February 8, 2010
- What makes pain medicine different?
- What defines profitability for a clinical service?
- What distinguishes successful practices?
These three linked questions were the focus of the talk presented by ABC Vice President Jody Locke at the ASA Practice Management Conference in Atlanta on January 30, 2010.
There are two answers to the first question, for purposes of understanding profitability. First, while the anesthesiologist in the operating room does not control his own productivity or case-mix, the physician in the chronic pain clinic decides how busy he wants to be and defines the scope and type of services he will provide. Second, while the fundamental unit of measurement for anesthesia services is the “anesthesia unit” (base or time or modifying unit), chronic pain is measured by encounters.
An encounter consists of all the services provided to a patient on a date of service (evaluation, procedure, and fluoroscopy). “Yield per encounter” is the overall average yield for all types of encounters based on total revenues received, which, multiplied by “encounters per clinical day,” gives us the total gross revenues for a practice. Profitability is determined by subtracting overhead costs from gross revenues. Understanding these metrics and analyzing your own data are fundamental to the profitability of your practice.
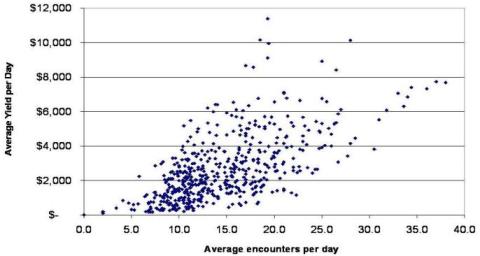
Looking at data from multiple practices in Figure 1 below, Mr. Locke estimated generally that a pain physician should perform 15-17 procedures (encounters) per day and generate about $2,000 just to cover costs. If the daily yield is lower, the practice may not be able to afford to dedicate an anesthesiologist full-time to the pain service.
Figure 1. Where Is Your Practice?
It is critical to understand the role of overhead costs in establishing the profitability of a pain practice. Overhead depends very much on where the physician provides her services. In a hospital-based practice, she is only entitled to the “professional” as opposed to the “technical” component of the fee; her overhead and exposure are limited, and her referrals are defined by the hospital. In a freestanding clinic, on the other hand, the pain physician will be entitled to the entire fee for each service (professional plus technical components); she will be responsible for all overhead and expenses, and she will have to generate referrals to fill her schedule. Overhead may easily run to nearly 50 percent of gross revenues in a private office while they will typically be 10 percent or less in the hospital, where the pain practice is not paying for space or equipment or nursing and technical staff.
Additionally, payment for pain procedures and evaluation and management (E&M) services differs according to “site of service.” The difference between Medicare rates for hospital-based and office- or clinic-based services can vary from approximately 30 percent to more than 150 percent.
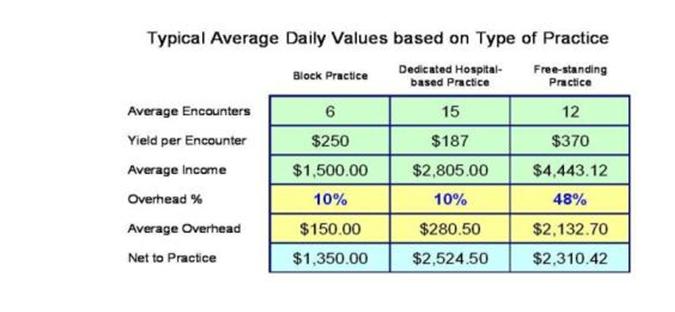
The combined effect of the differences in overhead and in third-party payments can easily make a hospital-based clinic (as opposed to a simple “block practice” that performs pain procedures as needed in the OR suite) more profitable than a practice with its own facility. See Figure 2 below.
Figure 2. Typical Average Daily Net Revenues Based on Type/Site of Practice
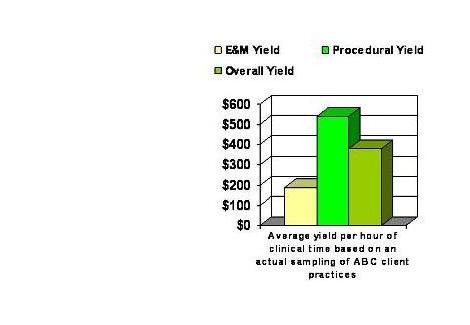
 The successful pain practice increases its profit margin not just by filling its schedule, but by filling it with the right mix of procedures. Interventional procedures, together with fluoroscopic guidance, produce higher net revenues per hour than do E&M services (which is of course why the top rungs of the physician income ladder are not occupied by internists or pediatricians). Medicare allows $74 for a Level 3 hospital outpatient visit in Michigan, for example. The physician would need to perform more than 27 such visits per day in order to break even ($2,000 ÷ $74). Figure 3 shows the difference in fees generated by the two types of service.
The successful pain practice increases its profit margin not just by filling its schedule, but by filling it with the right mix of procedures. Interventional procedures, together with fluoroscopic guidance, produce higher net revenues per hour than do E&M services (which is of course why the top rungs of the physician income ladder are not occupied by internists or pediatricians). Medicare allows $74 for a Level 3 hospital outpatient visit in Michigan, for example. The physician would need to perform more than 27 such visits per day in order to break even ($2,000 ÷ $74). Figure 3 shows the difference in fees generated by the two types of service.
Figure 3. Average Yield Per Hour, Procedure vs. Visits
The financial success of a pain practice depends, first and foremost, on providing excellent clinical service. Paying careful attention to gross revenues, overhead costs and net yield is just as critical to the sustainability of the enterprise. It is true that “you cannot measure what you cannot manage.” Mr. Locke’s presentation demonstrated, however, that you may be able to manage very well the practice for which you have solid metrics.
ASA is to be congratulated on its latest highly successful Practice Management Conference. More than 600 anesthesiologists and practice executives attended the conference in Atlanta. Other presentations included “Employment Situations: The Aging Partner, What to Do About Compensation, No Call, and When the Doctor Does Not Want to Cut Back” (Shena Scott, MBA), “Pitfalls with Managed Care Contracts” (Genie Blough, MBA), “Change: Creating a Culture of Success – The New Generation” (Jeffrey Vender, MD), “Anesthesiology Practice Consolidations & Acquisitions: Survival of the Mid-Size Group” (Judith Semo, JD), “The Joint Commission: What You Need to Know and What You Need to Show” (Robert Lagasse, MD) and an update from the executive director of the Anesthesia Quality Institute (Richard Dutton, MD). Monographs will be available on the ASA web site. Next year’s conference will be held in Houston. See you there!
With best wishes,
Tony Mira
President and CEO
Click here to download a PDF of this eAlert