burdensome; significant resources have been dedicated to responding to volumes of record requests and defending claims denials.
Notably, CMS compensates RACs on a contingency fee basis, and RACs are entitled to keep their fee if a denial is upheld at the first level of Medicare appeal (i.e., redetermination to the Carrier or Fiscal Intermediary), regardless of whether the provider prevails at a later stage in the appeals process. Amazingly, subsequent appeals after the first level of appeal do not impact a RAC’s ability to retain the contingency payment. This fee arrangement appears troublesome, as it provides incentives to private companies to aggressively review and deny claims. This includes denying claims alleging that services were not medically necessary or appropriately documented, areas that contain much subjectivity and are often highly disputed by the provider. CMS’ payment agreement seems to guarantee that RACs will audit with a highly motivated work ethic to identify as many overpayments as possible.
Given what New York, Florida, and especially California providers are experiencing in the pilot RAC demonstration project, Medicare providers are well advised to begin the process of preparing for the RACs now. Although providers may not be able to stop RAC audits, providers can engage in activities that should assist with the process. For example, providers need to prepare by dedicating resources to:
- Internal monitoring protocols to better identify and monitor areas that may be subject to review;
- Responding to record requests;
- Compliance efforts including, but not limited to, documentation and coding education; and
- Dedicating personnel and resources to properly work up and defend denials in the appeals process.
MEDICARE APPEALS PROCESS
Claims denied as a result of a RAC audit are subject to the standard Medicare appeals process. Medicare providers should utilize the appeals process. In addition to substantive arguments, such as attacking claim denials on the merits, it is important for providers to understand that other legal arguments and strategies exist and can be utilized in the appeals process. These legal arguments and strategies may prove invaluable to the case. For example, the Social Security Act contains provisions, such as the Medicare Provider Without Fault and Waiver of Liability provisions, which can be used and developed with certain facts and circumstances that may exist in the case.In 2005, a new uniform Medicare appeals process was created resulting in the same appeals process for both Part A and Part B providers. This process includes:
- A redetermination appeal to the Carrier or Intermediary;
- A reconsideration submitted to a Qualified Independent Contractor (“QIC”);
- An appeal to an Administrative Law Judge (“ALJ”);
- An appeal to the Medicare Appeals Council (“MAC”); and
- An appeal to Federal district court.
In order to pursue the various levels of appeal, certain requirements must be met at certain stages in the appeals process. Although many providers have not seen much success at the redetermination stage of the appeal, the later stages of appeal, particularly the ALJ stage, may prove more successful. Providers must use due care in complying with the timeframes and other requirements set forth in the appeals process. Failure to do so may result in the inability to pursue the appeal.
The first level in the appeals process is redetermination. Providers must submit a redetermination request in writing within 120 calendar days of receiving notice of an initial determination. There is no amount in controversy requirement. Providers dissatisfied with a Carrier’s redetermination decision may file a request for reconsideration to be conducted by the QIC. This second level of appeal must be filed within 180 calendar days of receiving notice of the redetermination decision. As with the redetermination stage, there is no amount in controversy requirement. The QIC reconsideration stage of appeal has important ramifications for both Part A and Part B providers. With respect to Part B providers, the QIC reconsideration stage replaces the in-person Carrier Hearing that was afforded under the prior regulations. In an important negative change for Part B providers, the QIC reconsideration is an “on-the-record” review, rather than an in-person hearing. The previous process afforded Part B providers with an actual in-person hearing.
Moreover, it is important to note, as many providers may be unaware, that the reconsideration stage of the appeals process contains an early presentation of evidence requirement. This means that a provider’s failure to submit evidence to the QIC at the reconsideration stage of appeal will likely preclude the provider from introducing the evidence to an ALJ or later stages in the appeals process. Accordingly, it will be crucial for providers to fully work up their cases at the reconsideration stage of appeal.
The third level of appeal is the ALJ hearing. A provider dissatisfied with a reconsideration decision may request an ALJ hearing. The request must be filed within 60 days following receipt of the QIC’s decision and must meet the amount in controversy requirement. ALJ hearings can be conducted by video-teleconference (“VTC”), in-person, or by telephone. The final rule requires the hearing to be conducted by VTC if the technology is available; however, if VTC is unavailable, or in other extraordinary circumstances the ALJ may hold an in-person hearing. Additionally, the ALJ may offer a telephone hearing. Notably, the provider is not automatically entitled to an in-person hearing at the ALJ stage of appeal. The fourth level of appeal is the MAC Review. The MAC is within the Departmental Appeals Board of the U.S. Department of Health and Human Services. A MAC Review request must be filed within 60 days following receipt of the ALJ’s decision. Among other requirements, a request for MAC Review must identify and explain the parts of the ALJ action with which the provider disagrees. Unless the request is from an unrepresented beneficiary, the MAC will limit its review to the issues raised in the written request for review. The final step in the appeals process is judicial review in federal district court. A request for review in district court must be filed within 60 days of receipt of the MAC’s decision. In a federal district court action, the findings of fact by the Secretary of HHS are deemed conclusive if supported by substantial evidence.
