Obstructive Sleep Apnea: The Not-So-Silent Killer
Brian J. Thomas, JD, Director of Risk Management & Senior Claims Attorney,
Preferred Physicians Medical, Shawnee Mission, KS
As the prevalence of obesity in the general population is rapidly increasing, so too is the incidence of obstructive sleep apnea. Anesthesiologists face significant challenges and risks when treating patients with diagnosed obstructive sleep apnea or patients who exhibit all the signs and symptoms of obstructive sleep apnea. Concurrent with the increase in obesity and obstructive sleep apnea, Preferred Physicians Medical’s loss data reflect an increase in allegations of medical negligence involving obstructive sleep apnea patients. These cases often involve catastrophic brain damage or death. In light of the increased risks presented by obstructive sleep apnea patients, anesthesiologists frequently seek risk management advice for managing these challenging patients.
Obstructive Sleep Apnea Defined
Obstructive sleep apnea (OSA) is defined as upper airway collapse during sleep that may be accompanied by sleep disruption, hypoxemia and arterial oxygen desaturation. OSA is common in obese patients due to the propensity of fat deposition in the pharynx causing the upper airway to close. However, non-obese patients can have OSA from tonsillar hypertrophy or craniofacial abnormalities, especially in pediatric patients. OSA disrupts normal sleep patterns and results in arousal events that may lead to other symptoms including, but not limited to, hypertension, coronary artery disease, congestive heart failure, fatal arrhythmias, myocardial infarction, daytime somnolence, diabetes, and restrictive pulmonary disease.
 Preoperative Assessment
Preoperative Assessment
 Preoperative Assessment
Preoperative AssessmentPreoperative assessment of patients for potential identification of OSA includes: 1) medical record review, 2) patient and/or family interview, 3) physical examination, 4) sleep studies, and 5) preoperative x-rays for cephalometric measurement in selected cases. All obese patients, BMI ? 30, undergoing surgery should be suspected of having OSA preoperatively. There are several screening tools and scoring systems available to assist anesthesiologists in evaluating whether a patient might have OSA. However, it should be noted these screening tools and scoring systems have not been clinically validated and should be used as a guide in evaluating patients for OSA. In the absence of a sleep study, a presumptive diagnosis of OSA may be made using the STOP-BANG scoring model (see Figure 1).
Other physical characteristics such as enlarged tonsils, prominent tonsillar pillars, enlarged nasal turbinates, narrowed maxilla or mandible, pronounced tongue and enlarged adenoids are often reflected by a high Mallampati score used by anesthesiologists to predict difficulty with intubation. A high Mallampati score, with anticipated intubation difficulty, should alert the anesthesiologist and perioperative team to the high potential for OSA.
Preoperative Management
Prescribing sedatives preoperatively may be problematic for OSA patients, as they are often sensitive to sedatives, especially if the OSA is untreated. Even minimal sedation can cause airway obstruction and ventilatory arrest. Therefore, many anesthesiologists do not give preoperative sedatives to patients with OSA, unless the patient can be carefully monitored.
 The most serious perioperative complication is the loss of airway control after induction of general anesthesia. Because of reduced oxygen reserve due to decrease in lung volume in the morbidly obese patient, these patients cannot tolerate a lack of ventilation for appreciable periods before hypoxemia results. It is for that reason anesthesiologists should be prepared for a difficult intubation and have all of the necessary resources and equipment, including supraglottic devices, to follow the ASA difficult airway algorithm. It may also be prudent under certain circumstances to have an experienced surgeon available at the time of induction of general anesthesia in case tracheostomy becomes necessary. An alternative to general anesthesia for OSA patients is regional anesthesia (epidural, intravenous regional or peripheral nerve block).
The most serious perioperative complication is the loss of airway control after induction of general anesthesia. Because of reduced oxygen reserve due to decrease in lung volume in the morbidly obese patient, these patients cannot tolerate a lack of ventilation for appreciable periods before hypoxemia results. It is for that reason anesthesiologists should be prepared for a difficult intubation and have all of the necessary resources and equipment, including supraglottic devices, to follow the ASA difficult airway algorithm. It may also be prudent under certain circumstances to have an experienced surgeon available at the time of induction of general anesthesia in case tracheostomy becomes necessary. An alternative to general anesthesia for OSA patients is regional anesthesia (epidural, intravenous regional or peripheral nerve block).
