eAlerts
-
2016 Coding Updates for Anesthesia
Kelly D. Dennis, MBA, ACS-AN, CANPC, CHCA, CPC, CPC-I
Perfect Office Solutions, Inc., Palmetto, FLWhen you received your 2016 Current Procedural Terminology (CPT) and American Society of Anesthesiologists (ASA) Relative Value Guide (RVG) books or discs, you probably noticed there were no new anesthesia code additions or deletions listed for this year. Since the CPT book usually arrives before the RVG, you may not have taken a good look through your RVG or may not have ordered a 2016 RVG as there were no coding changes. However, there are a number of important updates in the RVG New/ Revised RVG Coding Comments section which are not included in the Anesthesia section of the CPT. These comments may affect the way anesthesia coders assign procedure codes in the upcoming year. As this article will not include all updated comments, be sure to order your 2016 RVG. I’ve chosen a few that are certain to have an impact on 2016 coding for anesthesia services.
Let’s start with 00218, “Anesthesia for intracranial procedures; procedures in the sitting position” with a base value of thirteen units. As you may know, base unit values increase as the difficulty of a procedure increases. The new coding comment indicates “This code may be reported for anesthesia for any intracranial procedure performed with the patient in the sitting position.” For example, although the sitting position for cranial surgery is associated with a high incidence of air embolism (Schubert), a craniotomy or craniectomy for evacuation of a subdural infratentorial hematoma may be performed with a patient in the sitting position. Rather than assigning 00210 “Anesthesia for craniotomy or craniectomy for evacuation of hematoma” with a base unit value of ten, coders will assign 00218. This code assignment also depends on the anesthesia provider clearly indicating on the anesthesia record that the patient was in the sitting position.
 Coders cannot capture billable services that are not indicated on the anesthesia record, even if they are marked on an internal billing sheet. Billing sheets are not usually considered as part of the patient’s medical records. There is no universal anesthesia record and a typical anesthesia billing company sees a number of different records, so coders must determine where on each record anesthesia providers document special positioning, which can be quite challenging with paper records and handwritten notes. With a paper record, the clearest way to document is a legible note in the remarks or comments section. Electronic anesthesia records (EARs) are much easier to read and may have a field summary, which typically includes an area to document when the patient is in the sitting, or any other special position. If the EAR doesn’t have a field summary, look within the body or comments section. If you are not sure where this information is documented, learn where patient positioning information is documented in your practice.
Coders cannot capture billable services that are not indicated on the anesthesia record, even if they are marked on an internal billing sheet. Billing sheets are not usually considered as part of the patient’s medical records. There is no universal anesthesia record and a typical anesthesia billing company sees a number of different records, so coders must determine where on each record anesthesia providers document special positioning, which can be quite challenging with paper records and handwritten notes. With a paper record, the clearest way to document is a legible note in the remarks or comments section. Electronic anesthesia records (EARs) are much easier to read and may have a field summary, which typically includes an area to document when the patient is in the sitting, or any other special position. If the EAR doesn’t have a field summary, look within the body or comments section. If you are not sure where this information is documented, learn where patient positioning information is documented in your practice.There were substantial changes to pacemaker coding comments under CPT codes 00530, 00534 and 00537 (See Table 1). The comments describe anesthesia for pacemaker services and indicate when it is acceptable to report the higher base unit values for active testing of an implantable cardioverter defibrillator (ICD) device or electrophysiologic (EP) testing. So it is important that (1) coders understand the difference, and (2) anesthesia providers are giving enough information to the coders to allow proper anesthesia code selection.
If cardioversion or defibrillator functions are not tested, coders are referred to CPT 00530, with a base value of four units. Documented testing of cardioversion or defibrillator functions increases the base value to seven units and is reported with CPT 00534. If an EP procedure is performed, CPT 00537 with a base unit value of ten is the appropriate anesthesia code. Coders should review these codes and circumstances with providers to ensure documentation supports the anesthesia code selected and reported, and be aware the Center for Medicare and Medicaid Services (CMS) has assigned a lower unit value than the RVG for EP procedures (See Table 1). The anesthesia codes for pacemaker related services are not listed in the MLN Matters article “National Coverage Determination (NCD) for Single Chamber and Dual Chamber Permanent Cardiac Pacemakers” (Number MM9078) as requiring a -KX modifier (indicating “Requirements specified in the medical policy have been met”) for Medicare patients, although the surgeon may be required to report a -KX modifier.
Another common area of interest to anesthesia coders is related to extracorporeal shock wave lithotripsy (ESWL). When I first started in anesthesia more than 32 years ago, it was common to see treatment for lithotripsy while the patient was immersed in a water bath; however, now it may be more common to see other types of ESWL treatment. According to Dr. Grasso, “In first-generation lithotriptors (Dornier HM3), the patient was placed in a water bath. However, with second- and thirdgeneration lithotriptors, small waterfilled drums or cushions with a silicone membrane are used instead of large water baths to provide air-free contact with the patient’s skin.” The 2016 comment for CPT 00872 indicates, “Use only when patient immersed in water bath. With small water filled drums/cushions, see 00873.” As there is a base unit value difference of two units between these codes, coders should ensure they are reporting as instructed. If you are not certain whether your practice’s facilities still use water bath or not, it’s time to check!
CPT codes 36221–36626 describe non-selective and selective arterial catheter placement and diagnostic imaging of the aortic, arch, carotid and vertebral arteries. The 2016 ASA Crosswalk revises the reported anesthesia code for each of these procedures to 01916, “Anesthesia for diagnostic arteriography/venography” with a base value of five units. This is a substantial change from 2015 crosswalk codes ranging from six to ten base units.
Aside from multiple valuable comment and crosswalk code revisions, it is noteworthy that the 2016 RVG no longer includes ASA standards and guidelines relevant to coding and billing in the back of the book. The bad news is that it is no longer a matter of flipping through to the end of the RVG to access information when coders need to provide “proof” of why we do the things we do. The good news is the ASA provides all current version of their standards and guidelines on the ASA website (See Resources). While the information is not as convenient, unless you have internet access, keep in mind there is added value to having access to the most up-to-date information ASA provides.