SUMMARYCMS has announced its intention to aggressively expand the RAC pilot demonstration project, with plans for nationwide auditing to take place as early as spring 2008. The contingency payment arrangement between CMS and the RACs ensures that the RACs will aggressively audit providers, with an eye towards denying as many claims as possible. Providers are well advised to act now to prepare for the expansion of RAC activity. Providers should dedicate resources towards compliance education and towards timely addressing any document requests and/or claim denials. Because claim denials made by the RACs will be subject to the Medicare appeals regulations, providers must be cognizant of the appeal rules. 1 November 22, 2006, CMS RAC Status Document FY 2006, available at www.cms.hhs.gov (last accessed September 10, 2007).
-
The Three-Prong Changes To "Stark" That You Must Understand
By Mark F.Weiss, J.D.
Advisory Law GroupIf you have any concern about complying with Stark, the federal prohibition against self-referral, you need to understand the three-prong changes that have occurred since the beginning of July. Without this understanding, you will be unable to make an informed decision as to whether your activities conform to Stark’s requirement of absolute compliance.
Although Stark is a civil, not a criminal statute, if you have a financial relationship, as defined by Stark, in an entity to which you make Medicare or Medicaid referrals for “designated health services,” you must strictly fall within an exception in order to avoid substantial civil penalties and exclusion from Medicare and Medicaid program participation.
Complying with Stark is akin to trying to hit a moving target: Since the original statute’s enactment in 1989, the law has been amended multiple times and the Centers for Medicare and Medicaid Services’ process of issuing final regulations has spanned seven years, including four major regulatory pronouncements.
Even though it is difficult to argue that the government should not have a role in fighting fraud and abuse within federally funded healthcare programs, Stark’s tortured and esoterically complex legislative and regulatory scheme makes clear that the law’s authors, and the government employees charged with writing the interpretive regulations, have little understanding of business reality. They certainly have no appreciation of the impossibility of planning and executing complex business transactions in a regulatory environment is continually changing – what was legal under Stark yesterday is illegal today.
Three recent legislative and regulatory actions have increased this complexity.
PRONG ONE: PHYSICIAN FEE SCHEDULE PROPOSALS
This past July, the Centers for Medicare and Medicaid Services (“CMS”) issued its Proposed Revisions to Payment Policies Under the Physician Fee Schedule. Those revisions impact the Stark regulations, including:
- Suggestions of possible changes to the “same building” and “ centralized location” definitions pertaining to Stark exception.
- Suggestions that percentage based compensation deals would be considered to meet the “set in advance” requirement only in those circumstances in which they are based on revenue from services personally performed by the physician receiving the compensation.
- Proposed changes to the definition of an “entity” to include both the person or entity that presents the claim and the person or entity that either provides the designated health services or causes the claim to be presented. The impact of this would be to make illegal “under arrangements” services contracts between physicians and hospitals.
- Expanding the definition of ownership and investment interests to include a physician’s, or her family member’s, interest in a retirement plan, such that if the retirement plan has an interest in a DHS entity, the physician’s referrals to that entity would be prohibited unless subject to an exception.
- The requirement that the burden be on the entity submitting the claim to prove that the service was not furnished pursuant to a prohibited referral.
PRONG TWO: SCHIP LEGISLATION
In August, the United States House of Representatives passed the Children’s Health and Medicare Protection Act of 2007, commonly referred to in the press as the “SCHIP amendment legislation,” which includes language severely limiting Stark’s “whole hospital” exception.
As presently in effect (that is, unaffected by the proposed new law), there is an exception to the general Stark law prohibition on referrals by a physician to a hospital in which the physician has an ownership interest. This exception is referred to as the “whole hospital” exception as it permits an ownership interest in the whole facility, as opposed to an interest in merely a part of the facility. The House version of the Children’s Health and Medicare Protection Act of 2007 eliminates that exception. It grandfathers in hospitals with physician ownership that were in operation with Medicare provider agreements as of July 24, 2007, as long as they do not increase the number of beds or the number of operating rooms that were in existence on that date. However, it requires grandfathered hospitals to reduce physician ownership to an aggregate of no more than 40% of the facility and to no more than 2% individually within 18 months of enactment. It also mandates new disclosure of ownership rules as well as the disclosure to patients if the hospital fails to have 24 hour physician coverage.