Postoperative Care
 The period of awakening from anesthesia can be problematic for patients with OSA. In patients who have undergone surgery for treatment of their OSA, the airway can be narrowed from swelling and inflammation. Also, the lingering sedative and ventilatory depressant effects of the anesthetic can pose difficulty. Perioperative vigilance should continue into the postoperative period. Some patients require postoperative intubation and mechanical ventilation until fully awake. A CPAP machine can be used in some patients postoperatively to reduce obstruction, especially if a patient has been on a CPAP preoperatively. For some patients, it may be prudent to admit them to an intermediate care or intensive care area postoperatively to facilitate close monitoring and airway support measures. Narcotics can precipitate or potentiate apnea that may result in ventilatory arrest. If narcotics are deemed necessary in the post-operative period, appropriate monitoring of oxygenation, ventilation and cardiac rhythm should be provided.
The period of awakening from anesthesia can be problematic for patients with OSA. In patients who have undergone surgery for treatment of their OSA, the airway can be narrowed from swelling and inflammation. Also, the lingering sedative and ventilatory depressant effects of the anesthetic can pose difficulty. Perioperative vigilance should continue into the postoperative period. Some patients require postoperative intubation and mechanical ventilation until fully awake. A CPAP machine can be used in some patients postoperatively to reduce obstruction, especially if a patient has been on a CPAP preoperatively. For some patients, it may be prudent to admit them to an intermediate care or intensive care area postoperatively to facilitate close monitoring and airway support measures. Narcotics can precipitate or potentiate apnea that may result in ventilatory arrest. If narcotics are deemed necessary in the post-operative period, appropriate monitoring of oxygenation, ventilation and cardiac rhythm should be provided. 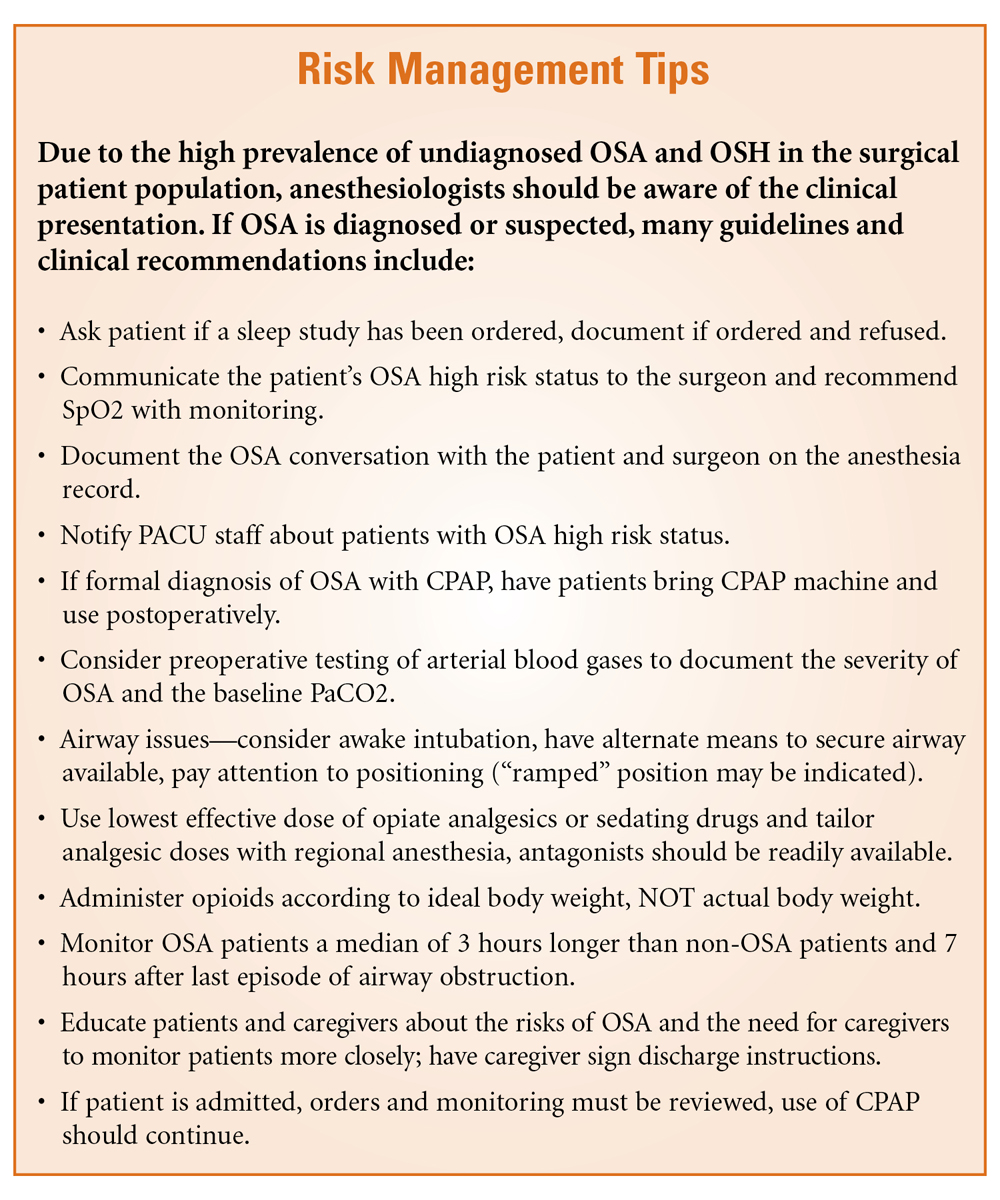 Summary
Summary
