eAlerts
-
Pre-Op Your Anesthesia Practice
Howard Greenfield, MD,
Founder and Principal, Enhance Perioperative & Anesthesia Consulting, Aventura, FL
Anesthesiologists routinely perform a “pre-operative” assessment of a patient scheduled to undergo an invasive procedure that requires anesthesia services. This assessment is a standard of care that has benefits that are guided by the provider’s intention to limit surprises. No physician wants to be in the middle of a complex surgical case and first find out about an underlying chronic condition that has deleterious effects on the patient. It is our observation that more anesthesia groups than ever are about to undergo the business equivalent of an invasive procedure. Shouldn’t you apply the same standard to your own practice, and find out how your group will look to a possible partner, investor or employer before your group is in the middle of negotiations with another entity? The radically changing healthcare world will confront all hospital-based anesthesia group practices with complex and difficult choices. Do you stay the course and try to postpone the inevitable, or pursue alternatives to the status quo? Either way, aren’t you better off mitigating the surprise factor now, rather than in the middle of a group take-over, merger, sale or offer of hospital employment?
There is no best single answer to any of the questions above. In fact, each option brings many additional questions to the forefront. One of the most important first steps is to perform a SWOT analysis (Strengths, Weakness, Opportunities, Threat) of your group. What are your group’s strengths and weakness? Do you have hospital contracts, and how secure are they? Are there opportunities, such as partnering with other similarlysituated groups? What are the real versus imagined threats? For example, is your hospital really interested in forcing employment on your group or is the hospital just tired of dealing with difficult members of your group? Where are your threats coming from, and do you have the ability to recognize them from the inside? Many small- to medium-sized groups are worried about the larger anesthesia group across town and fail to realize that the more likely threat comes from within their own hospital system. With hospital margins rapidly decreasing, hospital administrators are looking for different ways to minimize the physician spend at their facility.
In the past, a good anesthesia group providing quality services at the lowest possible cost would not have to worry that a competitor could underprice them without reducing services. That is no longer true, as more entrepreneurial physician organizations have a menu of hospital-based specialties to offer: Emergency, Radiology, Intensivists, etc. The opportunity for such a group is to use the substantial profitability of the other hospital-based services to “pay down” the anesthesia subsidy. This type of marketing has opened a whole new world of competitive bidding. These same large multi-specialty groups often have geographic leverage with payers and favorable national contracts to substantially increase anesthesia revenue and decrease the subsidy for their hospital customers.