Trying to keep up with ongoing changes to the Physician Quality Reporting System (PQRS) coding is a constant challenge for coders. There were no changes to the 2016 requirements for reporting cross-cutting measures, although a number of new cross-cutting measures have been added. However, PQRS coding is a different story.You may have noticed in CPT Appendix B – Summary of Additions, Deletions and Revisions that there were textual changes to Category II Code 6030F (removing “cap and mask and sterile gown and sterile gloves and a large sterile sheet and 2 percent chlorhexidine” from the code description), and there were no Category II code deletions—but that doesn’t mean anesthesia coders don’t have to worry about deleted PQRS codes. Although Measure #44 (Category II Code 4115F) is still listed as a valid code, CMS removed this measure from claimsbased reporting. Code 4115F is still a valid code for registry reporting along with CPT 00562. In a nutshell, effective January 1, 2016, Measure #44 is no longer reportable if your anesthesia practice is using claims-based PQRS reporting.
Similarly, although Category II Codes 4250F and 4255F (Measure #193) are both still listed in the 2016 CPT, 2015 will be the last reporting year for this measure. Measure #193 has been retired and, it too, will no longer be reportable effective January 1, 2016. These changes, announced in the final physician fee schedule rule, which was published in the Federal Register on November 16, 2015, leave claims-based reporting anesthesia groups (estimated at 80 percent) only one PQRS measure specific to anesthesia – Measure #76 (Category II Code 6030F). Since anesthesia providers do not have nine measures across three domains, they will automatically be subject to the Measures Applicability Validation (MAV) process (unless they make a measure applicable to themselves by reporting it even once “unsuccessfully,” e.g., by appending the -8P modifier that shows that the measure wasn’t performed and doesn’t indicate that there was a valid reason for the non-performance. Many anesthesiologists unfortunately fell into this trap, which deems them to have failed PQRS altogether, for payment year 2016 based on 2104 reporting.)
The MAV applies to both claims-based and registry-based reporting, though the methodology differs. With claims-based, as there is only one applicable anesthesia measure (#76), as long as your provider meets the 50 percent threshold and also reports at least one “cross-cutting measure” if any apply (see below), no penalty should be assessed. Keep in mind that a claim with an -8P modifier, which indicates the action was not performed and no reason was documented, does not count toward the 50 percent threshold—or successful performance. Surprisingly, many anesthesia providers who successfully performed and reported PQRS in 2014 received a 2016 penalty notice (based on a two year look back period) and it appears other specialties experienced the same issue. Fortunately, the American Medical Association (AMA), Medical Group Management Association (MGMA) and the ASA are aware of the problem and are working toward a potential solution.
Unfortunately, anesthesia practices that do not place Swan Ganz or Central Venous Pressure (CVP) lines have no associated claims-based PQRS measures. According to the PQRS help desk (Quality Net communication to author), “if you are not able to report Measure #76 via claims, you are required to hire a registry for reporting the other applicable measures or a Qualified Clinical Data Registry (QCDR).” Although claims-based reporting of PQRS measures has not gone away, if you can’t report the only anesthesia PQRS measure left, registry reporting allows your anesthesia practice to report enough anesthesia specific performance measures to avoid payment penalties in 2018.
Similar to Measure #193, many of the registry-related PQRS codes include “G” codes as listed in the Healthcare Common Procedure Coding System (HCPCS) book. In 2016, there are no longer anesthesia clusters related to claims-based reporting. Cluster Number 38, Anesthesiology Care (for Registry-Based Measures), includes Measures #424, #426, #427 and #428 (See Table 2).
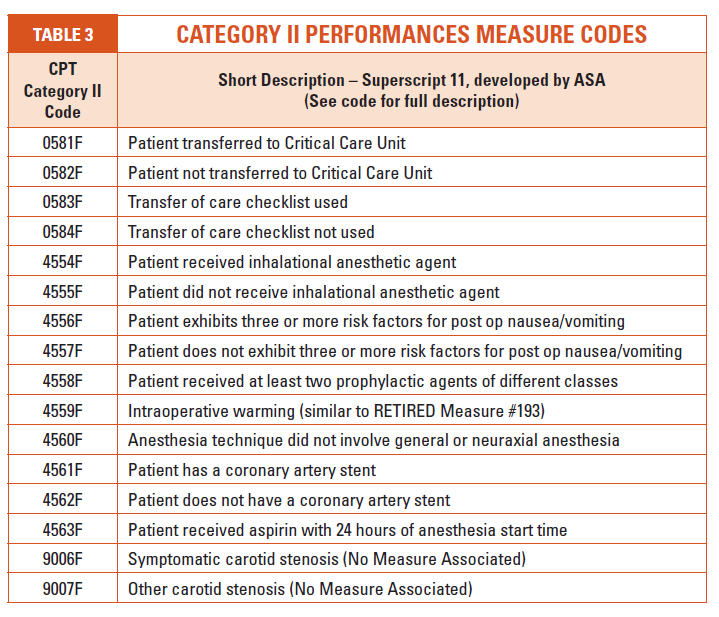
Also, take a few minutes to thumb through the Category II performance measure codes listed in the 2016 CPT. The ASA has been working on developing specific measures relative to quality reporting of anesthesia services (see superscript number 11 under Category II footnotes). Many of these codes appeared in the 2014 CPT and several may look familiar to anesthesia coders. Codes listed in Table 3 are Category II performance measure codes developed by the ASA, although these codes are reported only through a registry.
By 2019, coders will see PQRS segue into a new quality program called the Merit-Based Incentive Payment System (MIPS). Whether you are a seasoned coder or new to the specialty, anesthesia coding will continue to be unique, interesting and challenging!
