April 1, 2013
To avoid the 2015 PQRS and 2015 Value Based Payment Modifier (VBM) penalties, ABC recommends that all large group anesthesia practices (groups with 100 or more eligible professionals (EPs)) complete the group practice self-nomination process and elect the administrative claims reporting option, without quality tiering, by October 15, 2013.
In last week’s Alert, we summarized the requirements for participating in Medicare’s Physician Quality Reporting System (PQRS) in 2013. One of the major changes to the PQRS program—which we deferred until this week—is the implementation of the Value-Based Payment Modifier (VBM) for groups of 100 or more eligible professionals (EPs), consisting of physicians and CRNAs and others described in detail below.
Groups of 100 or more EPs — Watch out for the Value-Based Payment Modifier
The Patient Protection and Affordable Care Act (ACA) requires that Medicare implement a Value-Based Payment Modifier (VBM) that would apply to Medicare fee-for-service payments beginning in 2015. The VBM is intended to pay physicians differentially based on the quality and cost of their care.
While CMS must adhere to certain statutory requirements, such as using the modifier to promote shared responsibility and systems-based care, the ACA gives CMS considerable flexibility in terms of implementing the VBM. The 2013 Medicare Physician Fee Schedule (MPFS) rule, which lays out the rules for the initial roll out of this program, demonstrates CMS' commitment to easing physician burden, promoting alignment across federal quality reporting programs and offering greater choice of measures and reporting mechanisms, ensuring a fair and gradual application of the VBM.
Below is a summary of CMS' initial implementation plan, including the populations that CMS will first target, as well as the measures and methodologies it will employ to calculate the value-based payment modifier.

Groups with 100 or More Eligible Professionals (EPs)
As mentioned, CMS is only required under statute to apply the VBM to select physician populations in 2015 and has the discretion to determine the makeup of this initial target. For 2015, CMS will initially apply the modifier to groups with 100 or more eligible professionals (EPs). "Group" refers to all EPs practicing under the same Tax ID Number (TIN).
For purposes of identifying group practices, CMS will define "eligible professionals" as not only physicians, but physician assistants, nurse practitioners, clinical nurse specialists, certified registered nurse anesthetists, anesthesiologist assistants, certified nurse-midwives, clinical social workers, clinical psychologists, registered dietitians/nutrition professionals, physical and occupational therapists, qualified speech-language pathologists, and qualified audiologists. CMS chose this broader definition since it aligns with the PQRS. Since this definition is not limited only to physicians, smaller practices that rely heavily on ancillary staff will want to verify whether they fall under this initial target. Group practices with 2-99 EPs will remain unaffected during the first year.
Although group practices will be defined broadly, the payment modifier itself will apply only to items and services billed by physicians under a single tax-identification number (TIN). CMS will identify groups of physicians subject to the VBM based on a query of Medicare's Provider Enrollment, Chain, and Ownership System (PECOS) on October 15, 2013. CMS will remove any groups from this list if, based on a claims analysis, the group of physicians did not have 100 or more eligible professionals that submitted claims during the performance period.
How to Avoid the Value-Based Modifier Penalty for 2013 in Three Easy Steps
To avoid the penalty under the VBM in 2015, group practices of 100 or more eligible professionals should follow the three easy steps outlined below.
- PECOS
Since CMS will gather information such as a physician’s specialty and group practice affiliation from PECOS for both the Physician Feedback Reports and the VBM, it is important that you make sure your practice data is up-to-date by visiting PECOS Medicare Enrollment website. - Self-Nominate for PQRS
Groups of 100 or more EPs have to self-nominate to participate in one of the PQRS Group Practice Reporting Options (GPROs) by October 15, 2013 via the CMS Communications and Support website. - Successfully Report PQRS
- Satisfy the reporting criteria for the 2013 PQRS incentive via either the GPRO registry reporting option or the GPRO Web Interface;
– OR – - Elect to be analyzed under the PQRS administrative claims-based reporting option by October 15, 2013.
ABC recommends that all large group anesthesia practices complete the group practice self-nomination process and elect the administrative claims reporting option by October 15, 2013 to avoid the 2015 PQRS and 2015 VBM penalties. (NOTE: CMS has not yet opened the self-nomination process to providers, we anticipate the website will be available early this summer.) This also will allow members of your group to continue to report the traditional claims-based measures as individuals in order to earn the PQRS incentive in 2014 based on the 2013 reporting period. The administrative claims option means that CMS will review your practice’s claims and abstract certain quality metrics. Please see the interaction between the PQRS and the VBM in Figure 1 below.

Budget Neutral Quality Tiering
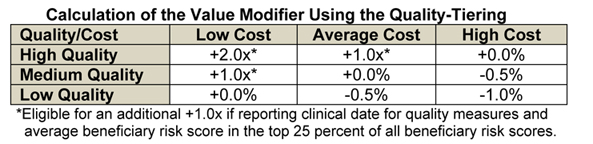
Quality tiering is an optional aspect of the 2015 VBM that rewards or penalizes a group based on quality data (based on a composite of the group's PQRS reporting mechanism and a set of care coordination measures) and cost (based on a composite of total per capita measures). In order to achieve the legislatively-mandated budget neutrality for the program, positive adjustments to groups of physicians would be offset by negative adjustments to other groups of physicians. CMS will divide the total quality and cost composite scores for each group practice into three tiers based on whether the score is above, not different from, or below the national mean. Since the total sum of downward adjustments is unknown at this time, CMS cannot determine specific upward payment amount percentages. As shown in the table below, CMS will give groups that are high quality and low cost the highest upward adjustment. The value of the upward payment adjustment factor ("x") will depend on the total sum of negative adjustments in a given year. In addition, to ensure that the VBM encourages physicians to care for the severely ill and beneficiaries with complicated cases, CMS will apply an additional upward payment adjustment for groups furnishing services to high risk beneficiaries. ABC also recommends that groups do not elect the quality tiering option for 2015. The program is still not completely fleshed out and more information will be needed before any recommendation could be made for anesthesiologist to participate.
