September 8, 2015
The Medicare Value-Based Payment Modifier, the Physician Quality Reporting System and the Electronic Health Record meaningful use incentive program will all sunset in 2018. They will be replaced by a single program, the Merit-Based Incentive Payment System, for most providers. A number of providers will opt alternatively to participate in an Alternative Payment Model. The details of these new programs will be established over the next few years through federal rule-making.
In last week’s Alert, we looked at Medicare’s Value-Based Modifier (VM) and the Quality and Resource Use Reports (QRURs) that will explain how the VM will affect individual payments. This week we will take a closer look at where Medicare’s move from volume to value will be heading after the VM system sunsets at the end of 2018, as laid out in the payment reform legislation (H.R. 2) that did away with the Sustainable Growth Rate (SGR) methodology in April of this year:

Starting in 2019, the amounts paid to eligible professionals (EPs) will be subject to adjustment for “value” through either the MIPs or an APM, depending on which option the individual EP selects.
The MIPS will replace three cumbersome, costly and almost-unintelligible programs, i.e., the VM, the Physician Quality Reporting System (PQRS) and the Meaningful Use [of Electronic Health Records] incentive program. In concept, at least, it represents a real improvement. Moreover, the aggregate level of financial risk to physicians has been mitigated in comparison to current law, which will expose them to cumulative penalties of up to nine percent in 2017.
How the MIPS will operate remains to be determined. The MIPS will evaluate performance in four categories:
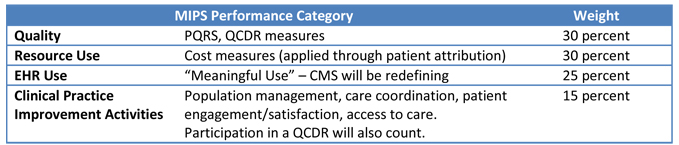
EPs who participate in the MIPS will be subject to a maximum bonus or penalty rising from four percent in 2019 to nine percent in 2022 and beyond, based on their MIPS scores and how these compare to previously established performance thresholds on a 100-point scale. Providers scoring above the threshold will receive MIPS bonus payments. Those providers with higher performance scores will receive proportionately larger payments, bonuses of up to three times the annual penalty cap (i.e., up to a 12 percent increase in 2019.) These bonus payments will be funded by the penalties assessed against providers scoring below the threshold. Additionally, MACRA provides $500 million each year from 2019 to 2024 as a further performance adjustment for EPs in this program who achieve exceptional performance. Apart from that temporary bonus pool, the MIPS is designed to be budget-neutral so the value of positive adjustments will depend upon how the number and aggregate cost of negative adjustments. Beyond that, it is impossible to provide much information until CMS begins to develop MACRA regulations. We do not know, for instance, which measures and criteria from existing Medicare quality reporting programs will be retained; what the measures, reporting periods and thresholds will be. According to the AMA’s Detailed Summary of MACRA, however,
In many respects, the MIPS program should be more attainable for physicians than current quality programs. The MIPS program presents the first real opportunity for high-performing physicians to earn substantial bonuses, and for all physicians to avoid penalties if they meet prospectively-established quality thresholds. Several new aspects of the MIPS program support physicians scoring better, and receiving more credit for their efforts, than under current programs.
For many physicians, APMs may prove to be the better option. Physicians who receive a “significant” percentage of their income from APMs that involve risk of financial losses and quality reporting requirements will have the option to opt out of MIPS. Notably, physicians would only be subject to the quality reporting requirements for their APM. Instead of the MIPS adjustments, they would receive an annual five percent bonus payment between 2019 and 2024.
Again, the legislation provides broad outlines, leaving it to CMS to define exactly what qualifies as an APM and what amounts to a significant percentage of income. At a minimum, APMs will include the Medicare Accountable Care Organizations and patient-centered medical homes.
Stanley W. Stead, M.D., M.B.A. in his July 2015 article in the ASA Newsletter (An Update on the Division of Professional Affairs MACRA Strategy: Quality Reporting and Contribution to Savings) estimates that “payments to physicians in APMs are likely to constitute 60 percent of Medicare physician spending in 2019 and to continue to increase thereafter” and asks what this may mean for physician anesthesiologists. Dr. Stead’s answer: “Physicians using FFS [fee for service Medicare] will have to successfully report on quality, meaningful use and the value-based system, and this undefined “clinical practice improvement activities” to maintain their current levels of payment, and perhaps a little more. In addition, we must prepare to work with alternate payment models,” including, of course, the perioperative surgical home.
There are numerous other provisions contained in MACRA’s 300 pages in addition to those addressing the MIPS and the APMs. None are more important, however, or go farther in advancing the transition from volume-based reimbursement to value-based payments. The specialty and its individual members must ramp up their efforts to report real quality and anesthesia’s contributions to health care cost savings.
With best wishes,
Tony Mira
President and CEO