Resources
2016 Professional Edition CPT American Medical Association2016 Relative Value Guide and Crosswalk, American Society of Anesthesiologist
Hyperlink Resources
American Society of Anesthesiologist (ASA), Standards and Guidelines
http://www.asahq.org/quality-and-practice-management/standards-and-guidelinesASA, Physician Quality Reporting System Reporting for 2016
http://www.asahq.org/quality-and-practice-management/quality-improvement/physician-quality-reporting-system/PQRS-2016-NoticeCMS Anesthesiologists Center, 2014 Anesthesia Base Units by CPT Code [Zip 13KB] (latest published information, unchanged for 2016 and 2016)
https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PhysicianFeeSched/Downloads/2014-Anesthesia-BaseUnits-CPT.zipCMS, Final Rule containing Revisions to Payment Policies under the Physician Fee Schedule and Other Revisions to Part B for CY 2016
http://www.gpo.gov/fdsys/pkg/FR-2015-11-16/pdf/2015-28005.pdfCMS, 2016 Cross Cutting Measures List
https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/PQRS/Downloads/2016_PQRS-Crosscutting.pdfCMS, 2016 PQRS Claims/Registry Measure Specifications Release Notes https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/PQRS/Downloads/2016_PQRS_IndivMeasures_ReleaseNotes_111715.pdf
CMS, PQRS MAV Process for Registry Based Reporting
https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/PQRS/Downloads/2016_PQRS_IndivMeasures_Guide_11_17_2015.pdfCMS, PQRS Measures Codes
https://www.cms.gov/medicare/quality-initiatives-patient-assessment-instruments/pqrs/measurescodes.htmlCMS, Qualified Clinical Data Registry Reporting
https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/PQRS/Qualified-Clinical-Data-Registry-Reporting.htmlRonald Hirsch, MD, FACP, CHCQM. New Guidance on Pacemakers Come with Needless Modifier: RAC Monitor, March, 2015
http://www.racmonitor.com/rac-enews/1803-new-guidance-on-pacemakers-comes-with-needless-modifier.htmlMichael Grasso, III, MD. Extracorporeal Shockwave Lithotripsy, January, 2015 http://emedicine.medscape.com/article/444554-overview
MLN Matters Number MM9078, NCD for Single Chamber and Dual Chamber Permanent Cardiac Pacemakers, October, 2015
https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/downloads/MM9078.pdfNoridian, NCD for Single Chamber and Dual Chamber Permanent Cardiac Pacemakers - Revised https://med.noridianmedicare.com/web/jeb/article-detail/-/view/10542/ncd-for-single-chamber-and-dual-chamber-permanent-cardiac-pacemakers-revised
Armin Schubert MD, MBA. Positioning Injuries in Anesthesia: An Update. Advances in Anesthesia. Volume 26, October 2008, Pages 31-65
https://www.openanesthesia.org/craniotomy_positioning_injury/
Kelly D. Dennis, MBA, ACS-AN, CANPC, CHCA, CPC, CPC-I has over 32 years experience in anesthesia and speaks about anesthesia issues nationally. She has a Master’s Degree in Business Administration, is certified through the American Academy of Professional Coders, is an Advanced Coding Specialist for the Board of Medical Specialty Coding and serves as lead advisor for their anesthesia board. She is also a certified healthcare auditor and has owned her own consulting company, Perfect Office Solutions, Inc., since November, 2001. She can be reached at kellyddennis@attglobal.net. -
The Perioperative Surgical Home: Our Partnership with the C-Suite
Rick Bushnell, MD, MBA
Director, Department of Anesthesia, Shriners Hospital for Children, Los Angeles, CA and
Huntington Memorial Hospital, Pasadena, CA“CMS’ pay-for-performance reimbursement changes are looming. As members of the Huntington Accountable Care Organization (ACO), anesthesia recognizes the need to improve surgical outcomes. Our collective financial future is tied to solid quality improvements that only increasingly coordinated care can deliver. We will double down on our cooperative effort with our hospital in order to improve medical outcomes, to lower costs and to improve the patient experience.” – Pacific Valley Medical Group, Pasadena, CA.
Summary of Recent Events
The Centers for Medicare & Medicaid Services (CMS) is pushing quality, the American Society of Anesthesiologists (ASA) is pushing the perioperative surgical home (PSH) and our 30-partner Pacific Valley Medical (anesthesiology) Group (PVMG) in Pasadena, CA is picking up both causes. In our commitment to a PSH clinic staffed and managed by anesthesiologists, we are fully embracing the concept of transitional care & perioperative medicine. This is our contribution to our patients and to our Huntington Memorial Hospital’s (HMH) Readmission Reduction Program.This past summer, we made rapid progress toward putting these concepts into operation. In June, two members of our group attended the ASA conference on the PSH. In July, we recruited a few more of our partners. In August, our anesthesia group hosted a presentation by Zeev Kain, MD, MBA of the Department of Anesthesia, University of California, Irvine to our administrators and surgeons. In September, several of us divided up the work (below) and in October, we presented the concept and proposed a partnership with the Huntington Memorial C-suite.
Presentation to the C-Suite
Our hospital administrators have long been aware of the issues of costly readmissions, looming CMS changes and marginal patient experience for some. They can be forgiven for being unaware, though, of how an engaged anesthesia group can help with those issues. Like many anesthesia groups, they were unaware of how an active, mature PSH partnership can meet their needs. In our presentation, then, we started by defining the PSH as (1) a concept, (2) a process and (3) a physical presence.
As a concept, the PSH is the idea that patients experience better surgical outcomes when anesthesiologists are fully engaged in the entire perioperative continuum. Complicated patients do especially better when physician anesthesiologists take responsibility for pre-surgical optimization, in-room anesthesia, immediate post-op care and transitional care medicine. Who better than anesthesiologists to understand the surgical challenges presented to patient physiology? Who better, then, to optimize pre-operative physiology and surveil post-operative outcomes? If not us, who? If not now, when? As an aside, anesthesia groups absolutely must understand their value to the concept of the PSH. Individual anesthesiologists must realize and exercise their superior medical management abilities relative to other care givers. The concept is the ASA’s investment.
As a process, the PSH is the engagement and coordination of anesthesia services throughout the entire continuum of surgical care. From the decision to operate to final disposition of the patient, anesthesiologists must make themselves available to patients, to their surgeon partners and to hospital administrators. In the case of Huntington’s 11,000 annual surgical cases, that seems a very tall order. In order to target resources toward those most at risk, PVMG will design systems to triage our surgical patients. We will assign 20 percent of the sickest to MD pre-op clinic visits, MD operating room anesthesia and MD post-discharge transitional care medical management by anesthesiologists. The remainder will be seen in a pre-op clinic by mid-level providers under MD management. PVMG will invest a full time equivalent anesthesiologist to manage the clinic and to work up patients. The manpower is our practice's investment.
