More Ingredients for your Alphabet Soup
Christine Sikora, CHM
Practice Administrator, Hartford Anesthesiology Associates, Inc., Hartford, CT
All of you are familiar with some of the regulatory requirements that affect your practice, as identified by their acronyms and initials: HIPAA, CMS, CoPs,PQRS, SCIP, ACO, HCAHPS. For hospital-based practices, there are now two additional “ingredients” in our regulatory alphabet soup that will require your attention: OPPE and FPPE.
 Historically, hospital medical staff appointments and reappointments have been primarily a subjective process, where the clinical chief signed off on credential/privilege requests, perceived competencies and specific skills.
Historically, hospital medical staff appointments and reappointments have been primarily a subjective process, where the clinical chief signed off on credential/privilege requests, perceived competencies and specific skills.
The Joint Commission and other accrediting bodies and payers have established more stringent guidelines for the ongoing evaluation of medical staff members. The Ongoing Professional Practice Evaluation (OPPE) and Focused Professional Practice Evaluation (FPPE) are now becoming part of every hospitalbased anesthesia practice’s routine. These evaluations are expected to occur on a regular basis and serve as the key component to the hospital reappointment process.
Key Components
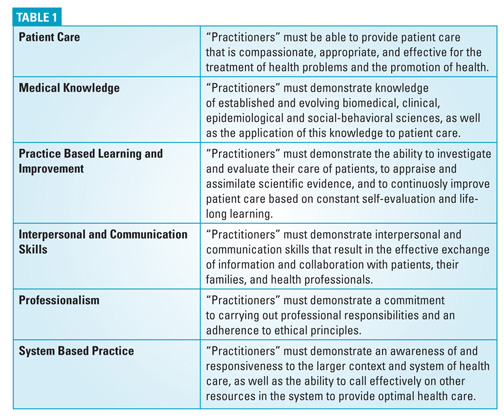
In adopting the Accreditation Council for Graduate Medical Education’s (ACGME) established competencies, www.acgme.org, the Joint Commission requires the following components as part of the OPPE/FPPE process (See Table 1)
A Systematic Approach to Your OPPE Program
 Advice for this alphabetic avalanche: don’t panic! There is a systematic approach that you can take to develop your OPPE program. Start by considering all the elements that are part of your daily clinical practice. Do you have practice management software that tracks provider certifications, licensure, privileges and CMEs? Do you have an AIS (anesthesia information system), interfaced to a hospital EMR and further interfaced to your billing application? Do you have an event reporting application, submit to the Anesthesia Quality Institute (AQI), or track your own adverse events for quality indicators and CORE/SCIP measures JCAH SCIP?
Advice for this alphabetic avalanche: don’t panic! There is a systematic approach that you can take to develop your OPPE program. Start by considering all the elements that are part of your daily clinical practice. Do you have practice management software that tracks provider certifications, licensure, privileges and CMEs? Do you have an AIS (anesthesia information system), interfaced to a hospital EMR and further interfaced to your billing application? Do you have an event reporting application, submit to the Anesthesia Quality Institute (AQI), or track your own adverse events for quality indicators and CORE/SCIP measures JCAH SCIP?
Once you have a list of these elements, continue to think of all the regulatory and required training that you might have to complete for the hospital. Such things as mandatory fire safety training, Malignant Hyperthermia drills, and risk management education sessions can fulfill components in your OPPE process.
Next, focus on clinical and billing documentation requirements. All of your qualified anesthesia providers must follow the CMS Anesthesia Conditions of Participation (CoPs). If you conduct clinical and/or billing documentation audits focusing on any of the anesthesia CoPs, audit results can be part of your OPPE program. Another hint: if your hospital conducts medical record audits for such things as non-approved medical abbreviations, missing signatures, and informed consent completion, request this information for your anesthesia providers and include it in your OPPE.
As we progress in the new era of healthcare, value-based purchasing indicators and HCAHPS scores are other ingredients that can really make your anesthesia OPPE program effective, and demonstrate your practice value to the hospital administration.
An OPPE Tool
 The goal of an effective OPPE program is more objective, relying on data elements, rates, goals and thresholds. Gone are the days of the total subjective evaluation. This is a very critical point that should be used to secure your physician’s participation in the overall OPPE process. If they can manage their own performance, they are more likely to be accountable. If they are more accountable, the quality of their patient care improves.
The goal of an effective OPPE program is more objective, relying on data elements, rates, goals and thresholds. Gone are the days of the total subjective evaluation. This is a very critical point that should be used to secure your physician’s participation in the overall OPPE process. If they can manage their own performance, they are more likely to be accountable. If they are more accountable, the quality of their patient care improves.
Figure 1 is an example of a physician OPPE tool that incorporates the required ACGME components and applicable anesthesia practice elements. You will see that we’ve kept three components as a subjective evaluation.

FPPE Process
Once you have your OPPE framework, the same process applies to conducting a more focused evaluation, or FPPE. An FPPE is usually completed when there is a concern about a currently privileged practitioner’s ability to provide safe, high quality patient care. It may be triggered through a peer review process, complaint, or ongoing professional practice review or for the evaluation of privilege-specific competence for all new medical staff members (including allied or adjunct staff) and for new privielges granted to members of the Medical Staff. For the FPPE, you may have specific information that would yield a “less than average” or “poor” result for one of the subjective elements, thereby requiring documentation, counseling, and/or corrective action.
“Killing two birds with one stone”
Your OPPE/FPPE template that you develop can also serve a dual process. You can adjust the template, as needed, adding in either subjective or other more objective competency evaluations, or attendance records, and utilize as part of your annual physician, CRNA, and AA internal evaluation process.
In summary, the elements for an effective OPPE program are already part of your daily clinical and operational practice management. By developing a list of your available data elements, you will be able to match them to the required OPPE components. Then develop a form that matches your data elements to the requierd OPPE components. Not only will you be able to manage the alphabet soup of rules and regulations, you will also be able to better demonstrate the value of your anesthesia practice to hospital administration.
Christine Sikora, CHM is the Practice Administrator with Hartford Anesthesiology Associates, Inc., (HAA), in  Hartford, CT, since 1998. Working with this 85 member physician anesthesia practice, Ms. Sikora focuses on corporate as well as daily operational responsibilities that include regulatory compliance and auditing, QAPI Program and staff privileging and credentialing. Contact her at (860)-545-2033 or csikora@harthosp.org.
Hartford, CT, since 1998. Working with this 85 member physician anesthesia practice, Ms. Sikora focuses on corporate as well as daily operational responsibilities that include regulatory compliance and auditing, QAPI Program and staff privileging and credentialing. Contact her at (860)-545-2033 or csikora@harthosp.org.