November 21, 2016
Although adverse events in anesthesia are relatively rare, they do happen. The Agency for Healthcare Research and Quality (AHRQ) has developed a communication resolution program called CANDOR (Communication and Optimal Resolution) that gives clinicians and healthcare organizations a framework for responding promptly and fairly to harmful events. The program provides a simple plan that supports quality and safety improvement as well as risk management.
“We realize mistakes happen, and we can forgive that,” says patient advocate Carol Hemmelgarn, whose nine-year-old daughter died of medical error and a hospital-acquired infection (HAI) in a teaching hospital. “But you harm us again by not being honest and transparent with us . . . we should be healing and learning together how to prevent this from happening to someone else.”
Hemmelgarn’s plea for honesty, transparency and shared learning is reflected in a recently introduced patient safety program from the AHRQ called CANDOR. Developed as an outgrowth of demonstration and planning projects conducted as part of a $23 million Patient Safety and Liability grant initiative launched by the agency in 2009, the program gives hospitals and clinicians a process for responding in a timely, transparent and, ultimately, more effective manner when unanticipated events lead to physical, emotional or financial harm to a patient.
As John H. Eichhorn, MD, writes in the Anesthesia Patient Safety Foundation’s comprehensive adverse event protocol for unanticipated intraoperative events:
Precisely because anesthesia care has become so safe in terms of the reduction of major intraoperative anesthesia accidents, very few anesthesia practitioners today have any first-hand experience dealing in real time with a major anesthesia adverse event. While from an overall anesthesia patient safety statistical perspective, this fact is highly desirable, it also functionally represents a new danger. There is absence of experience, training, or even thought about what to do in the extremely unlikely, but yet still possible event of coming face-to-face with an intraoperative anesthesia catastrophe. This deficit might prevent definitive action that can help the specific patient in a particular incident and patients in general who can benefit by lessons learned from that adverse incident.
What the AHRQ program offers that the APSF protocol does not is a comprehensive communication and resolution process involving the affected patients, families and clinicians, along with guidance in bringing about the cultural acceptance and change needed to implement the process organization-wide.
Safety Data
Despite recent strides, hospital patient safety data shows that harm continues to occur. For example, approximately one in 25 hospital patients acquired an infection during their stay in 2011, according to a 2014 study published in the New England Journal of Medicine. Patients acquired more than 720,000 infections in hospitals, and about 75,000 of those patients died, the Centers for Disease Control and Prevention (CDC) reports.
Concerted efforts on the part of hospitals have paid off in the form of a 50 percent decrease in central line-associated bloodstream infections (CLABSI) between 2008 and 2014 and an eight percent decrease in Clostridium.difficile (C.difficile) infections between 2011 and 2014, according to the CDC’s National and State Healthcare-Associated Infections Progress Report, published in 2016. Still, each day, “more than 200 Americans with healthcare-associated infections will die during their hospital stay,” Tom Frieden, MD, MPH, CDC director, says in a statement.
Open Communication
When an adverse event does occur, hospitals have traditionally had a strong tendency to disclose as little as possible about what happened, says Richard Kronick, PhD, former director of the AHQR, in a video on the agency’s website.
The purpose of CANDOR is to enable healthcare organizations to move away from that avoidance in favor of a process based on openness and fairness that supports continuous improvement. The process revolves around the following key elements (also see the diagram below):
- Providing emotional first aid to patients, families and caregivers immediately
- Maintaining ongoing communication as understanding of the cause of the event grows
- Learning to prevent similar adverse events from happening in the future
- Providing just and timely resolution
- Explaining how care will be safer for future patients
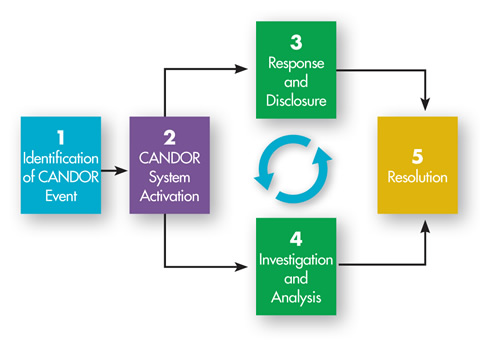
A diagram of the communication resolution process developed by the Agency for Healthcare Research and Quality. The process is described in detail in the agency’s online tool kit.
“When patients have been harmed during a hospital stay, we can’t always undo the harm that has occurred, but we can change the way we respond,” adds Richard Umbdenstock, former president and CEO of the American Hospital Association, in the video. “CANDOR urges transparency from the beginning, teaching providers to be honest, to rebuild trust.”
Hospitals have tended to rely on legal counsel to deal with events such as these before attempting to address them upfront with patients and families in a timely and supportive manner. It’s an approach that does not work well for patients, clinicians or hospitals, Dr. Kronick says.
“It’s very important to try to figure out the process of what happens after harm occurs, and even more important, to try to figure out how to reduce harm to begin with,” he says. “It is clear from the evidence we’ve generated that the implementation of communication resolution programs can be successful in achieving both of these goals.” A demonstration project resulted in a 22 percent reduction in malpractice premiums for one hospital and saved Medicare and Medicaid $3 million.
Resources for Implementation
As William Sage, MD, JD, professor of law at the University of Texas at Austin, puts it in the video: “We have several generations of physicians who believe in patient autonomy and believe in informed consent. If one should and, under law, must, tell patients about what could happen to them, don’t you think we should tell patients about what did happen to them?”
The communication resolution process does not view error disclosure as an isolated event, but rather, as the opening of a conversation, and the approach can be transformative for a healthcare organization, he says.
To help hospitals and practices implement the communication resolution program, the AHRQ has developed an eight-module online tool kit to:
- Engage patients and families in disclosure communication following adverse events.
- Implement a Care for the Caregiver program for providers involved in adverse events.
- Investigate and analyze an adverse event to learn from it and prevent future adverse events.
- Review and revise the organization’s current processes to align with the CANDOR process.
- Establish an organization-wide resolution process.
Modules include an implementation guide, an overview of communication resolution principles, strategies for obtaining organizational buy-in and support, tools to evaluate gaps between the organization’s existing process and a more effective communication resolution process, a guide to systematically analyzing and investigating events, an introduction to the response and disclosure process, a multi-faceted program to assist caregivers involved in events, instruction in effective resolution, and steps to ensure that the communication resolution process becomes a sustainable part of the hospital’s organizational framework.
Notes Richard C. Boothman, JD, chief risk officer of the University of Michigan Health System, on the CANDOR website: “One of the misconceptions of the CANDOR process is that it’s just a big mea culpa every time something goes wrong. The real truth of this approach has little to do with the malpractice part of it. It has everything to do with reconnecting a sense of accountability for the clinical outcomes that we have. At its core, it is literally as simple as saying we’re not going to push things to lawyers when maybe there’s a clinical explanation that is way more important to the key mission of healthcare in general.”
Despite good intentions and best efforts, clinicians occasionally make mistakes. A transparent process that immediately begins a meaningful conversation with the patient, family and caregivers involved, analyzes what went wrong and implements steps to prevent it from happening again will go a long way toward enabling healthcare organizations to achieve their safety goals and fulfill their mission.
With best wishes,
Tony Mira
President and CEO