Anesthesia's Role in Developing Effective OR Governance
Jerry Ippolito, BA, MHSA
Director, Perioperative Services Business Development, Southeast Anesthesiology Consultants, PA, Charlotte, North Carolina
A lot is written in the literature these days and there is ongoing debate in both the anesthesiology and OR-management communities with regard to who should be running the OR - Nursing Directors or Medical Directors of Anesthesiology. At the ASA’s recent conference on Practice Management one speaker referred to anesthesiology groups as ”Super Groups” and ”Orphan Groups.” In summary, the “Orphan Groups” continue to wring their hands, point fingers, and position themselves as “victims” — “Super Groups”, on the other hand, position themselves as “Champions of Program Excellence” partnering with their hospital / ASC customers in fostering quality, efficiencies and business growth. First and foremost, if anesthesiology wants to be respected as a leader in program governance, it must position itself as a “Super Group.”
 Simply stated, anesthesiology needs to be proactively involved in OR operations and planning with specific emphasis on schedule planning and administration. If not involved in schedule planning and administration, then anesthesia can only react to the decisions of others. When in a reactive vs. proactive mode, customer service can not be optimized. Who runs the OR (or best stated the perioperative services program) is a far more complex set of circumstances. The correct question is: ”What does Effective Perioperative Services Program Governance Look Like?”
Simply stated, anesthesiology needs to be proactively involved in OR operations and planning with specific emphasis on schedule planning and administration. If not involved in schedule planning and administration, then anesthesia can only react to the decisions of others. When in a reactive vs. proactive mode, customer service can not be optimized. Who runs the OR (or best stated the perioperative services program) is a far more complex set of circumstances. The correct question is: ”What does Effective Perioperative Services Program Governance Look Like?”
When anesthesia does not take a proactive role in fostering and enforcing effective governance, then anesthesia will remain in a reactive mode and will not be able to optimize satisfaction levels of its customers (surgeons, administration, nursing and last but not least the patient). Too frequently we hear of anesthesia being referred to by nursing and administration as “A Necessary Evil” – ”Orphan Group.” In my experiences anesthesia typically has a sound grasp on what is necessary to run an efficient and marketable OR program. Maintaining program efficiencies and garnering new business is even more important to anesthesia than to the hospital as an anesthesia group does not have the same level of financial reserves as a hospital. Unfortunately, however, rather that being a “Champion” for program reform by promoting program development, anesthesia typically points fingers at administration and nursing. Due to the perception of anesthesia being a “necessary evil” or “having an agenda of its own”, regardless of how sound recommendations may be, nursing and administration seldom listen to anesthesia.
Running the OR and fostering development of effective governance are two different issues. I was recently interviewed by the publication OR Manager and asked whether anesthesia or nursing should run the OR and my response was that if effective governance is in place, then it does not matter which constituency of the four-legged stool (anesthesia, nursing, surgeons or administration) runs the OR on a daily basis. [ABC addressed the same question in our March 13, 2009 Alert. We are grateful to Mr. Ippolito for providing much of the background material for our Alert entitled “Should Anesthesia Run the OR?” There we identified the many assets of anesthesiologists, who have a long and successful history of managing the OR - success being contingent, of course, on the requisite leadership and organizational skills as well as the knowledge of the anesthesiologist. If you would like a copy, or if you would like to be on the e-mail distribution list for the Monday Alerts, please contact cortney.shepherd@anesthesiallc.com. -Ed.]