It is no secret that the administrative claims option requires much less effort on the part of the group practice. In an effort to promote gradual implementation of the VBM, CMS also will not automatically consider group practice performance on quality measures when determining application of the modifier during this initial stage. Therefore, to avoid an adjustment under the VBM in 2015, group practices must simply demonstrate an attempt to engage in quality measure reporting in 2013. Group practices will only be held accountable for quality and cost performance if they voluntarily opt for the quality-tiering approach. However, as previously stated, ABC recommends that groups do not elect the quality tiering option in 2013 for the 2015 modifier, because more information will be needed before any recommendation could be made for anesthesiologists.
Despite the fact that payments under the PQRS and the initial year of the VBM are still largely based only a group practices' ability to report measures, physicians should not ignore their performance scores. CMS already expressed its desire to, in the very near future, base the modifier on performance and this decision will likely not remain optional. CMS also anticipates proposing to increase the amount of payment at risk under the modifier as it gains additional experience. Still, large anesthesia groups, like most hospital-based groups, will likely not be impacted by the VBM due to the complex methodology being used which is weighted heavily to primary care and multi-specialty groups.
Physician Feedback Reports
As required by statute, CMS has provided confidential Physician Feedback reports to certain physicians and groups of physicians since 2010. The reports quantify and compare quality and costs among physicians and physician group practices, relative to the performance of their peers.
In mid-September 2013, CMS plans to disseminate Physician Feedback reports at the TIN level to all groups of physicians with 25 or more eligible professionals. These reports will include a preview of the quality and cost composite methodologies that CMS will use to determine the VBM in 2015 and should help groups of ?100 professionals make an informed decision about electing the quality tiering approach, which they must do by October 15, 2013.
In the fall of 2014, CMS will disseminate Physician Feedback reports for all groups of physicians affected by the VBM in 2015. These reports will be based on 2013 data and will specify the amount of the modifier and the basis for its determination. These reports will be the basis of the VBM in 2015 and would contain, among other things, quality and cost measure performance and benchmarks used to score the composites. CMS plans to provide these reports to all groups of physicians (at the TIN level) with 25 or more eligible professionals even though groups of physicians with 25 to 99 eligible professionals will not be subject to the modifier in 2015. CMS also is examining whether it can provide reports to groups of physicians with fewer than 25 eligible professionals and individual level reports, as well. While these reports will include useful information, they will come too late to influence a larger group practice’s reporting mechanism choice for 2013.
Under statute, CMS also intends to include episode-based cost measures for several conditions in the Physician Feedback reports beginning in 2013 based on 2012 data. CMS is studying how "episode groupers" that would connect all claims for a beneficiary during a certain timeframe may be used in the reports and will seek input from medical specialty societies and other stakeholders on the development and use of episode groupers before phasing these measures into the VBM.
In response to public concerns, CMS continues to work to improve the content, format, and distribution of the Physician Feedback reports. CMS will work with national and state medical specialty societies to ensure that physicians understand the reports, to make the content more meaningful and actionable for quality improvement, and to increase physician awareness of the programs. CMS also has adjusted its procedures for disseminating reports in order to minimize the difficulties physicians may have in obtaining their reports and to ensure reports go to their intended recipients. Finally, CMS plans to make a help desk available to address questions related to the reports.
Participants in the Medicare Shared Savings Program and Center for Medicare and Medicaid Innovation Initiatives
CMS finalized and clarified its proposal to not apply the VBM for 2015 and 2016 to groups of physicians that are participating in the Medicare Shared Savings Program (i.e., ACOs), the testing of the Pioneer ACO model, or other similar Innovation Center or CMS initiatives (such as the Comprehensive Primary Care initiative). These programs are still at their early stages and CMS does not wish to unintentionally disturb those who are already making substantial investments in providing higher quality, more efficient care.
Concerns Remain
While CMS has taken commendable steps to ensure gradual implementation of the VBM program, concerns remain about whether it will be able to collect and analyze enough relevant and meaningful experience by the time it is required to apply the modifier to all physicians in 2017. Physicians are already required to comply with multiple quality reporting mandates while also facing the threat of multiple payment penalties and cuts. Premature implementation of the VBM, paired with these mounting regulatory requirements and payment cuts, will only lead to further confusion for patients and physicians. While CMS must adhere to certain statutory requirements to promote shared responsibility and systems-based care, the ACA gives CMS considerable flexibility in terms of implementing the VBM.
For most groups, electing to be analyzed under the administrative claims-based method will be the best option. ABC will work with all of our clients to help you qualify for the PQRS incentive payments, as long as those remain available, and avoid any PQRS or VBM penalties. We will also continue to publish information on this complex and dynamic subject.
With best wishes,
Tony Mira
President and CEO