As a physical presence, the PSH is necessarily a location with staff and support from the hospital. It is a substantial investment of both finances and administrative effort in managing 11,000 patients more effectively. Currently, the majority of those elective patients present to the hospital and the pre-operative holding suites the morning of surgery. You can imagine the resulting cancellations and delays that result from last-minute pre-op work that could have been done weeks before the very day of surgery. This patient and information flow is no longer acceptable. It wastes resources and it exposes patients to sub-optimal outcomes. Huntington Memorial is already in process of expanding the physical capacity of this clinic to accommodate all the surgical patents. This physical facility and support staff are the hospital’s investment.After thus explaining the PSH, we presented the PSH anesthesia team to the C-suite: those of us (initials below) who had coalesced into a working group, self-selecting ourselves into areas of responsibility based on our individual natural interests. There will be much other work and room for the remainder of our group, but in addition to seeing patients in clinic our initial responsibilities were divided in this manner:
AF - Goal directed therapy, regional block room, liaison to cardiothoracic section
RY - Data management, research, metrics, liaison to ObGyn section
JH - Pre- & post-operative work-up protocols, liaison to HMH quality committee
LK & AC - Pain management, liaison to orthopedic section
TC - Financial management, billing, negotiations
JM - Executive leadership, politics, liaison to general surgery section
RB - Experience in establishing prepost- op clinic, pace, focus & vision
MM – Liaison to ambulatory surgical centers, clinic duties
MA - Scheduling, office management, clinic duties
CK - Pre- and post-discharge protocols, NICU, PICU and fetal surgery sectionThe proximate result of the presentation of our team was the demonstration of our interest, our motivation, our research and the medical resources we were offering our Huntington C-suite administrators. We wanted them to sense an enthusiastic, well-motivated team, who offered a progressive physician partnership and a well-conceived plan.
Our Initial Goals Included
- Reducing day-of-surgery cancellations by 90 percent by the end of the 1st year
- Reducing surgical length of stay by 20 percent by the end of the 2nd year
- Reducing readmissions by 50 percent by the end of the 3rd year
To accomplish this, we specifically asked our C-suite to consider actively supporting the following program:
- Having every one of our 11,000 elective surgery patients appear in the PSH clinic,
- Triage and identify the sickest 20 percent of patients for pre-op clinic appointments with an anesthesiologist, with assignment to anesthesiologists intra-op, post-op and in post-discharge clinic,
- Improvement of pain management services with a dedicated operative suite nerve block room manned by those anesthesiologists most skilled at ultrasound regional nerve blocks, and
- Establishment of RN/NP/PA/ CRNA intervention teams to improve post-op and post-discharge surveillance and intervention on the hospital floor, in the home setting, in the emergency department and in the post-discharge clinic.
In response, and to our Huntington Memorial C-suite’s great credit, their explicit #1 priority was to improve the patient experience and surgical outcomes. They elaborated their faith in our PVMG anesthesia group as a worthy partner. Demonstrating intuitive understanding of the PSH, the CEO, the CFO and the VP of Quality found this project a worthy investment of their administrative energies and hospital finances. Our C-suite administrators then asked by what means they could facilitate the project.We offered to provide the physician manpower and leadership. Our group would increase the presence of an anesthesiologist in clinic as the patient and management demands increased. We would compensate that physician ourselves (more on physician billing and reimbursement in a future article) and not request a stipend from the hospital. In return, we presented the specific wish list below that included:
- Appoint a Huntington Memorial PSH administrative champion
- Appoint an anesthesiologist physician champion
- Expand the pre-op clinic facilities and increase the nursing staff
- Establish PA/NP/RN/CRNA discharge planning, home health and ER intervention teams
- Expand the role of quality committee to include mid-level HMH administration managers
- Improved collection of patient outcome data within
- Public relations help with and leadership of the effort; HMH as our partner
- HMH must be able to follow the cost, reimbursement and profit on each surgery
- Administrative support in same day surgery for nerve block room to improve the quality of pain management
- Patient data mining and patient triage support
Conclusion
At the end of our presentation, PVMG and Huntington Memorial shook hands on a new partnership.
Huntington named both anesthesiologist and administrative champions. The two of us immediately established weekly standing meetings. Huntington has also offered to support our second evening PSH conference with a presentation from a world class speaker, Maxime Cannesson, MD of the Department of Anesthesia, University of California, Irvine. Sponsored by Edwards Life Sciences, Dr. Cannesson will present the concept of Goal Directed Fluid Therapy and provide updates related to both invasive and non- invasive hemodynamic monitoring.
PVMG has selected anesthesiologists who are ready to see patients in clinics. Our Huntington administrators are fully on board and engaged. Our group is committing physician leadership manpower and Huntington is committing administrative energies and financial support. Together PVMG and Huntington Memorial have forged a progressive Anesthesia/C-suite partnership.
Now more than ever, the PSH is right for our patients, our hospital and our group.
Rick Bushnell, MD, MBA is the Director of the Department of Anesthesia, Shriners Hospital for Children, Los Angeles, CA and a Clinical Anesthesiologist at Huntington Memorial Hospital in Pasadena, CA. Dr. Bushnell graduated from the University of Illinois College Of Medicine and attended the University of Pittsburgh Medical Center, Pittsburgh and Loma Linda University for internship and residency. He has been with Pacific Valley Medical Group since 2003 and consults with Shriners Hospital for Children, Los Angeles. He and his partner have six adopted children in Tanzania where he serves as Visiting Clinical Anethesiologist at St. Elizabeth’s Hospital for the Poor in Arusha. He can be reached at propofolstingsme@gmail.com. -
“I’m Out Of Here!” Now What?
Kathryn Hickner, Esq.
Ulmer & Berne LLP, Cleveland, OHWe all know that the healthcare industry is experiencing a wave of integration. This trend has been evident for many years. Fewer physicians are willing to assume the legal, financial and other business risks associated with owning their own practices. More and more physicians, including anesthesiologists, are becoming employed by large physician groups, health systems and national providers.
This shift necessarily involves not only entry into new employment arrangements but also the termination of existing relationships. And those terminations are often governed by written employment agreements, state and federal healthcare laws and employer benefit plans and other policies and procedures.Before pursuing their next opportunity, physicians should pause for a moment and first attend to the arrangement that they are leaving. Departing physicians need to understand their legal rights and obligations when leaving their current employment relationships in order to avoid unintended consequences and detrimental missteps along the way. Here are a few words of practical advice for physicians contemplating an exit from their current employment arrangements.
- Ensure that the relationship is terminated in accordance with the terms of the written employment agreement. Whether the physician is terminating the employment agreement with or without cause, the physician is facing an involuntary termination initiated by the employer or the parties are mutually agreeing to end the relationship, the parties must terminate the relationship in accordance with the timing, prior notice and other procedural requirements set forth in the written employment agreement, when applicable. Failure to do so can result in a breach of contract claim and sometimes significant liability exposure.
- Avoid relying on verbal promises and assurances regarding the transition. In the event that the parties have mutually agreed to terminate an employment relationship in a manner that is contrary to the terms of the written contract, such agreement should be reduced to writing. Verbal promises and assurances provided by the other party that it will cooperate and agree to waive certain rights under the employment agreement are generally not enforceable unless reduced to writing. Relying upon verbal promises and assurances is especially dangerous when the departing physician’s primary contact is not the ultimate decision maker and lacks ultimate authority to ensure a smooth transition.
