February 25, 2013
The Medicare Recovery Audit Contractors have collected a total of $3.9 billion since the program began on a national basis in January 2010. The proportion of underpayments among the “improper” payments uncovered by the RACs has been decreasing. Still, although only 2.9% of all RAC determinations were overturned on appeal, 43.6% of all appeals were successful. Many more determinations are still in the appeals process. Anesthesia and pain medicine practices that accurately document and report patient services—which should be all of them, of course—might consider challenging any adverse RAC action.
CMS’ Medicare Recovery Audit Contractor (RAC) Program has now been in effect in all 50 states for three years. The RACs, readers will recall, are contractors who are compensated on a contingency fee basis for finding and recouping overpayments made by Medicare to physicians, hospitals and other providers. Each of the four RACs is responsible for identifying overpayments—and underpayments—“in a geographically defined area that is roughly one-quarter of the country. In addition, [they] are responsible for highlighting to CMS common billing errors, trends, and other Medicare payment issues,” according to a report from CMS to Congress released earlier this month and entitled Recovery Auditing in the Medicare and Medicaid Programs.
The RACs analyze Medicare FFS claims on a post-payment basis, using three different processes: (1) automated reviews of claims data, (2) semi-automated reviews where the RAC allows the provider to substantiate the claim with supporting documents and (3) complex reviews, where a qualified health care coder or a clinician, depending on the type of review, examines the medical records. The most frequent reasons for determining that a payment has been improper are:
- Failure to meet Medicare's coverage and medical necessity criteria,
- Coding errors, and
- Failure of documentation submitted to support the service or item ordered.
Across three of the four RACs (Connolly, Diversified Collection Services and CGI, Inc.) the most common reason for recoupment is the lack of documentation supporting the medical necessity of inpatient services for certain cardiovascular procedures. In the fourth RAC (Health Data Insights), the most common reason is reporting inpatient stays for minor procedures expected to require a stay of less than 24 hours.
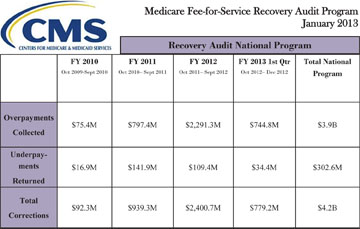
In Fiscal Year 2011, the single year covered by the CMS report to Congress, the RACs corrected $939.3 million in improper payments, of which $797.4 million were overpayments that the RACs collected and $141.9 million were underpayments returned to the providers. The corresponding amounts for the first year of the RAC program, FY 2010 through the first quarter of FY 2013 are shown in the table below:
We note the following about the RAC program trending:
- The amount of overpayments collected increased tenfold from Fiscal Year 2010 to 2011 and by a multiple of three in FY 2012. In the first quarter of FY 2013 (November-December 2012 and January 2013), overpayments collected were almost as great as in all of FY 2011.
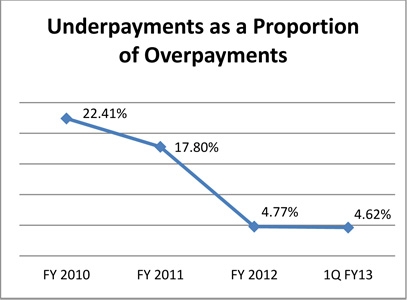
- The ratio of underpayments returned to overpayments collected has decreased markedly, from 22.41% in FY 2010 to 4.62% in the most recent quarter:
It thus appears that the RACs are becoming more active and aggressive each year. CMS claimed that the RACs had achieved a cumulative accuracy score of 90% or higher in 2011, and that only 2.9% of all RAC determinations were overturned on appeal.
The dollar value of attempted recoupments of alleged overpayments is considerably greater than the actual amount recovered, however. In FY 2011, the amount in fact returned to Medicare was $488.2 million out of a total of $939.9 million in payments determined to be improper, or 52 percent. The other 48 percent went to refunding underpayments, appeals, contingency payments, and program costs.
Most significantly, of the 60,717 claims appealed in 2011, 26,469 claims—43.6%—were overturned.
By CMS’ own admission, a large portion of the FY 2011 overpayment collections resulted from short-stay inpatient hospital admissions that should have been provided in the outpatient setting. (FY 2011 was the first year RACs reviewed short-stay inpatient hospital admission issues.) But according to one knowledgeable attorney quoted in Bloomberg BNA’s Health Care Fraud Report on February 20, 2013, some of the short-stay recoveries in the CMS report may be ephemeral, as many (up to 75%) are still in the appeals process and they “’are based on the recovery of the full amount Medicare paid for the inpatient stay, whereas ALJs [administrative law judges] are now routinely remanding appeals of those recoveries for a determination of how much would have been paid if the services had been provided in an outpatient setting (assuming the inpatient stay was not medically necessary).’”
Data from the American Hospital Association’s RACTrac survey show that hospitals are successfully resisting. In the third quarter of 2012, denials climbed—but more than 40 percent of all RAC denials were appealed. Providers won their appeals more than 74 percent of the time.
On October 24, 2012, the American Hospital Association wrote to HHS Inspector General Daniel R. Levinson calling upon the OIG to pay particular attention to the extent that RACs are inappropriately denying payment for medically necessary services. And on November 1st, the Association, together with four hospital systems, filed a lawsuit in the U.S. District Court for the District of Columbia seeking to invalidate an HHS policy that allows RACs to deny claims due to the fact that a service should have been provided on an outpatient basis as opposed to an inpatient setting.
Meanwhile, CMS itself feels enough heat that it published, on December 17, 2013, a paper entitled Medicare Fee-for-Service Recovery Audit Program Myths. Among the myths that the Agency saw the need to debunk are the following:
- RACs deny every claim that they review
- RACs have a contingency fee between 30 and 50 percent (it is in fact 9.5 to 12 percent)
- Every RAC denial is overturned on appeal
- RAC have non-clinicians conduct review of medical records and do not have physicians on staff
- RACs do not tell anyone what they are reviewing
- RACs outsource all the medical review to staff in India and the Philippines
CMS’ self-consciousness about the RAC program may not extend to the four RACs themselves. These organizations are driven by the prospect of the contingency fees and although anesthesia practices have not yet had much adverse experience with RAC audits, the past does not necessarily predict the future. The best defense, as always, is correct reporting of services, supported by the anesthesia or medical record.
With best wishes,
Tony Mira
President and CEO