Although the majority of hospital-based ABC clients have implemented an electronic medical record, or plan to implement one in the near future, many of our ambulatory surgery center clients have been slower to move from paper to a digital platform. However, the transition is an inevitability for all practices. We review the essentials of a successful EMR implementation, with a focus on ensuring that the chosen system provides an effective means of communicating all of the critical data elements for anesthesia billing.
February 11, 2019
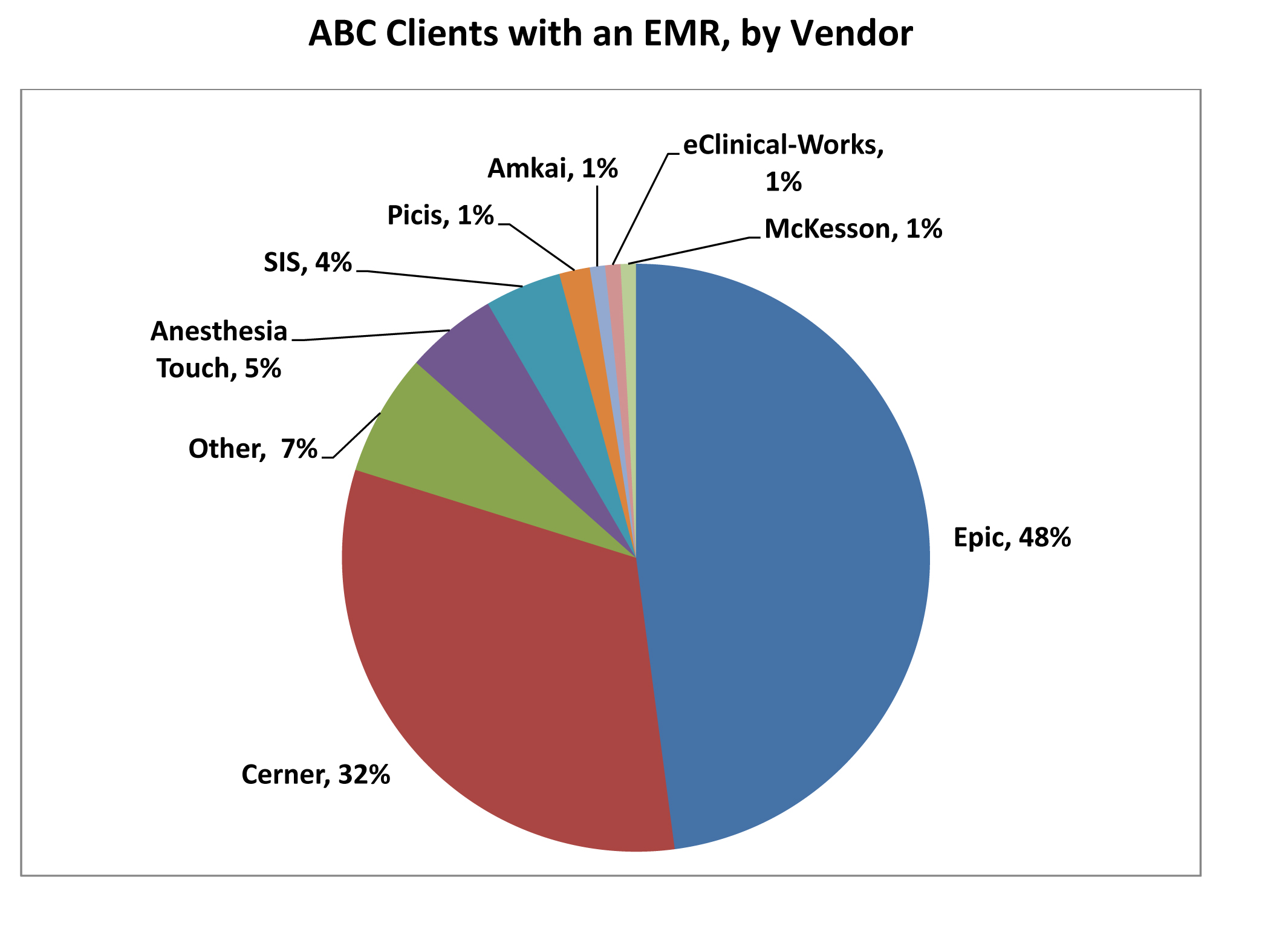
Thanks to our extensive client base, ABC has gained a unique perspective on the pros and cons of electronic medical records (EMRs) and the challenges anesthesia groups face in implementing them. In fact, the transition from a paper anesthesia record to an electronic record is so significant that ABC has established a special transition team to assist clients in ensuring that the EMR they implement will support anesthesia billing’s specific requirements.