The version of SCHIP amendment legislation passed by the Senate does not include this Stark law change. Although it is unknown in what final form the Act will emerge from conference committee or whether it will be signed into law, the prospect of loss of the whole hospital exception is already having a chilling effect on physician ownership of hospital deals.
If the Stark amendment language of the House version of the Act becomes law, the market for, and valuation of, hospitals will be affected greatly. Facilities which are owned largely, or entirely, by referring physicians will face particularly tough challenges: Divest to whom? Who must be cut from the investor roster entirely and who may remain? Stop participating in Medicare and Medicaid? Close? Cease any plans for expansion? Divestiture may create bargains in the hospital market; however, as physician ownership patterns change, so too will referral patterns, placing, in some instances, doubt on the continuation of historical operating margins and, therefore, on valuation.
PRONG THREE: PHASE III STARK REGULATIONS
On September 2007, CMS released its purportedly final phase, Phase III, of the Stark regulations. As it did with the proposed revisions to the Physician Fee Schedule, CMS used the Phase III regulations to further attack percentage based compensation.
CMS has a history of flip-flopping on this issue. Originally, CMS took the position that percentage compensation failed because it did not meet the “set in advance” requirement. Next, under pressure from the industry to recognize percentage payment as a common practice, CMS retreated from its former position, such that a percentage set in advance was seen as compensation that is set in advance. However, in the Phase III regulations, CMS reverses itself on the larger issue of percentage arrangements, taking the position that percentage compensation arrangements will often fail because they will not meet the additional requirement that compensation not take into account the volume or value of referrals.
In its Phase II final Stark regulations, issued in 2004, CMS created a safe harbor definition for fair market value of physician compensation that was based upon specific compensation survey data. CMS eliminates that safe harbor definition in the Phase III regulations.
CMS made clear in Phase III that for an independent contractor to qualify as a “ physician in the group practice,” the group’s contract must be with the individual physician or his professional corporation and not via a separate entity, such as another physician practice or a staffing company. Leased physician employees are not within the definition of physicians in the group practice. The Phase III regulations include clarifications by CMS that within group practices, productivity bonuses may be paid based on services that the physician has personally performed and/or services and supplies “incident to” such personally performed services. However, the allocation of profits within a group is subject to different rules, in that they must be allocated in a manner that does not relate directly to designated health services referrals, including those services which are billed “incident to.”
The regulations include new policy statements by CMS in connection with shared space and equipment. Specifically, physicians in more than one medical group may not simultaneously share space or equipment. A physician sharing a DHS facility in the same building must control the facility and the staffing at the time the that DHS is furnished to the patient. The practical effect is that block-leasing arrangements may be required. All shared facility arrangements must be carefully structured and operated in order to be compliant.
The definition of “indirect compensation arrangements” has been changed. A physician is deemed by the Phase III regulations to “stand in the shoes” of her group practice such that an arrangement between the group and an entity contracting with the group to provide DHS creates a direct compensation agreement with the physician. Previously, those sorts of relationships created “indirect” compensation relationships or perhaps no compensation relationship at all.
Phase III restates CMS’s position that when DHS is personally performed by the referring physician, there is no Stark law “referral.” However, CMS states in the preamble to Phase III that this position is not likely to apply to the provision of durable medical equipment, as there are few, if any, situations in which the referring physician is enrolled in Medicare as a DME supplier and personally performs all of the duties imposed on such suppliers.
CONCLUSION
The rules for Stark law compliance have changed and they will undoubtedly change again soon. The “finality” of the regulations is transitory. Existing referral relationships, in addition to new ones, must be tested for compliance with Stark’s ever changing requirements in order to avoid significant monetary penalties and exclusion from participation in Medicare and Medicaid.
Mark F. Weiss is a nationally recognized expert, and a frequent author and speaker, on the business and legal issues affecting physicians. He practices law with Advisory Law Group, A Professional Corporation, representing clients across the country from offices in Los Angeles and Santa Barbara, California. He is a Clinical Assistant Professor at USC’s Keck School of Medicine. Mr. Weiss offers our readers a series of complimentary educational materials. Mr. Weiss may be contacted via e-mail at markweiss@advisorylawgroup.com or via phone at 877-883-2803.