In order to decide which route may be best for your group, let’s go back to the common starting place where all anesthesiologists begin patient care—the anesthesia pre-op assessment.
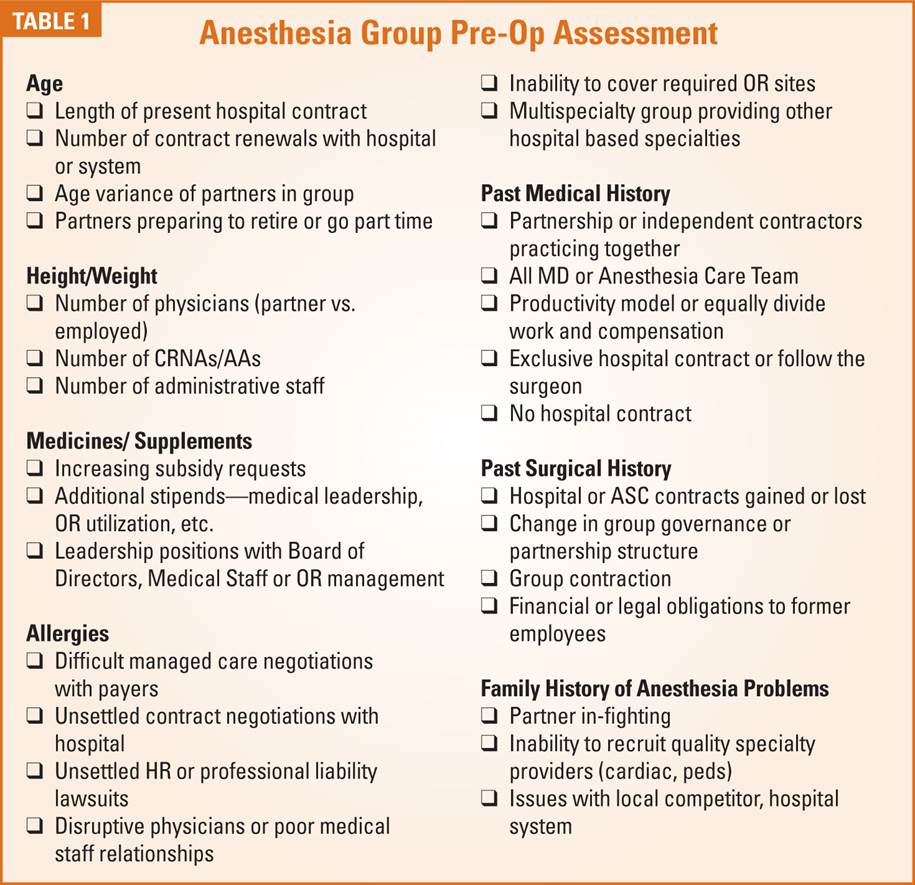
As you fill out your Anesthesia Pre-op Assessment sheet, remember to check the boxes that best describe your present anesthesia practice. (See Table 1 on page 4). Truthful answers to these questions will help you determine your anesthesia group’s ASA status—its Ability to Sell to Another. This is equally important in retaining your present contract or marketing your group to a hospital system, individual facility, national buyer or regional partner.
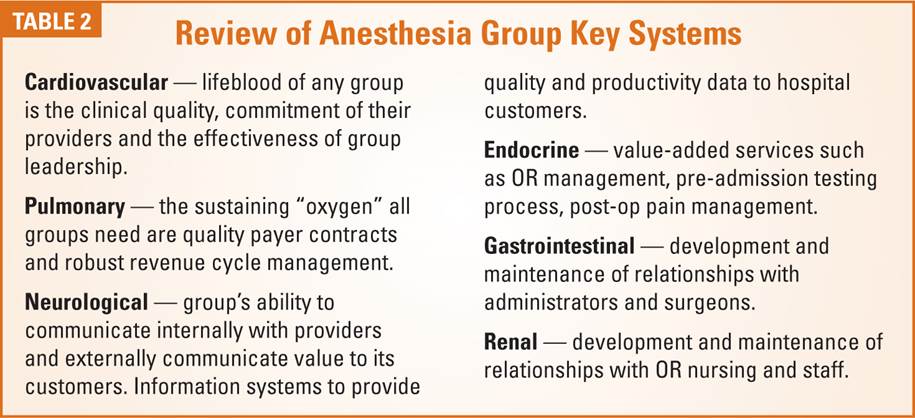
In the typical anesthesia pre-op process, the review of systems follows the collection of pertinent patient data and past medical and surgical history. As you begin to review your own group, it is important to look at and determine how well the key systems are functioning in your practice. (See Table 2). In many cases groups will need to bring in outside consultants to help them thoroughly evaluate a particular system.
At this point a simple question to pose to your group is, “If our practice sold shares to investors, with a promise of return on that investment, would you buy additional shares of our own practice?” Whatever the initial reply to that question, isn’t it incumbent on the partners or owners to determine “pre-operatively” what value the practice may have before potential investors or employers are about to “operate”?
Howard Greenfield, MD is a board-certified anesthesiologist and graduate of Temple University School of Medicine with anesthesia training at Jackson Memorial/University of Miami. He is an experienced clinician, and has served as Chief of Anesthesia at Memorial Regional Hospital. He became one of the original founding partners of Sheridan Healthcare. Greenfield later went on to found Enhance Healthcare with Dr. Robert Stiefel. Together, they have extensive national experience helping hospitals and anesthesia groups structure and negotiate anesthesia service agreements, optimize the revenue cycle, and implement operating room improvement initiatives. Enhance Healthcare partners are actively involved in the anesthesia merger and acquisition space. They have advised a number of anesthesia practices on strategic alternatives, and have worked with investment banking and private equity to help complete a number of group transactions. Dr. Greenfield can be reached at hgreenfield@enhancehc.com. -
Management Service Organizations and Anesthesia Practices Today and in the Future
William Hass, MD, MBA
Co-Founder, PhySynergy, LLC, Huntsville, ALManagement Service Organizations (MSOs) will have an increasingly important role in anesthesia practices. What today are cooperatives of independent anesthesia groups may morph into something quite different in the future.
