June 1, 2015
The OIG issued a report in May indicating that Medicare has overpaid hundreds of millions of dollars for claims incorrectly coded as “facility” rather than “nonfacility.” CMS is paying attention; so should anesthesiologists and pain physicians.
The Office of the Inspector General (OIG) reported in May 2015 that Medicare made up to $33.4 million in overpayments for claims on which the place of service (POS) was coded incorrectly during the period from January 2010 through September 2012. (Incorrect Place-of-Service Claims Resulted in Potential Medicare Overpayment Costing Millions.) Reports finding that Medicare has overpaid usually lead to heightened scrutiny of the conduct at issue. Thus it is important that pain physicians, anesthesiologists and their billing staff understand POS coding.
The Medicare Physician Fee Schedule provides for payment at a higher rate for services performed in doctors’ private offices (the “nonfacility” rate) than for the same services performed in a “facility” such as a hospital or ambulatory surgical center (ASC). The difference accounts for the increased practice expense that physicians generally incur by providing care in their offices and other nonfacility locations, including private clinics. When a physician provides services at a facility location, Medicare reimburses him or her for the services and makes a separate payment to the facility to cover the facility’s overhead expense.
Physicians are required to identify the place of service by reporting the appropriate codes on the claim forms that they submit to their Medicare contractors. (Medicare Claims Processing Manual Chapter 26 Section 10.5.) There are dozens of POS codes that distinguish between such locations as schools, prisons, pharmacies, urgent care clinics, etc. Those that an anesthesiologist or pain physician will typically use are the following:
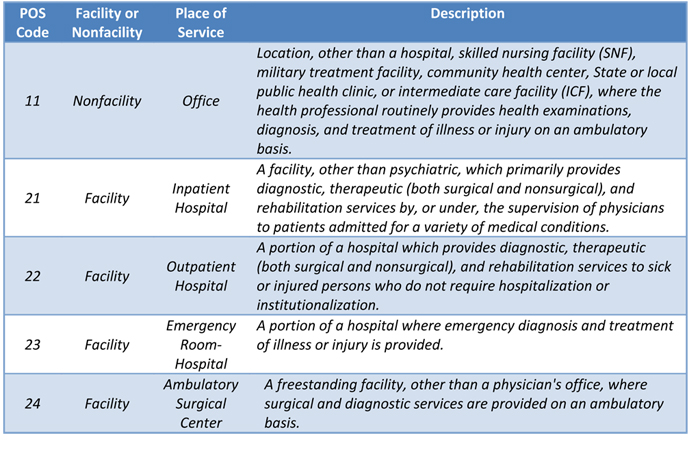
Using POS 11 (Office) instead of POS 22 (Hospital Outpatient) when the anesthesiologist in fact performed the visit or the pain procedure in the hospital would trigger a higher Physician Fee Schedule payment than Medicare allows. For example, the national allowable payment for a Level 3 outpatient visit for an established patient, Code 99213, is $72.94 in the office and $51.13 in a facility, both using the current Medicare conversion factor. The comparable office payment for a lumbar epidural injection (Code 62311) is $92.25 while the facility amount is $245.70.
There is no POS payment differential for anesthesia services—or for a number of procedures that are unlikely to be performed in the office setting such insertion of a Swan-Ganz catheter, Code 93503. Anesthesia claims, like all others, nevertheless require a POS code, and it is important to select the appropriate one because some procedures are only payable if performed on a hospital inpatient basis (POS 21) as opposed to in the outpatient (POS 22) setting. Other procedures performed by anesthesiologists do trigger different allowable amounts depending on where they are done, e.g., central venous catheter insertion, Code 36556 ($237.77/nonfacility; $125.14/facility).
The OIG undertook the recent review because a series of previous audits for the years 2005 through 2009 revealed a total overpayment estimate of more than $62,700,000. Specific contractor and provider audits added another $10,753,532 to the total amount overpaid. The improper billing was particularly problematic when physicians and other suppliers furnished services in outpatient hospitals and in ASCs. Accordingly, CMS released a MLN Matters article (MM7631) in 2013 to educate physicians and their billing staff on the use of the POS codes. Of particular note, the article states that:
Physicians/practitioners who perform services in a hospital outpatient department will use, at a minimum, POS Code 22 (Outpatient Hospital). Code 22 (or other appropriate outpatient department POS code as described above) will be used unless the physician maintains separate office space in the hospital or on the hospital campus and that physician office space is not considered a provider-based department of the hospital …. Physicians will use POS Code 11 (office) when services are performed in a separately maintained physician office space in the hospital or on hospital campus and that physician office space is not considered a provider-based department of the hospital….
By “at a minimum, POS Code 22" will be used, CMS indicates that POS 22 will be acceptable for services furnished in the outpatient hospital setting even if a more specific code is available:
If the physician/practitioner is aware of the exact setting the beneficiary is a registered hospital outpatient, the appropriate outpatient facility POS code may be reported consistent with the code list annotated in this section (instead of POS 22). For example, physicians/practitioners may use POS code 23 for services furnished to a patient registered in the emergency room.
In the May report, the OIG concluded that the apparent POS coding errors and potential overpayments were attributable to internal physician billing control shortcoming and also to insufficient post-payment reviews at the Medicare contractor level. The OIG therefore recommended “that CMS direct its Medicare contractors to continue to educate physicians and billing personnel on the importance of internal controls to ensure the correct place-of-service coding for physician services,” and in its response to the draft report, CMS concurred with the recommendation, as well as with the OIG’s recommendation “to expand and strengthen efforts to perform coordinated data matches of nonfacility-coded physician services and facility claims to identify physician services that are at a high risk for place-of-service miscoding and recover overpayments.”
Reasons given to the OIG for erroneously coding facility services as nonfacility included the following, which are consistent with a lack of adequate controls:
- Billing personnel were confused about the precise definition of a “physician’s office” or other nonfacility location or were simply following established practices in applying the nonfacility codes.
- Some billing personnel were unaware that an incorrect place-of-service code could result in an increased Medicare payment.
- Billing personnel made isolated data entry errors.
- Undetected flaws in the design or implementation of some billing systems caused all claims to be submitted with a nonfacility location as the place of service.
The OIG’s and CMS’ interest in preventing improper POS billing and in recovering overpayments for services incorrectly billed as “nonfacility” is clear. Inadequate training and/or systems shortcomings create vulnerabilities that can be mitigated. POS coding is not overly complex. We encourage readers to review their own coding patterns and practices for conformity to Medicare’s POS rules.
With best wishes,
Tony Mira
President and CEO