-
Coding Corner: Are You Reporting Pre-Operative Antibiotic Prophylaxis Under the Physician Quality Reporting Initiative (PQRI)?
Sharon Hughes
MBA, RHIA, CCSAT A GLANCEThe Tax Relief and Health Care Act of 2006 (TRHCA) Section 101 authorized,in Title I, the Physician Quality Reporting Initiative. This voluntary quality reporting program began on July 1st and ends on December 31, 2007. Unlike its predecessor, the Physician Voluntary Reporting Program (PVRP), the PQRI will pay physicians a bonus if they report the applicable quality measure(s) on at least 80% of the claims for eligible services performed during the second half of 2007. The only PQRI measure applicable to anesthesia care is #30, the timely preoperative administration of antibiotic prophylaxis.
Although groups seeking the bonus already have more than three months’ experience with the program, questions about the mechanics are still surfacing. A set of Frequently Asked Questions (FAQs)and answers furnished by members of the MGMA Anesthesia Administration Assembly (AAA) and by American Society of Anesthesiologists (ASA) staff recently appeared on the AAA list serv. These FAQs, as amended in October, appear below.Without additional legislation and funding it is not clear whether the PQRI will continue into 2008. Although Congress has failed to pass Medicare legislation thus far, it still has more than two months to do so. The Centers for Medicare and Medicaid Services (CMS) expects to be administering the PQRI or a similar program next year.
PQRI FAQS
The following answers to the Frequently Asked Questions were produced by MGMA and ASA staff in consultation with the Centers for Medicare and Medicaid Services (CMS) and are intended as an educational resource and reference guide only. They should not be considered legally binding or definitive statements of law. Differing answers may be warranted, based on varying facts and/or circumstances.
PQRI comments related to Perioperative Prophylactic Antibiotics:
Measure #20: is intended for the ordering physician and pertains to the surgeon.
Measure #30: is intended for the administering physician – typically an eligible professional providing anesthesia services – giving the prophylactic antibiotic at the correct time.
Eligible professionals include anesthesiologists, CRNAs and Anesthesiologist Assistants (AAs).
Question 1: Can both the Anesthesiologist and CRNA or AA receive credit if PQRI Measure #30 (antibiotic prophylactic timing) is submitted?
Answer 1: Any eligible professional with privileges to perform the clinical action described in Measure #30 can report CPT® II codes on the Medicare FFS claim. Therefore, both the anesthesiologist and the CRNA or AA may report Measure #30 (antibiotic prophylactic timing) if the actions described in the measure specification were performed for a given case. There is no medical direction issue or need to allocate the measure to one or the other of the clinicians.
Question 2: Can an Anesthesiologist and CRNA or AA report and get credit for delivery of prophylactic antibiotics if they are “hung” in the pre-op area and there is documentation that that they have been given pre-op as specified in PQRI Measure #30?
Answer 2: Yes, the anesthesiologist and CRNA or AA can report Measure #30 to indicate the prophylactic antibiotics were “hung” pre-operatively as long as there is a documented order and documentation of the timing of prophylactic antibiotic administration in the anesthesia record.
Question 2a: What about with a patient who comes down from the floor on antibiotics, so none are given prophylactically, how is this reported?
Answer 2a: In the scenario described above, there is no order for prophylactic antibiotics and the dosing schedule of the therapeutic antibiotics is unrelated to the procedure start or incision; therefore, Measure #30 would not apply to anesthesiology.
Question 3: PQRI Measure #30 “Timing of prophylactic antibiotics-administering physician” contains only two available numerators; 4048F-Given in timely manner and 4048F-8P-Not given in a timely manner. Modifier 1P is not listed with Measure #30. Can this modifier be used even if it is not listed on the measure for when a patient comes down from the floor already on an antibiotic?
Answer 3: No, there are no allowable performance exclusions for PQRI Measure #30 identified by the measure developer. Reportable numerator codes include 4048F or 4048F-8P as instructed in the measure specification.
Question 4: In a case with a deep abscess or wound infection, the surgeon states, “I do not want the prophylactic antibiotics to be given until after I obtain cultures from the wound” (i.e., after the incision has been made and the abscess has been located). May I report on PQRI Measure #30 using 4047F-8P and 4048F8P?
Answer 4: Since there was no order for prophylactic antibiotics to be administered prior to the surgical incision (or start of procedure when surgical incision is not required), Measure #30 does not apply. 4047F-8P is not a reportable code for measure #30.Question 5: Is the reporting of PQRI Measure #30 “Timing of Prophylactic Antibiotic-Administering Physician” only for surgical site prophylaxis or will SBE (Subacute Bacterial Endocarditis) Prophylaxis, when indicated, be included as well?