The original goal of an MSO was to be a cooperative of local independent anesthesia services that reduced costs and gained management expertise for its members. The desired functions and advantages were similar to those offered by cooperatives in other industries. Traditional and attainable goals to be sure, but then reality got involved.
Here’s one version of reality. Some anesthesia groups and anesthesia professionals are concerned (read terrified) that the “sharks” of the anesthesia business world, anesthesia management companies (AMCs) and private equity investors (PEIs), will devour local practices. The facts behind this assumed reality are quite different than imagined; more people die each year from being crushed by vending machines than from shark bites. Here’s another reality. Many more anesthesia practices will perish due to their poor governance, leadership, management and human resource management (HRM) than will be gobbled up by AMCs and PEIs.
If the risks from AMCs and PEIs are small, why should a local independent anesthesia group worry? Why do anything? It’s another, but different, reality this time. The probability of an anesthesia service having insight into its strengths and weaknesses is about as common as a shark attack. Many anesthesia services not only don’t know where they are headed, they don’t have a clue where they are. Are they:
- A success to be sustained,
- In need of organizational “tweaking” for realignment,
- Doomed without an extensive turn-around,
- A candidate to be restarted, or
- A sucking black hole of resources and careers?
They don’t know. Worse, the conventional wisdom inside anesthesia groups is that they are above average. Just ask them.
There are anesthesia groups that are well led and well managed. They can make decisions and prosper. They see the future and see the possibilities. There is also a vast wasteland of dead, dying, lost and confused anesthesia services. Sort of sounds like the definition of zombies, doesn’t it? In you’re waiting for them to make a decision, particularly a difficult business decision, you are wasting your time. The chances of that happening are less than that of a shark attack in a vending machine.
Why? Failed governance is the costly, and possibly lethal, flaw in many anesthesia services. Decisions are just about impossible to make given voting requirements in their operating agreements or the realities of their day-to-day functioning. Veto power maybe given to a minority of members more interested in preserving their prerogatives than in making difficult and/or uncomfortable decisions. Senior members may seek short-term solutions that are not in the best long-term interests of their junior associates, allied anesthesia professionals or the facilities they serve. Not only do these groups not know who they are or what their problems are, they can’t do anything to fix their situation. This is a case of suicide by failed governance.
This presents a significant problem for governing boards and facility administrators. If they:
- Can’t depend on the local group to make a decision,
- Don’t want the complications of an employed anesthesia service,
- Want to avoid the entanglements of an AMC compounded by the complexities of PEI involvement.
What should the facility leadership do? The best possible answer is to engage an MSO to transition their existing zombie anesthesia service into one that can provide long-term clinical excellence and community service, as well as the operational and financial performance needed for the future.
How does this work? Simply, the facility will enter into a “caretaker” contract for anesthesia services with an MSO to:
- Evaluate services needed and provided,
- Reorganize clinical, operational and financial operations, and
- Return the anesthesia service to local independent owners.
The newly-reorganized and revitalized local independent group and its staff will become new independent members of the MSO in order to continue low costs, proactive management and the valuable association with other successful groups.
At this point anesthesiologists and other anesthesia professionals might cry foul. Aren’t MSOs dealing with the enemy when they work with governing boards and administrators? With rare exception, anesthesiologists will be business partners with governing boards and facility administrators for their entire career. Reality again. Neither party can succeed without the other over the long term. When a governing board works with a MSO, the goal is to develop a local independent anesthesia service so that neither party is subject to the whims of distant AMC corporations or PEIs. The goal of the local facility-MSO relationship is to direct the resources of the practice to the local community, not the operating costs and profit of distant corporations or investors.
