March 2, 2015
Anesthesiologists can bill the transitional care management codes if they assume responsibility for coordinating post-operative patient care and meet the codes’ specific requirements.
Anesthesiologists’ role in perioperative medicine is rapidly expanding. It is now sufficiently visible that some surgeons are concerned about turf; see Brian Dunleavy’s article Perioperative Surgical Home Promotes Perioperativists in the February issue of General Surgery News online.
While much of the attention has focused on the services that anesthesiologists might provide in the pre-operative phase of surgical care, some anesthesiologists are providing care after discharge for a period of up to 30 days—and are being paid directly for some of that post-operative care. Medicare has recognized two transitional care management (TCM) codes (CPT™ codes 99495 and 99496) since January 1, 2013. Private payers may cover the service, but few, if any, have chosen to do so.
This year, the national unadjusted Medicare payment amounts for services provided in the facility setting are $111.91 (99495) and $161.25 (99496). For some anesthesiology practices, it makes financial as well as clinical sense to provide these services.
The Two TCM Codes
TCM involves care coordination in the 30 days following a Medicare patient's discharge from an inpatient hospital, skilled nursing facility, community mental health center, or following outpatient hospital observation services or a partial hospitalization. The two TCM services consist of initial communication with the patient, one face-to-face visit within seven or fourteen days of discharge, and non-face-to-face services that may be performed by the physician or certain qualified nonphysician provider (NPPs) and/or licensed clinical staff under his or her direction. The codes and their descriptors are:
- 99495 – Transitional care management services with the following required elements:
- Communication (direct contact, telephone, electronic) with the patient and/or caregiver within 2 business days of discharge
- Medical decision making of at least moderate complexity during the service period
- Face-to-face-to-face visit, within 14 calendar days of discharge
- 99496 – Transitional care management services with the following required elements:
- Communication (direct contact, telephone, electronic) with the patient and/or caregiver within 2 business days of discharge
- Medical decision making of high complexity during the service period
- Face-to-face-to-face visit, within seven calendar days of discharge
Requirements for Reporting TCM
The basic elements for each of the two TCM codes are:
- Communication with the patient and/or caregiver within two business days of discharge via telephone, e-mail or face-to-face.
CMS’ Medicare Learning Network paper on TCM elaborates:
For Medicare purposes, attempts to communicate should continue after the first two attempts in the required 2 business days until they are successful. A successful attempt requires a direct exchange of information and appropriate medical direction by clinical staff with the beneficiary and/or caregiver and not merely receipt of a voicemail or e-mail without response from the beneficiary and/or caregiver. You may not bill the TCM if there was no successful communication within the 30-day period between the facility discharge and the date of service for the post-discharge TCM code.
- The level of decision-making (moderate or high complexity) corresponding to the code reported.
The 1995 and 1997 Documentation Guidelines for Evaluation and Management Services describe the components of each level of medical decision making. For each level, two of the three elements must be either met or exceeded. The two lowest levels are included in the table below in order to make the intent of the codes as clear as possible.
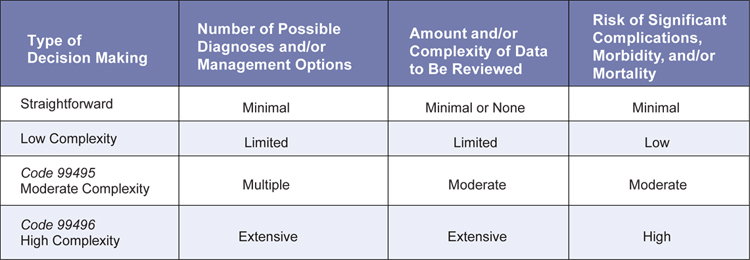
- A face-to-face visit within fourteen calendar days (99495) or within seven calendar days (99496).
Non face-to-face services are also required, although the number and nature of such services are left up to the discretion of the physician, except that the CPT TCM guidelines state that medication reconciliation must take place no later than the date of the face-to-face visit.
The non face-to-face services may be provided by the physician or other NPP (certified nurse-midwives, clinical nurse specialists, nurse practitioners and physician assistants; nurse anesthetists and anesthesiologist assistants are not covered). These services may include:
- Obtaining and reviewing discharge information;
- Reviewing need for or follow-up on diagnostic tests and treatments;
- Communication with other qualified health professionals who will care for the patient’s system-specific problem;
- Patient or caregiver education;
- Arranging referrals, and
- Assisting in scheduling follow-up with community providers and services.
Certain non face-to-face services may also be provided by clinical staff under the direction of the physician or NPP in the private office setting under the “incident-to rules.” It is extremely unusual for anesthesiologists to provide TCM services in private offices and we will refer readers who are interested to the CPT guidelines and to the Medicare Learning Network paper referenced above.
Other Points to Note
- TCM applies when patients are discharged to home, including assisted living—but not when they are discharged to a skilled nursing facility.
- Only one physician or NPP may report TCM services for an individual patient for the 30 days starting with the day of discharge. The claim should be dated on the 30th day after discharge, e.g., for a discharge on March 1st the billed date would be March 30th. Premature claims account for a large proportion of those denied.
- See #2: only one provider will be paid for the TCM codes and Medicare will pay the first claim that it reviews. It is important, therefore, to communicate with other physicians involved in the patient’s post-operative care so that all understand who will be in charge of the TCM and who will be seeking Medicare payment.
- If the patient is readmitted within the 30-day period, TCM services can still be reported as long as the services are furnished during the 30-day period, including the time following the second discharge. Alternatively, the physician can bill for TCM services following the second discharge for a full 30-day period as long as no other provider bills the service for the first discharge
- If the patient dies during the 30-day period, TCM should not be billed, but it may be appropriate to bill evaluation and management services.
- The TCM code only covers one evaluation and management service, so any other encounters during the 30-day period can be billed separately.
Physicians need to be careful how they report the TCM codes, which have some very specific requirements, as described in this Alert. Medicare claims data from 2013 show a 36.3% denial rate in 2013 for code 99495 and a 38.5% denial rate for 99496. To avoid denials, anesthesiologists should make sure to document the following information, at a minimum, in the patient’s medical record:
- The date the patient was discharged;
- The date of the first interactive contact with the patient and/or caregiver;
- The date of the face-to-face visit; and
- The complexity of medical decision making (moderate or high).
Anesthesiologists who are expanding their perioperative role and managing patients’ care for the 30 days following discharge (the same window of time as is defined in the perioperative surgical home model) should consider billing for TCM.
With best wishes,
Tony Mira
President and CEO