- Understand your obligations to obtain tail coverage. Employment agreements that permit professional liability insurance to be maintained on a claims made basis often require the physician (at least under certain circumstances) to assume the cost of obtaining tail coverage upon termination of the relationship. Before exiting an employment relationship, the physician should assess whether such obligation is present and the associated expenses. Note that the cost of tail coverage may vary greatly depending upon the particular state. Sometimes a physician’s obligation to procure tail coverage can be addressed, upon consent of the employer through an amendment to the written employment agreement, through the maintenance of the existing policy or by obtaining nose coverage.
- Determine your rights and obligations to provide patients with notice of your departure. The right of a physician to inform his/ her patients of the departure is often addressed in the underlying written employment agreement. Many state laws also include provisions related to patient notices upon a physician’s departure. Non-solicitation provisions set forth within employment agreements are subject to applicable state law. Further, even when employment agreements include non-solicitation provisions and the state laws are silent on patient notices, physicians are sometimes able to persuade their employers to permit appropriate notices to patients based upon applicable ethical rules, principles of patient choice and continuity of care considerations.
- Assume that noncompetition covenants will be enforced when permitted under applicable state law. It is common for physicians contemplating a departure to express disbelief that their employers would actually want to enforce a restrictive covenant or that a court would compel compliance with such an obligation. But they are often surprised. Employers place non-competes in their agreements for a reason—they believe they are important. When enforceable under applicable state law, non-competition prohibitions may significantly impact a physician’s post-termination career and should be taken very seriously. Physicians should review the restrictions carefully and objectively to ensure complete compliance. Applicable case law often informs how courts will interpret ambiguities within the contractual language (e.g., how the restricted geographic area would be determined). That being said, employers will sometimes grant waivers of such covenants when there is an incentive to do so.
- Consider a separation agreement. In the event that either party has potential claims against the other or there are ambiguities in the underlying written employment agreement regarding the terms of departure, it may be best to enter a separation agreement. Whether a separation agreement is necessary or appropriate depends upon the particular circumstances and each party’s respective negotiating leverage. Separation agreements often include releases of claims and confidentiality, non-disparagement and indemnification provisions. They also often include, for example, provisions related to posttermination access to patient and billing records (for continuing care of patients, audits, litigation, etc.), non-solicitation and non-competition prohibitions, obligations to obtain and pay for tail coverage, the calculation and payment of bonus compensation, payout for unused vacation or sick time, settlement amounts and buy-outs, references provided by the employer to third-parties with respect to the departing employee and reports to licensure bodies, the National Practitioner Data Bank and governmental bodies, as applicable.
- Anticipate collateral consequences, when applicable. Departing physicians should understand the impact that their employment termination may have on any medical staff memberships and faculty appointments. Also, those physicians who participate in or own the employing practice or related or third party physician organizations, accountable care organizations, co-management companies, ambulatory surgical centers, real estate investment entities and other ventures may need to terminate such membership or ownership interests in connection with the termination. Such termination requirements may be set forth in the employment agreement itself or in the shareholder, operating, participation or buy-sell agreements, as applicable.
- Refrain from saying or doing something you regret. Some employment terminations are amicable but others are more like a bitter divorce. In such cases, it is often wise for physicians to take the emotion out of all negotiations and communications with the soon to be former employer and others to the extent possible and rely upon attorneys and other advisors to negotiate the transition when helpful. Employment agreements often contain confidentiality and non-disparagement provisions that apply during and after the term. Even when those requirements are not reduced to writing, physician employees should understand that they are generally not entitled to retain any property, passwords or confidential information of the employer after the termination. Further, even if the governing employment agreement does not include a nondisparagement provision, departing physicians should be careful not to impermissibly defame their employers or violate any applicable fiduciary duties owed to the employer on the way out as such actions can result in substantial legal exposure and financial liability.
Briefly stated, physicians should exit their existing employment relationships with care. It is advisable for physicians to take some time to review the terms of their written employment and related agreements, to understand their rights and obligations under applicable laws (including for example those pertaining to post-termination restrictive covenants, access to records and patient notices) and to understand how employer benefit plans will impact their departure. Before succumbing to the relief, hope, excitement (and perhaps even fear or anger depending upon the circumstances) regarding the termination and what lies ahead, physicians should take a moment to tie up any loose ends before moving forward.
Kathryn (Kate) Hickner, Esq. is an attorney at Ulmer & Berne LLP, where she co-chairs the firm’s Health Care Practice Group. Additional information regarding Kate’s background, experience, publications and presentations can be found at http://www.ulmer.com/attorneys/Hickner-Kathryn-E.aspx. She can be reached via telephone at (216) 583-7062 and via e-mail at khickner@ulmer.com. -
The Evolving Relationships between Anesthesiologists and Their Hospitals and ASCs
By the time this issue of The Communiqué is in your hands, 2015 will be a fading memory and 2016 will have begun to take shape.
One important voice sounding a warning or at least a heads-up about what is coming is that of Mark Weiss, Esq. The title of Mr. Weiss’s article— Impending Death of Hospitals: Will Your Anesthesia Practice Survive?—which is also the title of his forthcoming book—is intentionally provocative. He lays out several of the major threats confronting hospitals, starting with health system growth, through mergers and acquisitions, acquisition of physician practices and investments in integrated delivery networks. Others have predicted that the Federal Trade Commission will place a damper on hospital merger activity in 2016, but the quest for greater scale and scope is going to continue. Anesthesiologists may want to consider the wisdom of relying on the ongoing health of just one or two hospitals. This is especially true in light of the ability of physician-owned facilities, notably ambulatory surgery centers, and new technologies (think telemedicine) to disrupt hospitals’ traditional business. Mr. Weiss concludes in no uncertain terms that anesthesiologists who are not yet deeply engaged with freestanding facility care should turn in that direction.
Of course, with more than 5,600 licensed hospitals in the U.S., the need and opportunity for anesthesiologists in hospitals is not going to dissipate completely in the near future. In the Fall 2015 issue of The Communiqué, Rick Bushnell, MD, MBA explained why forming a perioperative surgical home (PSH) with the active support of the hospital was right for his group. He brings us up-to-date on the process of agreeing upon goals, priorities and resources that has led to the formation of a true partnership in his new article The Perioperative Surgical Home: Our Partnership with the C-Suite.