Running the OR is the implementation, execution, and enforcement of the policies and procedures developed by the governance body. Some feel that anesthesia should run the OR because in order to maintain an effective OR program physicians must be positioned to police physicians. Others feel anesthesia should run the OR as OR Directors come and go from institutions and anesthesia is generally a more stable entity. Lastly, there is a school of thought that anesthesia should run the OR because anesthesia is “ever-present” in the OR. I don’t totally disagree with any of this thinking but must indicate that making anesthesia the “policeman” of the OR without holding other constituencies accountable will only result in fostering the reputation of that “necessary evil.” About eight years ago I was engaged by a major mid-Atlantic university hospital to assist in improving operating room efficiencies. To this day I use this case study as an example of what happens when effective governance is lacking. In this instance the Chairman of the Department of Anesthesia was sponsoring the engagement for the hospital. The anesthesia chair had been directed by the Dean of the university and hospital CEO to “fix the OR.” The OR was totally dysfunctional; surgeons did whatever they wanted, whenever they wanted; the environment was total chaos. The Chair continues to be a highly regarded individual and has a sound grasp of what is required to maintain an effective OR program. The Chair proposed sound strategies for change and promoted sound policies and procedures. Needless to say the Chair remained very frustrated as progress was not being made and it was alleged to be the fault of anesthesia. Progress was not being made as only one constituency of the four legged stool was being held accountable – only anesthesia was being held accountable. I was simultaneously engaged at a university on the opposite side of the city where effective governance was developed and each of the constituencies was held accountable. Anesthesia championed the process through its “ever-presence in the OR” and tremendous progress was made.
Generally when there is a lack of effective governance silos develop among the four constituencies and it is difficult to have effective program management and optimized satisfaction levels among the constituency members. Indeed each of the constituencies does have an agenda so to speak.
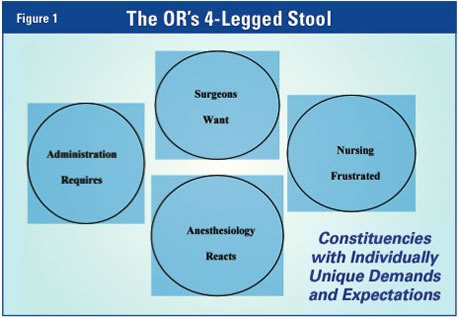
The OR’s 4-Legged Stool
Typically in siloed environments constituency members maintain an expectation that their wants and needs will be fulfilled by others, to a 100 percent level, 100 percent of the time. In this environment constituent members do not take accountability for their actions and are unwilling to police themselves much less each other (See Figure 1). The Director of Surgical Services and anesthesia remain in a “NO-WIN” situation until both anesthesiologists and surgeons recognize that they must be accountable for their actions, be responsible for development of solutions, not maintain expectations that their needs will be fulfilled by others, be champions of program change and prosperity as opposed to complainers.
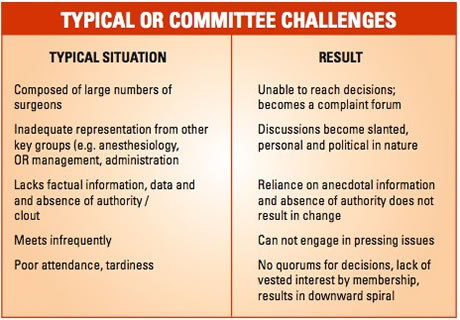
Effective surgical program governance is best achieved by considering the OR as a business corporation. The OR is the “Financial Engine of a Hospital” and should be governed as such. Corporations have boards of directors and CEOs. CEOs do not make unilateral decisions; CEOs brief boards of ongoing situation, changes in the environment, provide data and information, guide decision making after having analyzed facts and circumstances. Boards develop strategic and tactical plans and develop policies and procedures. CEOs and management teams implement and enforce decisions of the board. In this regard, what we typically refer to as the hospital’s OR Committee acts as the board; the Director of Surgical Services in partnership with anesthesia acts as the CEO. To this point you may say to yourself, “Our hospital has an OR Committee, but the OR is still dysfunctional and chaotic. In my experiences most hospitals’ OR Committees are dysfunctional, lack value and clout for reasons as follows.
Generally the OR Committee lacks clout because it has not been formally charged by the hospital’s CEO as an empowered hospital operations committee (as to differ from the Department of Surgery which is a medical staff body). Similarly, if the CEO does not bestow formal authority on the OR Committee and support Committee decisions, disgruntled individuals (usually surgeons) make “end-runs” to the hospital’s CEO around the Committee. In these instances the CEO typically intercedes, makes decisions based on the anecdotal evidence provided by the disgruntled party and undermines the Committee’s authority and effectiveness. Committee members lose interest and are unwilling to invest their personal time; a negative spiral develops.