Answer 5: No, SBE prophylaxis is not included. The clinical recommendation statements and rationale refer to surgical wound infections which do not include SBE. See guidelines referenced for this measure in Measure #30 worksheet
Question 6: When reporting PQRI Measure #30 should we use the same diagnosis used when reporting the surgical procedure?
Answer 6: Yes, codes should be submitted via the CMS 1500 as part of your routine claims processing.
Question 7: How should one report PQRI codes on the claim form when Medicare is the secondary insurance? If the measure is applied to the primary insurance claim will it result in denials? Has CMS worked this out with other insurance carriers?
Answer 7: As referenced in FAQ #8467 on the CMS website: “Providers should not include the PQRI codes on claims submitted to primary payers (when Medicare is secondary) unless notified or approved to do so by that payer. Providers should, however, place the PQRI codes on the claim when submitting that claim to Medicare for secondary payment. When Medicare is primary there is an automatic cross-over of claims to payers who enter into agreements with CMS. Some payers may also elect to receive claims where Medicare is the secondary payer.”
Question 8: Should one report both the 4047F and 4048F for PQRI Measure #30 or does 4048F indicate an order was given?
Answer 8: Measure #30 requires you to submit both 4047F for the order and 4048F (with or without the 8P as indicated) for the administration of the prophylactic antibiotic. The denominator coding for Measure #30 includes 4047F (Documentation of order for prophylactic antibiotics) and the numerator coding includes 4048F with or without the 8P modifier (Documentation should note that prophylactic antibiotic was given within one hour (if fluoroquinolone or vancomycin, two hours) prior to surgical incision (or start of procedure when no incision is required).
Question 9: If 4047F has to be checked off by the anesthesiologist, must there be documentation that the surgeon ordered the prophylactic antibiotic for PQRI Measure #30?
Answer 9: Yes. For the purpose of reporting for PQRI, standing orders (clinical pathways and protocols) may be included; however, what is submitted on the claim should match the documented actions in the patient’s chart. Each physician or other eligible professional would need to refer to internal policies and standards from other governing bodies to determine whether the use of standing orders is permitted.
Question 10: How should reporting of the perioperative care measures be documented in the medical record? Should they be taken from the pre-operative nurse notes? Do they need to be noted in the anesthesiologist’s pre-operative evaluation and plan? Do they need to be on the anesthesia record?
Answer 10: Medical record documentation is required for all clinical actions described in a measure. Each eligible professional will need to determine the appropriate forms (paper or electronic) that require documentation (i.e. nurse’s notes, anesthesia record, etc.). The anesthesia provider should document the time the prophylactic antibiotic was initiated verifying the timing was appropriate for reporting the measure.
Question 10a: In the event that a pre-op or hospital RN administers the medication in the presence of an Anesthesiologist or CRNA, who should report the measure?
Answer 10a: Only eligible professionals can report PQRI Measure #30. However, if an Anesthesiologist or CRNA or AA is responsible for the administration of the prophylactic antibiotic, including observation of the pre-operative nurse administering the medication, they may report Measure #30. Note: The measure must be reported on the same claim as the procedure with which it is associated.
Question 11: Regarding PQRI Measure #30, does the time of administration of the antibiotic and the time of incision (or start of procedure if no incision) need to be documented together on the anesthesia record or other document?
Answer 11: Each physician or other eligible professional would need to refer to internal medical record documentation policy. For Measure #30, the timing, dosage, and route of administration of the prophylactic antibiotic must be documented in the medical record at the time of administration. Appropriate documentation may be more easily accessible for anesthesia providers if it were documented in one place, i.e. the anesthesia record. The incision time should be noted either in the anesthesia record or the operative record of the patient’s chart.
Question 11a: Does the type of antibiotic used, the time and signature have to be on the record?
Answer 11a: Yes, please refer to internal policies and standards from other governing bodies (i.e. JCAHO), which require this documentation.
Question 12: If a case is scheduled as an orthopedic “closed procedure/possible open procedure” how should this be handled for PQRI reporting purposes? The antibiotics may not be ordered until after the closed procedure is not successful and the open procedure is planned.
Answer 12: Note that prophylactic antibiotics may be given for planned open or closed procedures: “or start of procedure when no incision is required”. In this scenario, the antibiotics would be ordered to be given within 60 minutes of the incision and the relevant PQRI codes may be reported. It does not matter that the closed (non-eligible measure) intervenes between induction and incision.