Jerry Ippolito, MBA, MHSA reminds us all of the continuous need to attend to the well-being of one’s hospital and surgeons in The Hospital is Your Practice’s Client—Understand Client Satisfaction to Retain Your Contract. As Mr. Ippolito states, “Every business, regardless of its service offering or discipline, must continue to reinvent itself, to remain marketable, in changing times. Anesthesia is no exception.”
The arrival of a new year always brings us coding changes. Kelly Dennis, MBA, who is a certified expert coder with 32 years of experience in anesthesia, reviews the changes to the CPT® system and also to the increasingly frustrating Physician Quality Reporting System (PQRS) in 2016 Coding Updates for Anesthesia. PQRS is now in its penultimate year of existence, and we would like to think that the Merit- Based Incentive Payment System that, in 2019, will replace the various Medicare quality reporting programs bedeviling us today will be an improvement. We shall see.
Confidentiality is a topic that perennially looms large in healthcare. Improving or even maintaining health does not take place in a void; information is and must be shared in order to achieve our health-related goals both as individuals and as participants in healthcare systems. One area that engenders confusion is the extent to which personal information gathered and shared in the context of peer review may be protected from disclosure or “discovery” in legal proceedings. Every state has a statute governing the discoverability of records, reports and conclusions. In Confidentiality in the Peer Review Process: What Does it Mean and What is Covered? Part I, Neda Ryan, Esq. reminds readers of the basic principles and considerations and also provides a summary of the statutes for Alabama through Iowa. Part II will appear in the Spring issue of The Communiqué and will contain summaries for the remaining states.
Just as important a legal matter, although one that comes up somewhat less frequently than confidentiality, is covered by Kathryn Hickner, Esq. in “I’m Out Of Here!” Now What? Physicians leaving a practice are often covered by an employment contract with
the group they are leaving and also by federal and state laws regarding employer benefitWe hope that 2016 will be a year of successful and satisfying relationships, old and new, for all our readers.
With best wishes,
Tony Mira
President and CEO -
Confidentiality in the Peer Review Process: What Does it Mean and What is Covered? Part I
Neda M. Ryan, Esq. Corporate
Compliance Attorney, Anesthesia Business Consultants, Jackson, MIDepending on one’s standpoint and experience, the peer review process can bring about mixed feelings in healthcare providers. Opinions about the effectiveness of the process, those who sit on the panel and the outcome are often debated. However, what is often less debated until long after the process has taken place is whether the information reviewed during the peer review process is subject to discovery in other settings.
Generally, the peer review process is a retrospective review of an event or series of events conducted in an effort to improve quality of care. In order to encourage candid review, many states have enacted laws to limit the discoverability of the proceedings, the records reviewed and the records created during the peer review process. In other words, in a civil proceeding, the contents of the peer review meetings and the records discussed are not discoverable and are not subject to a subpoena and the participants in the meetings are not required (or, in many cases, permitted) to testify to or disclose the matters discussed by the committee or its decision. However, in light of these legal protections, many lawyers representing plaintiffs in malpractice cases seek to poke holes in the protection to obtain evidence to support their case against physicians. This unfortunate fact jeopardizes and compromises the effectiveness of the process.
In light of the litigious environment within which all physicians practice, it behooves all anesthesiologists and pain specialists to consider the following:
- Familiarize yourself with the peer review process within your organization and the facilities in which you practice to ensure that retrospective reviews are protected by the privilege.
- It is especially important to consider how to initiate the peer review process to ensure initial inquiries are protected.
- Work with the administration/ risk management in your group or the facilities in which you practice to improve upon the peer review process.
- Ensure any conversations or notations about the peer review committee’s review of an issue remain within the confines of the peer review process. In other words, casual conversations with colleagues or notations in a patient’s record regarding the review may be subject to discovery.
- Familiarize yourself with the types of records that are protected under the privilege in the state in which you practice.
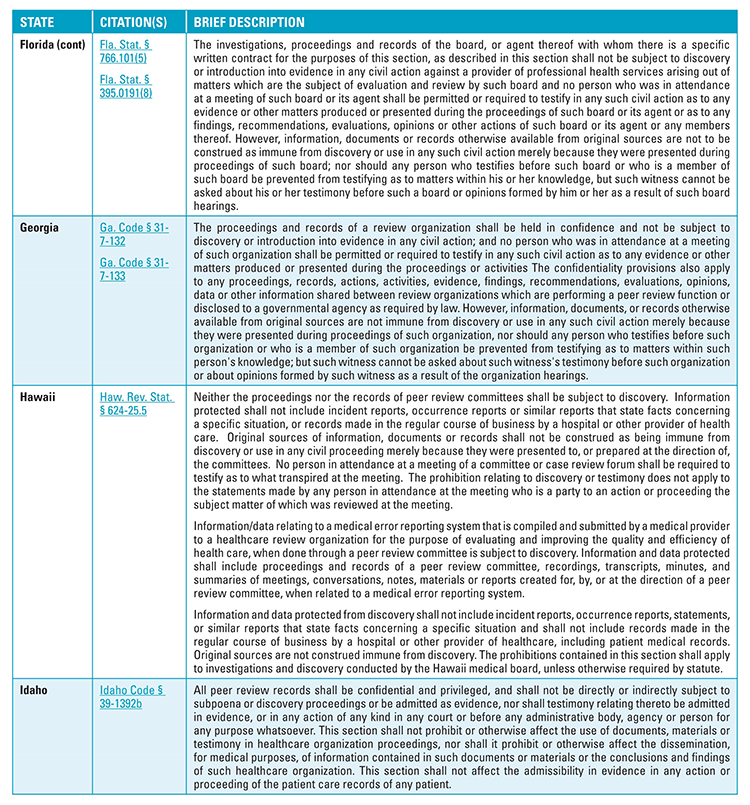
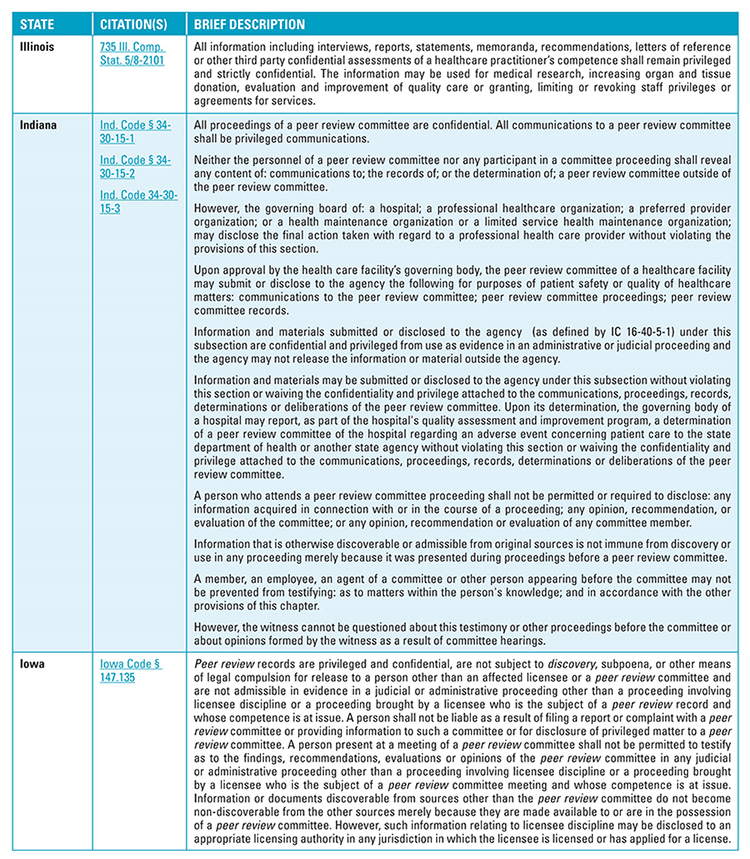
On the next 3 pages, you will find Part I (Alabama through Iowa) of a brief summary of what is protected by the peer review privilege in every state. Please note that the table is meant to be strictly informational and would require a more detailed review of the state’s judicial interpretation of its statutes. A summary of the remaining states (Kansas through Wyoming) will appear in the next issue of The Communiqué.