It is possible that governing boards and management would cry foul too. The concept of working constructively with anesthesiologists might seem so foreign that the whole idea is more like science fiction than a reasonable alternative. So what are the alternatives? Doing nothing doesn’t seem like a viable plan in today’s environment. The problems with employment are becoming increasingly apparent. Becoming an ATM for an AMC and their PEI investor doesn’t seem like a good idea, either. MSOs provide the greatest potential for the best possible operational and financial performance at the lowest possible—and sustainable—cost.
There is a significant potential that MSOs will go be beyond being cooperatives of member anesthesia groups to actually developing new MSO member groups. Using caretaker contracts, these MSOs will steward troubled anesthesia groups though the process of becoming successful local independent anesthesia services. While voluntary membership in an MSO is preferred, given flaws in many groups’ decision-making, this transition may eventually be led by governing boards, administrators and managers who understand the operationaloperational and financial benefits of local and independent practices. Building on strong relationships with facilities, MSOs may provide a full range of medical services including hospitalists and other hospital-based services. This is happening already.
Why will MSOs succeed? Because there is strength in cooperative and collaborative efforts based on mutually advantageous local relationships. In fairness it should be noted that there are well-led and well-managed AMCs, but their business model gets in the way. If you rob Peter to pay Paul long enough, Peter is going to figure that there is something wrong with the relationship and that there must be a better way.
For a proactive physician group, facility or multi-site corporation, an MSO is the best choice now and in the future. If your organization is better served by being subject to the whims and entanglements of management companies and their investors, that’s your decision to make. If you feel that your organization’s financial resources can be better used supporting the operating expenses and investor expectations of other companies, that too is your decision to make. Just know that MSOs will be around to pick up the pieces long after your bad choices are gone.
William Hass, MD, MBA has been actively involved in anesthesia practice management for more than thirty years. He currently is the medical service organization (MSO) evangelist for PhySynergy, an MSO based in Huntsville, Alabama. PhySynegry executives had more than 100 years cumulative service in anesthesia service management. Dr. Hass is also the medical director for the Madison Surgery Center in Madison, Alabama. He can be reached at whhass@physynergy.com. -
Reporting Critical Care Services
Joette Derricks, CPC, CHC, CMPE, CSSGB
Vice President of Regulatory Affairs & Research, ABCAnesthesiologists are uniquely qualified to coordinate the care of patients in the intensive care unit because of their extensive training in clinical physiology/pharmacology and resuscitation. Some anesthesiologists pursue advanced fellowship training to subspecialize in critical care medicine in both adult and pediatric hospitals. In the intensive care unit, they direct the complete medical care for the sickest patients. The role of the anesthesiologist in this setting includes the provision of medical assessment and diagnosis, respiratory and cardiovascular support and infection control. Clinical competence and expertise in meeting the needs of a critically ill or injured patient unfortunately does not automatically transfer to payer’s documentation and coding requirements. The following article reviews the critical care services documentation, coding and billing guidelines.
* * *
The American Medical Association’s Current Procedural Terminology® (CPT) Codebook defines critical care as the direct delivery by a physician(s) or other qualified health care professional of medical care for a critically ill or critically injured patient. A critical illness or injury “acutely impairs one or more vital organ systems such that there is a high probability of imminent or life threatening deterioration in the patient’s condition”.
Critical care involves high complexity decision making to assess, manipulate and support vital system functions(s) to treat single or multiple vital organ failure and/or the prevention of further life threatening deterioration in a patient’s condition. Examples of vital organ system failure include, but are not limited to: central nervous system failure, circulatory failure, shock, renal, hepatic, metabolic and/or respiratory failure.
Delivering critical care in a moment of crisis, or upon being called to the patient’s bedside emergently, is not the only requirement for providing critical care service. Treatment and management of a patient’s condition in threatening imminent deterioration, while not necessarily emergent, is also required.
The presence of a patient in an Intensive Care Unit (ICU) or Critical Care Unit (CCU), or the patient’s use of a ventilator, is not sufficient to warrant billing critical care services. The service must be medically necessary and meet the definition of critical care. Medically reasonable and necessary services that do not meet all the criteria to report critical care should be reported with the appropriate evaluation and management code (e.g., CPT codes 99231-99233).