Most of ABC’s hospital-based clients have implemented an EMR or plan to implement one in the near future, while our ambulatory surgery center (ASC) clients have been somewhat slower to make this transition. However, all practices will inevitably make the change to a digital platform. To support these efforts, this eAlert offers insights and tactics for an effective EMR implementation from ABC’s Jody Locke, vice president for anesthesia and pain practice management services, and Karen Gehne, director of EMR integration.
As soon as we learn that a hospital is planning to transition the anesthesia department to an electronic record, we suggest that key providers begin working with our team to delineate how critical data elements will be captured and transmitted. There is a common misbelief, promoted by EMR vendors, that the EMR will allow a direct feed to the billing office. We have yet to see that happen. Virtually every EMR must be modified to suit the practice’s needs.
We have learned some valuable lessons over the years from our extensive experience managing our clients’ EMR implementations. For most clients, the EMR consistently provides the details our coders need to code each case and calculate a charge based on the pdf image of the anesthesia record. We have also found that the EMR provides a valuable tool with which anesthesia providers can record relief in the care team model as well as intraoperative activity/discontinuous time.
To help ensure an effective EMR implementation, it is critical to:
- Designate a key member of the practice to work closely with the EMR vendor to ensure that the practice’s specific billing and documentation requirements can be met. This virtually always means the system needs to be modified.
- Establish a mechanism to validate the number of records received. A certain percentage of records do not get identified for a variety of reasons, including software updates in the EMR system.
Many of the documentation deficiencies we find are related to lack of understanding of or attention to the EMR system’s requirements among the anesthesia providers. Not all providers embrace a new technology with the same level of interest and enthusiasm.
Following are some specific items that anesthesia groups should pay close attention to:
Pre-op Block Placement
- Will pre-op block placement be included within the anesthesia record?
- If there is a separate block placement note, how will that be sent to the biller and connected with the anesthesia record?
Post-op Pain Management Rounding
- How will this visit be documented and what mechanism is available to send this note to the biller?
Blood Patch and Emergency Intubation
- Is there capability to create an ad hoc anesthesia record or procedure note? How will this information be sent to the biller?
- Can this service be pulled into a report listing to ensure that the information is billed?
Labor Epidural
- How will you capture face-to-face or interval visits?
- When a labor epidural moves to a C-section, is it captured as one anesthesia case or as two separate cases? How will the biller know that the labor epidural became a C-section?
Workflow
When researching an EMR, consider your workflows. Will the EMR support the various workflows, or are changes required due to EMR functionality? Some EMR implementation projects will use the current workflow as the template with which to build the new EMR process. However, it is important to consider when moving from paper to an EMR that new functionality will be required to capture more data.
Remember also that in the EMR world, the surgeon is responsible for communicating the post-op procedure and diagnosis. Is a process in place to allow the surgical procedure and diagnosis to be entered into the anesthesia record before it is closed? Some procedures need additional information before the anesthesia services can be billed. Is there an area on the EMR where this additional information can be entered?
EMR Functionality
How easy is it to create a data and image transfer from the EMR to your biller? Does the EMR come with this functionality or is this something that the IT project team will have to create?
Types of Information Transferred for Billing
- Patient demographic, guarantor and insurance data
- Anesthesia record PDF
- Case as completed listing for use as an audit tool
Access for Billing
- View/print remote access to the EMR system for pulling additional information such as operative reports, H&P, etc.
There was a time when the discussion about EMRs focused on their potential value to the practice and the facility. This question no longer matters; the eventual implementation of an EMR is virtually inevitable for every practice. What matters now is ensuring that the chosen system provides an effective means of communicating critical billing elements. Careful planning, regular communication and verification are the keys to making that happen.
ABC clients: We have learned from our work with clients during their transition to an EMR that the sooner we can become involved in the implementation process, the smoother the transition. If you have questions or would like further information, please feel free to contact Karen Gehne, director of EMR integration, at Karen.Gehne@anesthesiallc.com.
We want to hear from you. Do you have a topic you would like to see covered in an ABC eAlert? Please send your suggestions to info@anesthesiallc.com.
With best regards,
Tony Mira
President and CEO