The foundation of effective surgical services program governance is based on the composition, authority, mission, charge and enforcement of the OR Committee. The foundation of effective OR governance is that where a culture is developed and programs are developed and governed by that culture and not one or several individuals. Some key elements of an effective OR Committee follow:
- Maintains a charge of fostering development of and maintaining a quality oriented, effective, efficient and marketable surgical services program through the development and enforcement of effective policies and procedures.
- Is charged and supported by the hospital’s board and CEO as a hospital operations committee; decisions of the Committee are not to be overruled by hospital administration, the Board or departments of the medical staff. The OR Committee is not subordinate to, nor needs approval of, medical staff bodies (e.g. Department of Surgery or medical staff as a whole).
- Maintains a philosophy that the OR is a shared and common work place, is no one person’s or constituency’s domain, is a place where compromise and consensus is paramount.
- Maintains a manageable size – typically of 11 to thirteen members.
- Maintains representation of key and high volume surgical specialties. Assures that physician committee members (particularly surgeons) have a vested interest in the hospital and are personally affected by Committee decisions:

- operate frequently at the hospital and use the hospital as their primary place of surgery;
- have an interest in developing their practices;
- have a willingness to foster program change and success for the greater group;
- have a willingness to enforce policies and procedures and a willingness to approach their colleagues;
- chiefs of service who do not have the referenced characteristics should not be on the OR Committee
- have an ability and willingness to enforce policies and procedures against physician friends and business associates
- Committee members should be effective formal and informal leaders.
- Maintain representation of anesthesiology by an anesthesiologist with good interpersonal, communicative, organizational and data interpretation skills; an anesthesiologist who takes a lead role in the planning and administration of the schedule on a daily basis (this may not necessarily be the chief of anesthesiology).
- Include representation of OR management (Director of Surgical Service, OR Manager) and administration (VP over surgery, CNO, but not CEO).
- Meet on a monthly basis and have a planned agenda.
- Be guided by data and factual information presented by the Director of Surgical Services in partnership with anesthesiology.
- Charge the Director of Surgical Services and anesthesia to implement and enforce policies and procedures developed by the OR Committee.
Where this structure is developed anesthesia is positioned to assist in championing program development and success but is not regarded as a “policeman or necessary evil.” Where this structure is developed each of the schools of thought referenced earlier in this article as to why anesthesia should run the OR is addressed and applied, but in a formal and organized manner:
- Anesthesia participates in enforcing policies and procedures among anesthesiologists and surgeons (physician to physician communication);
- Anesthesia maintains the ever-presence in the OR;
- Directors of Surgical Services come and go, but a “culture” sustains program success; and
- Regardless of which constituency is the “organizational leader” nurses continue to be evaluated by nurses in terms of clinical competencies.
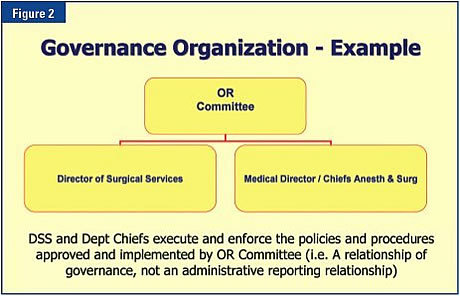
Where this governance structure is developed, it does not matter whether anesthesia or nursing runs the OR. Neither does. In partnership the two implement policies and procedures developed by a higher authority; nursing and anesthesia guide the higher authority in decision making. (See Figure 2.)
Additional articles by Jerry Ippolito and complimentary learning tools can be downloaded from www.ORefficiencies.com.
Jerry Ippolito, BA, MHSA Director, Perioperative Services Business Development, Southeast Anesthesiology Consultants, PA, Charlotte, North Carolina