Question 13: What should occur when a surgeon fails to write an antibiotic order, for a procedure or does not give the verbal order until the incision has been made? In this situation there would be no time to prepare and administer the prophylactic antibiotic “on time” because of this “late” order.
Answer 13: Late ordering of prophylactic antibiotic will result in performance failure for Measure #20. The surgeon responsible for the “late” order could report 4047F-8P (antibiotics were not ordered within one hour….) providing the surgical procedure performed was part of the denominator inclusion codes for the measure. The eligible professional providing anesthesia services would not be accountable to report Measure #30 since there was no documentation of the order for prophylactic antibiotics prior to the incision.Question 14: The patient is an inpatient and has been receiving regular scheduled doses of one or more therapeutic antibiotics. When the patient arrives in the operating room, the previous dose of antibiotics may not have been given within the “one hour prior to the incision” timeframe. How should the anesthesia provider report Measure #30?
Answer 14: In this scenario, the patient is receiving therapeutic, not prophylactic, antibiotics and the dosage schedule is unrelated to surgical incision or procedure start. Measure #30 is inapplicable unless an additional dose or additional antibiotic agent is ordered to be administered in the specified timeframe for wound prophylaxis. For more information please visit www.communiquenews.com.
For additional information please visit www.cms.hhs.gov.
-
The Medical Direction Team and Comparisons in Clinical Work Measures
Amr Abouleish, MD, MBA, Department of Anesthesiology, University of Texas Medical Branch
When an anesthesiology group is small and covers only one facility, the issue of “who is working hard” is moot. In a small setting, everyone can “see” everyone, and all the members take the same call and take the same time off. In contrast, as a group grows and begins to cover more than one facility, invariably there will be members of the group who think they do more work and should be paid more. In this situation, the group will need to reevaluate its compensation plans and how it measures “work done,” the majority being clinical work.
For clinical anesthesiology work, several categories of measurements can be used – all reflect the different types of compensation plans that exist in private-practice.i,ii Listed in order of prevalence, the systems used are based on (1) shift-worked (includes revenue split up equally), (2) charges or billed ASA units, (3) time billed,iii or (4) a combination. (I do not list “revenue-collected” since this is a measure of financial productivity, and not clinical productivity.)
Each of these categories values work slightly differently and devalues different types of work. Briefly, shift-worked values availability to work and assumes everyone’s daily caseload will even out in the end (since it gives no value to the actual charges billed). Charges or billed ASA units values actual charges but those billed units are dependent on OR scheduling, surgical duration, and type of surgery.ivTime billed values anesthesia time with a patient and not total time worked (since any turnover time and down time are non-billable). And finally, a combination represents a group’s attempt to minimize the downsides of each category.One factor that is essential to consider is the effect of anesthesia care team model on any comparisons of work done. When a group begins to consider measuring individual work, the group will invariably look at measuring work done “per doctor” or in business “per FTE” (where FTE = full-time equivalent). For a physician-only group, there is no problem with this methodology since the work done is done only by each member. On the other hand, once you introduce anesthesia care team model, then each doctor will be producing units billed in more than one room and the issue of staffing ratios becomes important to consider. It should be noted that this issue of staffing ratio is only important if billed units – either total ASA units/charges or time-billed – are used as the measurement of work.v
Since 2005, the MGMA has published an annual anesthesia survey entitled “Cost Survey for Anesthesia Practices.”vi In one of the breakdowns of the data, the data is presented by staffing models: physician only, 1 CRNA/AA per physician. The effect of staffing models is seen clearly when one looks at the data in these surveys. From the 2006 report, time and total units per case are almost identical among the three staffing models. (See Table) On the other hand, there is a marked differences between the models (especially between physician-only and >1 CRNA/AA per physician) when looking at time and total units billed per physician. This is not surprising since the medical direction groups bill more than one OR per physician while the physician-only group bills one OR per physician. On the other hand, when one takes the staffing model out of the equation, the work “per OR” shows fewer differences.