Patients with OSA present many challenges to anesthesiologists. Obese and morbidly obese patients are particularly prone to this sleep disorder. Anesthesiologists frequently elicit the symptoms and suspect OSA during examination of the airway and sleep history. Special care must be taken in the management of anesthetic induction, intubation and maintenance of these patients with particular attention to titration of neuromuscular relaxation and analgesic use. Perioperative and postoperative management should ideally include CPAP therapy for those patients with diagnosed OSA. Outpatient procedures must be approached with caution and should include clinical judgment and patient selection criteria based on the severity of OSA, presence of coexisting co-morbidities, invasiveness of surgery, type of anesthesia, anticipated postoperative opioid requirements, and adequacy of post-discharge observation. Anesthesiologists should make their own independent evaluation as to whether a patient is an appropriate candidate for anesthesia in an outpatient surgery facility and admit those patients who do not meet those criteria.
 Brian J. Thomas, JDis Director of Risk Management & Senior Claims Attorney for Preferred Physicians Medical Risk Retention Group, Inc. in Shawnee Mission, KS. He can be reached at (800) 562-5589 or at brian.thomas@ppmrrg.com.
Brian J. Thomas, JDis Director of Risk Management & Senior Claims Attorney for Preferred Physicians Medical Risk Retention Group, Inc. in Shawnee Mission, KS. He can be reached at (800) 562-5589 or at brian.thomas@ppmrrg.com.
References:
1. Isono S. Obstructive Sleep Apnea of Obese Adults. Anesthesiology. 2009;110:908-21.
2. ASA Practice Guidelines for the Perioperative Management of Patients with Obstructive Sleep Apnea. Anesthesiology. 2006;104:1081-93.
3. Doyle JD. Obstructive Sleep Apnea And the Surgical Patient: What the Anesthesiologist Should Know. Anesthesiology News—Guide to Airway Management. Supplement. 2009.
4. Ogan OU, Plevak DJ. Anesthesia Safety Always an Issue with Obstructive Sleep Apnea. See, http://www.apsf.org/newsletters/html/1997/summer/sleepapnea.html.
5. Joshi GP. The Adult Patient with Morbid Obesity and/or Sleep Apnea Syndrome For Ambulatory Surgery. Presentation—American Society of Anesthesiology Annual Meeting, October 16, 2010.
6. Leone, BJ. Obstructive Sleep Apnea and Anesthesia. Revista Mexicana de Anestesiologia. Vol. 30, Suppl. 1, April-June 2007.