April 10, 2017
The interscalene block is not a new technique, but its acceptance as a routine anesthetic modality for shoulder surgery has evolved slowly. A review of the ABC client base indicates additional potential for the use of this block with ultrasonic guidance. Anesthesia practices should review their data to assess that the reasons for not doing a block are appropriate based on patient and surgeon expectations. We encourage ABC clients to request a documentation review to ensure compliance and payment for all services provided.
The specialty of anesthesia is in a constant state of evolution as practitioners seek new modalities to safely manage patients through the discomfort and trauma of surgery. As providers experiment with new procedures, such as nerve blocks for postoperative pain management, ultimately, each new modality is evaluated on three levels: technical expertise, clinical efficacy and financial viability. The use of interscalene blocks for the management of postoperative pain associated with painful shoulder procedures provides us with a useful case study, highlighting the various prerequisites for a successful rollout of a new modality.
The typical anesthesia practice now routinely provides interscalene blocks for many types of shoulder surgery, and some anesthesiologists now perform sciatic and femoral blocks for procedures on the knee, ankle and foot. There is also interest in some quarters in other types of blocks, including transversus abdominis plane (TAP) blocks for abdominal procedures and paravertebral blocks for breast procedures. When medically reasonable and necessary, the use of these blocks over the past five years has resulted in additional revenue. The question in many practices is whether this opportunity will continue and whether there are other ways to take advantage of nerve blocks to enhance patient care and practice finances.
What has made the use of interscalene blocks so popular? While the successful administration of an interscalene block requires a certain degree of training, most anesthesiologists seem to master the technique with little difficulty. The typical block does not require more than 15 minutes, and many are completed in less time. The resistance appears to come less from anesthesia providers than from certain orthopedic surgeons who do not consider the block worth the time it delays the case.
The administration of these blocks is further enhanced by the use of ultrasonic guidance (USG). Most hospitals now have this technology readily available where needed. The ability to clearly visualize the needle and the brachial plexus has significantly increased the accuracy of the blocks and the efficacy of their administration. Data indicates that patients who receive interscalene blocks are more comfortable and have fewer postoperative complications.
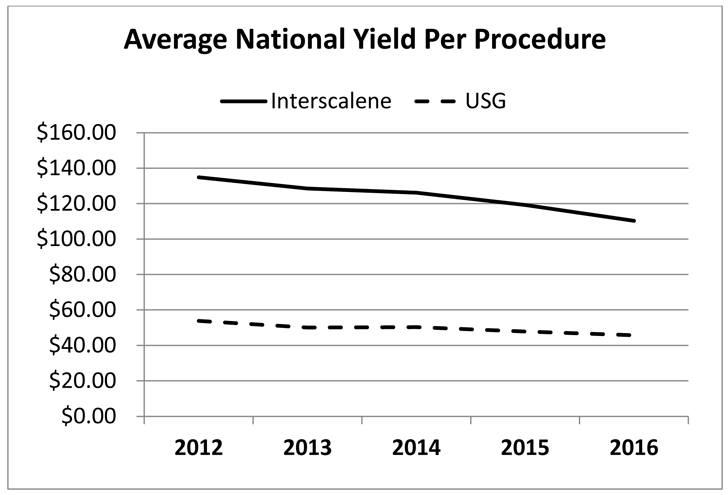
The interscalene block is not a new technique, but its acceptance as a routine anesthetic modality for shoulder surgery evolved slowly until the evidence was clear that providers would get paid for the service. A five-year review of ABC client utilization of these blocks clearly indicates that a subset of more progressive practices has consistently used these blocks, while others have slowly gotten up to speed. Based on the ABC database, the use of interscalene blocks for a limited number of surgical procedures on the shoulder has become the standard of care. The chart below is based on a study of the shoulder procedure that most commonly involves an interscalene block, CPT Code 29827 (Endoscopy/Arthroscopy Procedures on the Musculoskeletal System). The sample includes 135 practices across the country that performed, on average, about 15,000 arthroscopic rotator cuff repairs per year for the five years beginning January 1, 2012.
The law of supply and demand suggests that as the supply of a particular service increases and demand is satisfied, the price will start to drop. Thus far, this has not been the case for the block or the USG. For many practices, this means that what would have been a $500 case is now worth closer to $650, which is a significant increase for relatively little additional work.
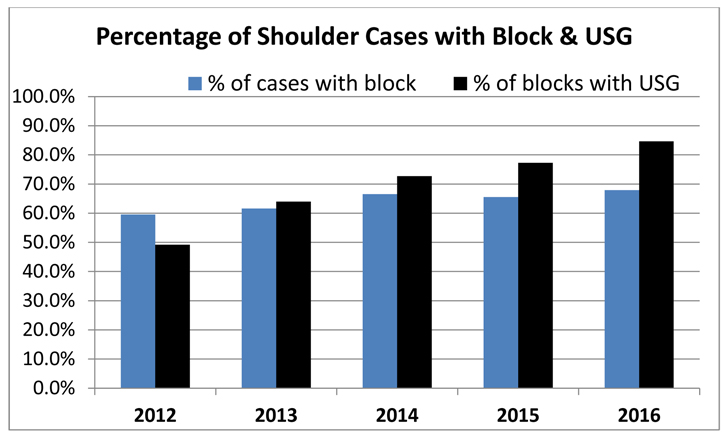
Anesthesia providers are always looking for services that represent the intersection of clinical efficacy and financial viability. A review of the ABC client base indicates additional potential for the use of this block with USG. While overall utilization has increased over the past five years, even now, only about two-thirds of these shoulder cases involve the use of a nerve block for postoperative pain management.
There are many reasons why a nerve block might not be performed for a particular case, but the takeaway here is that each practice should review their data to assess that the reasons for not doing a block are appropriate based on patient and surgeon expectations. In our experience, sometimes blocks do not get billed because the documentation is deficient. A careful review of the documentation requirements of incidental procedures is always useful. More important, though, is to ensure that the compliance requirements are consistently being met to safeguard that appropriate payment is being received for all the valuable services provided.
For more information about the documentation requirements for these services and a comprehensive review of your utilization, contact your ABC account manager.
With best wishes,
Tony Mira
President and CEO