Within a group that covers more than one facility, differences in staffing models may confound comparisons of any measurements similar to the survey data. For instance, if a group covers a traditional inpatient facility and a newer ambulatory surgical center (ASC), the group may choose to cover the inpatient facility with 1:2 to 1:3 MD: CRNA ratio but 1:4 in the ASC. In this situation, billed units per FTE will favor the ASC due to the increased staffing ratio. Another example is the way some groups cover cardiac anesthesia cases with physicians only, and other cases with medical direction. In this situation, the differences in staffing models would confuse comparisons using “units per FTE”. In conclusion, measuring and comparing clinical productivity is difficult. It is not surprising that so many anesthesiology groups choose to split the money up evenly or only track shifts worked. If a group does choose to use units billed as a measure, staffing ratio differences should be reviewed. Even if the group does not use units billed for compensation, they may use them to track group productivity.viiNOTE: The Cost Survey for Anesthesia Practice is sent out every Spring, and the report is published in the late fall. The 2007 report has just been released. It is available at a discount for ASA members. Even better, every group completing the survey receives a copy of the final report free of charge. This article discusses only a small portion of the comprehensive survey.
i Abouleish AE et al. Measurement of individual clinical productivity in an academic anesthesiology department. Anesthesiology 2000;93: 1509-16
ii Blough GG, Scott SJ. Presentation of AAA survey on practice patterns at the ASA Practice Management Conference in San Antonio, Texas, on January 31-February 2, 2003
iii Feiner JR et al. Productivity versus availability as a measure of faculty clinical responsibility. Anesth Analg 2001;93:313-8
iv Abouleish AE et al. The effects of surgical case duration and type of surgery on hourly clinical productivity of anesthesiologists. Anesth Analg 2003;97:833-838
v Abouleish AE et al. Comparing clinical productivity of Anesthesiology groups. Anesthesiology 2002;97:608-616
vi Medical Group Management Association. Cost Survey for Anesthesia Practices: 2006 Report Based on 2005 Data. (Denver 2006)
vii Abouleish AE et al. Organizational Factors Affect Comparisons of Clinical Productivity of Academic Anesthesiology Departments. Anesth Analg 2003;96: 802-812

 As part of our desire to keep both clients and readers up to date, the Communiqué has been printing compliance information since its inception. In the Compliance Corner, we will now formally keep you abreast of the various compliance issues and/or pick out a topic that would be of interest to most of our readers.
As part of our desire to keep both clients and readers up to date, the Communiqué has been printing compliance information since its inception. In the Compliance Corner, we will now formally keep you abreast of the various compliance issues and/or pick out a topic that would be of interest to most of our readers. The original three-year RAC pilot demonstration project was a result of Section 306 of the Medicare Modernization Act, which directed CMS to investigate Medicare claims payments using RACs to identify overpayments and underpayments. The pilot demonstration targeted the three states with the highest Medicare expenditures (New York, Florida and California), and has proven highly successful from the financial perspective of CMS and the RACs. The CMS RAC Status Document for FY 2006 reflects $303.5 million as total “improper” payments identified by the RACs for FY 2006, with a high percentage being linked to inpatient hospital claims.1
The original three-year RAC pilot demonstration project was a result of Section 306 of the Medicare Modernization Act, which directed CMS to investigate Medicare claims payments using RACs to identify overpayments and underpayments. The pilot demonstration targeted the three states with the highest Medicare expenditures (New York, Florida and California), and has proven highly successful from the financial perspective of CMS and the RACs. The CMS RAC Status Document for FY 2006 reflects $303.5 million as total “improper” payments identified by the RACs for FY 2006, with a high percentage being linked to inpatient hospital claims.1 Claims denied as a result of a RAC audit are subject to the standard Medicare appeals process. Medicare providers should utilize the appeals process. In addition to substantive arguments, such as attacking claim denials on the merits, it is important for providers to understand that other legal arguments and strategies exist and can be utilized in the appeals process. These legal arguments and strategies may prove invaluable to the case. For example, the Social Security Act contains provisions, such as the Medicare Provider Without Fault and Waiver of Liability provisions, which can be used and developed with certain facts and circumstances that may exist in the case.
Claims denied as a result of a RAC audit are subject to the standard Medicare appeals process. Medicare providers should utilize the appeals process. In addition to substantive arguments, such as attacking claim denials on the merits, it is important for providers to understand that other legal arguments and strategies exist and can be utilized in the appeals process. These legal arguments and strategies may prove invaluable to the case. For example, the Social Security Act contains provisions, such as the Medicare Provider Without Fault and Waiver of Liability provisions, which can be used and developed with certain facts and circumstances that may exist in the case. SUMMARY
SUMMARY AT A GLANCE
AT A GLANCE Although groups seeking the bonus already have more than three months’ experience with the program, questions about the mechanics are still surfacing. A set of Frequently Asked Questions (FAQs)and answers furnished by members of the MGMA Anesthesia Administration Assembly (AAA) and by American Society of Anesthesiologists (ASA) staff recently appeared on the AAA list serv. These FAQs, as amended in October, appear below.
