May 4, 2015
ERAS protocols lead to improved outcomes, reduced rates of complications, shorter inpatient stays and significant cost savings. They are going to be an important feature in many perioperative surgical homes.
The term “Enhanced Recovery After Surgery” and the acronym ERAS are familiar to most anesthesiologists and to other clinicians. Anesthesia administrators and non-physician advisors may not have encountered the ERAS concept yet. Because of burgeoning interest in better evidence-based perioperative care protocols leading to improved patient outcomes in this era of value-based payment, administrators and practice management staff should acquire a basic understanding of the ERAS concept.
“Enhanced recovery after surgery (ERAS) protocols are multimodal perioperative care pathways designed to achieve early recovery after surgical procedures by maintaining pre-operative organ function and reducing the profound stress response following surgery. The key elements of ERAS protocols include preoperative counselling, optimization of nutrition, standardized analgesic and anesthetic regimens and early mobilization.” (M. Melnyk, RG Casey, P. Black, A.J. Koupparis. Enhanced recovery after surgery (ERAS) protocols: Time to change practice? Can Urol Assoc J. 2011 Oct; 5(5): 342–348). Also referred to as “optimized patient care” or “fast-track surgery,” ERAS protocols and programs lead to improved outcomes, reduced rates of complications, shorter inpatient stays and significant cost-savings. Initiated by Professor Henrik Kehlet in Denmark in the 1990s, ERAS programs have become an important focus of perioperative management after colorectal surgery, vascular surgery, thoracic surgery and radical cystectomy.
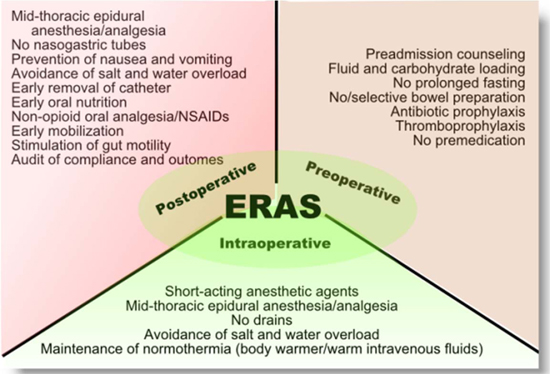
According to the ERAS® Society website, there are “about 20 care elements that have been shown to influence care time and postoperative complications. The following graph illustrates the components of the ERAS multimodal care pathway:
Also according to the ERAS Society website, use of the ERAS pathway has been shown to reduce care time by more than 30 percent and to reduce postoperative complications by up to 50 percent. A 2014 study in the Journal of the American Medical Association of the protocol's use for colorectal surgery in a community hospital setting found it helped reduced stays from 6.7 days to 3.7 days without an increase in 30-day readmission rates. Narcotic use dropped from 63 percent to 15 percent of patients. Studies have shown the protocol could save anywhere from $2,000 to $7,000 per surgery. The review by Melnyk et al. noted a recently published a cost analysis of ERAS in colorectal surgery in which the authors found that there was a significant reduction in total hospital stay, intravenous fluid use, complications and duration of epidural use in the ERAS group: “The implementation of an ERAS program costs about $102 000, but this was offset by costs saved in reduced postoperative resource utilization, with an overall cost-saving of roughly $6900 per patient.”
It should be noted that the evidence of ERAS programs’ effect on costs is not unequivocal. In another colorectal surgery study summarized by Alex Macario, MD, MBA in a 2014 Medscape Viewpoint article, Enhanced Recovery Protocol for Colorectal Surgery, the median length of stay was reduced from seven to five days with the enhanced recovery protocol compared with the traditional group. Patients who received the enhanced recovery protocol also had fewer urinary tract infections (13% vs 24%) and fewer readmissions (9.8% vs 20.2%). Even with a shorter length of stay and lower patient ward costs, nevertheless, there was no statistically significant difference in unadjusted total hospital costs for patients who received the enhanced protocol compared with traditional care ($18,377 vs $20,537).
Adoption of ERAS protocols has been slow, for reasons summarized by Vijaya Gottumukkala, M.B, B.S, M.D. and Henrik Kehlet, M.D., Ph.D. (Optimized Perioperative Care: Why Is Change So Difficult? And What Can We Do To Overcome Barriers?, ASA Newsl 2014 Dec;78(12): 14-16): “lack of awareness of advances in enhanced recovery programs among the anesthesia community, lack of interest in reviewing surgical literature, concerns of liability with initiating something new (deviation from standard teaching), realization that the process of implementation is too long and with many barriers (multi-disciplinary), the belief that enhanced recovery is a surgical and not anesthetic issue, and finally, resistance to new ideas.”
The development of the perioperative surgical home (PSH) is going to increase the popularity of ERAS programs, which reflect some of the features of the PSH but places less direct emphasis on patient care coordination. As David C. Mackey, MD and Michael P. Schweitzer, MD, MBA state in their article The Future of Surgical Care in the U.S.: State Surgical Quality Collaboratives, Optimized Perioperative Care, and the Perioperative Surgical Home (ASA Newsl 2014 Dec;78(12): 13-165): “For most U.S. health care institutions and health care systems, it is the PSH concept—which is fundamentally based upon patient-centric, systems-oriented, interdisciplinary, team-based, global surgical care, along with a payment model to support this surgical care delivery model—that will provide the necessary enabling environment for OPC [ERAS] to be sustainably implemented. And these concepts will synergistically reinvigorate the value provided by physicians to health care delivery systems.”
As the potential for providing and demonstrating value continues to grow, readers should expect to read a good deal more about the PSH, ERAS and related concepts in future Alerts.
With best wishes,
Tony Mira
President and CEO