Neda M. Ryan, Esq. is a Corporate Compliance Attorney for ABC. Ms. Ryan has experience in all areas of healthcare law, including healthcare transactional and corporate matters; healthcare litigation matters; providing counsel regarding compliance and reimbursement matters; and third party payer audit appeals. She can be reached at (517) 787-7432 or at Neda.Ryan@AnesthesiaLLC.com- .
 Coders cannot capture billable services that are not indicated on the anesthesia record, even if they are marked on an internal billing sheet. Billing sheets are not usually considered as part of the patient’s medical records. There is no universal anesthesia record and a typical anesthesia billing company sees a number of different records, so coders must determine where on each record anesthesia providers document special positioning, which can be quite challenging with paper records and handwritten notes. With a paper record, the clearest way to document is a legible note in the remarks or comments section. Electronic anesthesia records (EARs) are much easier to read and may have a field summary, which typically includes an area to document when the patient is in the sitting, or any other special position. If the EAR doesn’t have a field summary, look within the body or comments section. If you are not sure where this information is documented, learn where patient positioning information is documented in your practice.
Coders cannot capture billable services that are not indicated on the anesthesia record, even if they are marked on an internal billing sheet. Billing sheets are not usually considered as part of the patient’s medical records. There is no universal anesthesia record and a typical anesthesia billing company sees a number of different records, so coders must determine where on each record anesthesia providers document special positioning, which can be quite challenging with paper records and handwritten notes. With a paper record, the clearest way to document is a legible note in the remarks or comments section. Electronic anesthesia records (EARs) are much easier to read and may have a field summary, which typically includes an area to document when the patient is in the sitting, or any other special position. If the EAR doesn’t have a field summary, look within the body or comments section. If you are not sure where this information is documented, learn where patient positioning information is documented in your practice.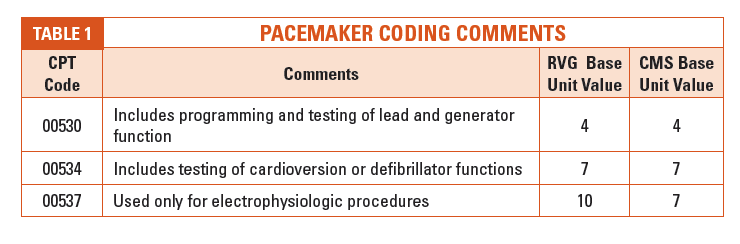
 Trying to keep up with ongoing changes to the Physician Quality Reporting System (PQRS) coding is a constant challenge for coders. There were no changes to the 2016 requirements for reporting cross-cutting measures, although a number of new cross-cutting measures have been added. However, PQRS coding is a different story.
Trying to keep up with ongoing changes to the Physician Quality Reporting System (PQRS) coding is a constant challenge for coders. There were no changes to the 2016 requirements for reporting cross-cutting measures, although a number of new cross-cutting measures have been added. However, PQRS coding is a different story.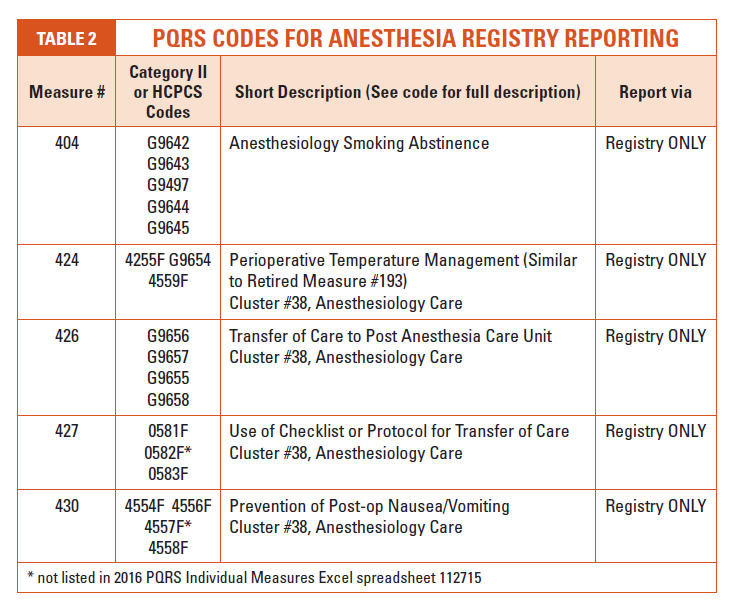
 Kelly D. Dennis, MBA, ACS-AN, CANPC, CHCA, CPC, CPC-I has over 32 years experience in anesthesia and speaks about anesthesia issues nationally. She has a Master’s Degree in Business Administration, is certified through the American Academy of Professional Coders, is an Advanced Coding Specialist for the Board of Medical Specialty Coding and serves as lead advisor for their anesthesia board. She is also a certified healthcare auditor and has owned her own consulting company, Perfect Office Solutions, Inc., since November, 2001. She can be reached at
Kelly D. Dennis, MBA, ACS-AN, CANPC, CHCA, CPC, CPC-I has over 32 years experience in anesthesia and speaks about anesthesia issues nationally. She has a Master’s Degree in Business Administration, is certified through the American Academy of Professional Coders, is an Advanced Coding Specialist for the Board of Medical Specialty Coding and serves as lead advisor for their anesthesia board. She is also a certified healthcare auditor and has owned her own consulting company, Perfect Office Solutions, Inc., since November, 2001. She can be reached at  The Centers for Medicare & Medicaid Services (CMS) is pushing quality, the American Society of Anesthesiologists (ASA) is pushing the perioperative surgical home (PSH) and our 30-partner Pacific Valley Medical (anesthesiology) Group (PVMG) in Pasadena, CA is picking up both causes. In our commitment to a PSH clinic staffed and managed by anesthesiologists, we are fully embracing the concept of transitional care & perioperative medicine. This is our contribution to our patients and to our Huntington Memorial Hospital’s (HMH) Readmission Reduction Program.