Although groups seeking the bonus already have more than three months’ experience with the program, questions about the mechanics are still surfacing. A set of Frequently Asked Questions (FAQs)and answers furnished by members of the MGMA Anesthesia Administration Assembly (AAA) and by American Society of Anesthesiologists (ASA) staff recently appeared on the AAA list serv. These FAQs, as amended in October, appear below. Answer 4: Since there was no order for prophylactic antibiotics to be administered prior to the surgical incision (or start of procedure when surgical incision is not required), Measure #30 does not apply. 4047F-8P is not a reportable code for measure #30.
Answer 4: Since there was no order for prophylactic antibiotics to be administered prior to the surgical incision (or start of procedure when surgical incision is not required), Measure #30 does not apply. 4047F-8P is not a reportable code for measure #30. Answer 13: Late ordering of prophylactic antibiotic will result in performance failure for Measure #20. The surgeon responsible for the “late” order could report 4047F-8P (antibiotics were not ordered within one hour….) providing the surgical procedure performed was part of the denominator inclusion codes for the measure. The eligible professional providing anesthesia services would not be accountable to report Measure #30 since there was no documentation of the order for prophylactic antibiotics prior to the incision.
Answer 13: Late ordering of prophylactic antibiotic will result in performance failure for Measure #20. The surgeon responsible for the “late” order could report 4047F-8P (antibiotics were not ordered within one hour….) providing the surgical procedure performed was part of the denominator inclusion codes for the measure. The eligible professional providing anesthesia services would not be accountable to report Measure #30 since there was no documentation of the order for prophylactic antibiotics prior to the incision. Each of these categories values work slightly differently and devalues different types of work. Briefly, shift-worked values availability to work and assumes everyone’s daily caseload will even out in the end (since it gives no value to the actual charges billed). Charges or billed ASA units values actual charges but those billed units are dependent on OR scheduling, surgical duration, and type of surgery.ivTime billed values anesthesia time with a patient and not total time worked (since any turnover time and down time are non-billable). And finally, a combination represents a group’s attempt to minimize the downsides of each category.
Each of these categories values work slightly differently and devalues different types of work. Briefly, shift-worked values availability to work and assumes everyone’s daily caseload will even out in the end (since it gives no value to the actual charges billed). Charges or billed ASA units values actual charges but those billed units are dependent on OR scheduling, surgical duration, and type of surgery.ivTime billed values anesthesia time with a patient and not total time worked (since any turnover time and down time are non-billable). And finally, a combination represents a group’s attempt to minimize the downsides of each category.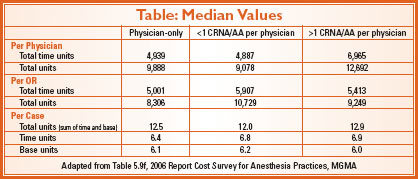 Within a group that covers more than one facility, differences in staffing models may confound comparisons of any measurements similar to the survey data. For instance, if a group covers a traditional inpatient facility and a newer ambulatory surgical center (ASC), the group may choose to cover the inpatient facility with 1:2 to 1:3 MD: CRNA ratio but 1:4 in the ASC. In this situation, billed units per FTE will favor the ASC due to the increased staffing ratio. Another example is the way some groups cover cardiac anesthesia cases with physicians only, and other cases with medical direction. In this situation, the differences in staffing models would confuse comparisons using “units per FTE”. In conclusion, measuring and comparing clinical productivity is difficult. It is not surprising that so many anesthesiology groups choose to split the money up evenly or only track shifts worked. If a group does choose to use units billed as a measure, staffing ratio differences should be reviewed. Even if the group does not use units billed for compensation, they may use them to track group productivity.vii
Within a group that covers more than one facility, differences in staffing models may confound comparisons of any measurements similar to the survey data. For instance, if a group covers a traditional inpatient facility and a newer ambulatory surgical center (ASC), the group may choose to cover the inpatient facility with 1:2 to 1:3 MD: CRNA ratio but 1:4 in the ASC. In this situation, billed units per FTE will favor the ASC due to the increased staffing ratio. Another example is the way some groups cover cardiac anesthesia cases with physicians only, and other cases with medical direction. In this situation, the differences in staffing models would confuse comparisons using “units per FTE”. In conclusion, measuring and comparing clinical productivity is difficult. It is not surprising that so many anesthesiology groups choose to split the money up evenly or only track shifts worked. If a group does choose to use units billed as a measure, staffing ratio differences should be reviewed. Even if the group does not use units billed for compensation, they may use them to track group productivity.vii