Assessing Operating Room Efficiency
Jody Locke
Vice President of Anesthesia and Pain Management Services, ABC
The measurement of operating room efficiency used to be one of those arcane sciences reserved for a special breed of consultant with experience in balancing the political and practical requirements of the daily management of a suite of operating rooms, but not any more. Given the impact of inefficient operating room management on anesthesia coverage and call requirements, O.R. utilization is rapidly becoming a key factor in an anesthesia practice’s need for financial support. While the causes of inefficient operating room utilization tend to be complex and directly related to a hospital’s need to compete for surgeon allegiance in increasingly competitive markets, it is not uncommon for anesthesiologists to be invited to join the fray. The concept of an anesthesiologist or an anesthesia department designee playing some role in O.R. management is not new. Many practices have had a “floor person,” “Clinical Day Director,” or “Captain of the Ship” for years. Typically, these have been ombudsmen providing a customer service rather than aggressive managers empowered to actively modify surgeon behavior. The problem is simply that for all their experience in the arena, most anesthesiologists have yet to develop the necessary tools and strategies to make them effective agents of change.
From an anesthesia perspective all discussions of operating efficiency ultimately hinge on the economics of coverage and call. This takes some overeager practitioners right to a discussion of profitability. From a management perspective, however, an exploration of benchmarks and metrics may be more useful in the strategic positioning of anesthesia as a contributor to the solution of declining productivity. Establishing a common vocabulary of performance utilization is deceptively complex. It is not uncommon to hospital administrations to view any data from the anesthesia practice with a healthy dose of skepticism. As in so many exercises in change, management time must be spent educating all the stakeholders so that they agree on the problem, accept the metrics and share some ownership for the process.

Most observers would agree all metrics should be viewed and tabulated by anesthetizing location. Let us further assume,for the sake of this discussion,that an anesthetizing location is an actual or virtual location that requires dedicated anesthesia personnel for part or all of a 24 hour period. By this definition each operating room is an anesthetizing location, as is the delivery suite, the Cystoscopy room, or any other physical space where anesthesia services might be required. The definition becomes a little less clear when the dedicated personnel are required to provide a variety of non-operating room services. Each practice must work through its own definition of N.O.R.A. (Non-Operating Room Anesthesia) requirements.
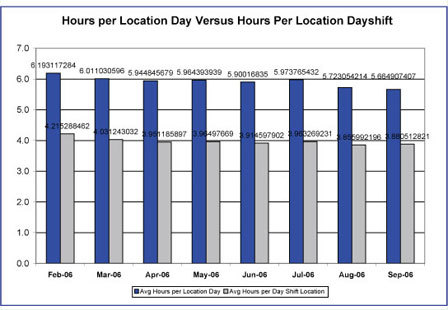
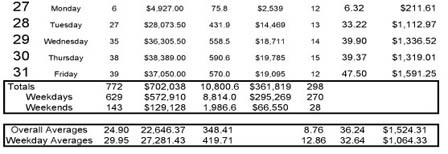
One school views operating room efficiency through the absolute lens of a particular metric such as cases, units or minutes per anesthetizing location day. There is considerable discussion across the country as to appropriate points of reference. There is some data to support an optimal number of cases per location day, but as even the most casual observer of the specialty will note not all cases are of equal acuity or duration. Others prefer to focus on total ASA units billed per location per day (base, time, modifier and incidental units) and will site the magic number 50 as an ideal productivity benchmark. Still others prefer to measure and monitor minutes. Actual anesthesia time has the advantage of corresponding, more or less, to the operating room time captured by the hospital staff. Discussions of anesthesia time can take a number of directions depending upon how important it is to identify when activity occurs. It has been suggested that an operating room that generates 6 hours of anesthesia time between 7 AM and 3 PM is running at optimum efficiency. Obviously, all benchmarks and standards must be adjusted to meet the particular requirements and challenges of the facility.
Proponents of such metrics argue that while they may not be a perfect measurement of every situation at least they provide a consistent frame of reference. They lend themselves to an objective comparison of facilities. An operating room that consistently generates 40 ASA units per location day is clearly less efficient than one that generates 50 or more units.
Inevitably, the question arises: Which metric is best? “Best” is a relative term because all valid data has some value if it is applied judiciously. A determination of the most appropriate metric or approach for a particular setting should hinge on two separate issues: reliability and credibility. Many anesthesiologists put great stock in measuring total ASA units per location day, because they know how they get paid for anesthesia, but such an approach may be viewed with great suspicion by hospital administrators who do not understand how anesthesia basic values and time units are determined. In other words, if a particular metric does not serve the goal of providing common coinage for a discussion of management options it will serve no practical purpose.
Another school of thought is more concerned with the relationship between coverage commitments and actual production patterns. In this variation on the theme actual hours of anesthesia time are divided by total hours of staff coverage. Such an approach factors in such issues as call and distinctions between short and long rooms. The advantage of such a perspective is that it can be customized to any particular configuration of anesthetizing locations. The disadvantage is that all applications become relative.
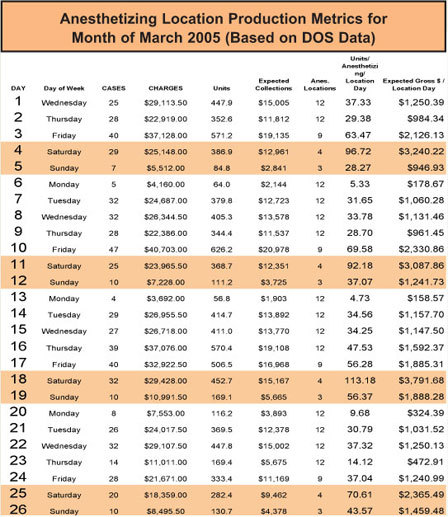
Included below are examples of each of the two approaches to the measuring of operating room productivity. Not every anesthesia practice will want to develop the tools to generate such reports, although more practices should probably be exploring the possibilities than are currently doing so because too often it is the initiation of a serious subsidy discussion that triggers the need to look at productivity. Practices that have been monitoring O.R. metrics over time have much greater conversance with their applicability and relevance. The fact is that as is true of the administration of anesthesia, it is difficult to manage what one does not measure. While anesthesia practices have traditionally focused on the measurement and management of billings and collections, more and more are beginning to realize that the one piece of the equation they did not choose to monitor is the one that has the greatest impact on the income and lifestyle of the members.
It has been said that you cannot manage what you do not measure. Anesthesiologists know this intuitively, because the availability of reliable physiologic data about a patient’s response to the trauma of surgery and anesthesia plays such a critical role in the consistent outcomes of today’s practitioners. The converse is also true: what you do not measure, you cannot manage. Anecdotal discussions tend not to support serious change. If O.R. productivity is an issue for your practice then an investment in the tools and resources to capture the data and monitor it closely is a small price to pay for the opportunity to be part of the solution rather than a victim of the problem.