The Centers for Medicare & Medicaid Services (CMS) is pushing quality, the American Society of Anesthesiologists (ASA) is pushing the perioperative surgical home (PSH) and our 30-partner Pacific Valley Medical (anesthesiology) Group (PVMG) in Pasadena, CA is picking up both causes. In our commitment to a PSH clinic staffed and managed by anesthesiologists, we are fully embracing the concept of transitional care & perioperative medicine. This is our contribution to our patients and to our Huntington Memorial Hospital’s (HMH) Readmission Reduction Program. As a physical presence, the PSH is necessarily a location with staff and support from the hospital. It is a substantial investment of both finances and administrative effort in managing 11,000 patients more effectively. Currently, the majority of those elective patients present to the hospital and the pre-operative holding suites the morning of surgery. You can imagine the resulting cancellations and delays that result from last-minute pre-op work that could have been done weeks before the very day of surgery. This patient and information flow is no longer acceptable. It wastes resources and it exposes patients to sub-optimal outcomes. Huntington Memorial is already in process of expanding the physical capacity of this clinic to accommodate all the surgical patents. This physical facility and support staff are the hospital’s investment.
As a physical presence, the PSH is necessarily a location with staff and support from the hospital. It is a substantial investment of both finances and administrative effort in managing 11,000 patients more effectively. Currently, the majority of those elective patients present to the hospital and the pre-operative holding suites the morning of surgery. You can imagine the resulting cancellations and delays that result from last-minute pre-op work that could have been done weeks before the very day of surgery. This patient and information flow is no longer acceptable. It wastes resources and it exposes patients to sub-optimal outcomes. Huntington Memorial is already in process of expanding the physical capacity of this clinic to accommodate all the surgical patents. This physical facility and support staff are the hospital’s investment. In response, and to our Huntington Memorial C-suite’s great credit, their explicit #1 priority was to improve the patient experience and surgical outcomes. They elaborated their faith in our PVMG anesthesia group as a worthy partner. Demonstrating intuitive understanding of the PSH, the CEO, the CFO and the VP of Quality found this project a worthy investment of their administrative energies and hospital finances. Our C-suite administrators then asked by what means they could facilitate the project.
In response, and to our Huntington Memorial C-suite’s great credit, their explicit #1 priority was to improve the patient experience and surgical outcomes. They elaborated their faith in our PVMG anesthesia group as a worthy partner. Demonstrating intuitive understanding of the PSH, the CEO, the CFO and the VP of Quality found this project a worthy investment of their administrative energies and hospital finances. Our C-suite administrators then asked by what means they could facilitate the project. Rick Bushnell, MD, MBA is the Director of the Department of Anesthesia, Shriners Hospital for Children, Los Angeles, CA and a Clinical Anesthesiologist at Huntington Memorial Hospital in Pasadena, CA. Dr. Bushnell graduated from the University of Illinois College Of Medicine and attended the University of Pittsburgh Medical Center, Pittsburgh and Loma Linda University for internship and residency. He has been with Pacific Valley Medical Group since 2003 and consults with Shriners Hospital for Children, Los Angeles. He and his partner have six adopted children in Tanzania where he serves as Visiting Clinical Anethesiologist at St. Elizabeth’s Hospital for the Poor in Arusha. He can be reached at
Rick Bushnell, MD, MBA is the Director of the Department of Anesthesia, Shriners Hospital for Children, Los Angeles, CA and a Clinical Anesthesiologist at Huntington Memorial Hospital in Pasadena, CA. Dr. Bushnell graduated from the University of Illinois College Of Medicine and attended the University of Pittsburgh Medical Center, Pittsburgh and Loma Linda University for internship and residency. He has been with Pacific Valley Medical Group since 2003 and consults with Shriners Hospital for Children, Los Angeles. He and his partner have six adopted children in Tanzania where he serves as Visiting Clinical Anethesiologist at St. Elizabeth’s Hospital for the Poor in Arusha. He can be reached at  This shift necessarily involves not only entry into new employment arrangements but also the termination of existing relationships. And those terminations are often governed by written employment agreements, state and federal healthcare laws and employer benefit plans and other policies and procedures.
This shift necessarily involves not only entry into new employment arrangements but also the termination of existing relationships. And those terminations are often governed by written employment agreements, state and federal healthcare laws and employer benefit plans and other policies and procedures. Kathryn (Kate) Hickner, Esq. is an attorney at Ulmer & Berne LLP, where she co-chairs the firm’s Health Care Practice Group. Additional information regarding Kate’s background, experience, publications and presentations can be found at
Kathryn (Kate) Hickner, Esq. is an attorney at Ulmer & Berne LLP, where she co-chairs the firm’s Health Care Practice Group. Additional information regarding Kate’s background, experience, publications and presentations can be found at  the group they are leaving and also by federal and state laws regarding employer benefit
the group they are leaving and also by federal and state laws regarding employer benefit
 Neda M. Ryan, Esq. is a Corporate Compliance Attorney for ABC. Ms. Ryan has experience in all areas of healthcare law, including healthcare transactional and corporate matters; healthcare litigation matters; providing counsel regarding compliance and reimbursement matters; and third party payer audit appeals. She can be reached at (517) 787-7432 or at
Neda M. Ryan, Esq. is a Corporate Compliance Attorney for ABC. Ms. Ryan has experience in all areas of healthcare law, including healthcare transactional and corporate matters; healthcare litigation matters; providing counsel regarding compliance and reimbursement matters; and third party payer audit appeals. She can be reached at (517) 787-7432 or at