Since critical care is a time-based service, the physician’s critical care note(s) must document the total time spent evaluating, managing and providing critical care services to a critically ill or injured patient. Critical care time may be continuous or intermittent in aggregated time increments. Time spent performing other, separately billable procedures/services cannot be used to support critical care time.
The time spent providing critical care services must be at the immediate bedside or elsewhere on the floor or unit as long as the physician is immediately available to the patient. Therefore, the physician cannot provide services to any other patient during the same period of time.
In the teaching environment, the teaching physician must be present for the entire period of time for which the claim is submitted. Time spent teaching may not be counted towards critical care time. Teaching physicians, in addition, cannot bill for time spent by the resident providing critical care services in their absence. Only time that the teaching physician spends with the patient, or that he or she and the resident spend together with the patient, can be counted toward critical care time. Provided that all requirements for critical care services are met, the teaching physician’s documentation may tie into the resident’s documentation. The teaching physician may refer to the resident’s documentation for specific patient history, physical findings and medical assessment. However, it is the teaching physician’s stand-alone documentation that determines whether a critical care service can be billed.
The teaching physician medical record documentation must provide information including the time the teaching physician spent providing critical care; that the patient was critically ill during the time the teaching physician saw the patient; what made the patient critically ill; and the nature of the treatment and management provided by the teaching physician.
The following is an example of acceptable teaching physician documentation:
Patient seen and examined with Dr. Resident. Reviewed and agree with his note and the plan of care we developed together. One hour of critical care time personally performed due to patient’s hemo-dynamic instability. Patient was resuscitated with 2 units of packed red blood cells. Additional studies were obtained to determine possible causes for patient’s instabilities.
In 2014, the CPT Codebook lists the following services as included in critical care services and provides that they should not be reported separately: the interpretation of cardiac output measurements (93561, 93562), chest x-rays (71010, 71015, 71020), blood draw for specimen (36415), blood gases and information data stored in computers (e.g., ECGs, blood pressures, hematologic data) (99090), gastric intubations (43752, 91105), pulse oximetry (94760, 94761, 94762), temporary transcutaneous pacing (92953), ventilator management (94002-94004, 94660, 94662), and vascular access procedures (36000, 36410, 36415, 36591, 36600).
Time involved performing procedures that are not bundled into critical care (i.e., billed and paid separately) may not be included and counted toward critical care time. The physician’s progress note(s) in the medical record should document that time involved in the performance of separately billable procedures was not counted toward critical care time. For example, an emergency intubation may be billed separately as 31500 if supported by the documentation and the time is excluded from critical care time if both are being reported. What services are and are not bundled into critical care change from time to time and physicians along with their billing staff should review the list each January.
Routine daily updates to family members are considered part of critical care services and not separately billable. However, time spent with family member or other surrogate decision makers may be counted toward critical care time when these criteria are met:
- The patient is unable or clinically incompetent to participate in giving a history and/or decision making and
- The discussion is necessary for determining treatment decisions.
A summary of any family discussion is to be documented within the medical record and should show that the patient was unable or incompetent to participate as well as the necessity for the discussion and any treatment decisions made.
Telephone calls to family members and/or surrogate decision makers may be counted provided that they meet the same criteria as described above. All other family discussions, no matter how lengthy, may not be counted towards critical care time.
Critical Care Services Codes
- Code 99291 (critical care, first hour) is used to report the services of a physician providing constant attention to a critically ill patient for a total of 30 to 74 minutes on a given day.
- Only one unit of code 99291 may be billed by a physician for a patient on a given date.
- If the total duration of critical care provided by the physician on a given day is less than 30 minutes, the appropriate evaluation and management code should be used. In the hospital setting, it is expected that the Level 3 subsequent hospital care code 99233 would most often be used.
- Code 99292 (critical care, each additional 30 minutes) is used to report the services of a physician providing constant attention to the critically ill patient for 16 to 30 minutes beyond the first 74 minutes of critical care on a given day.
- The following illustrates the correct reporting of critical care services:
Total Duration of Critical Care Code(s)
Less than 30 minutes 99232 or 99233 30-74 minutes 99291 x 1 75-104 minutes 99291 x 1 and 99292 x 1 105-134 minutes 99291 x 1 and 99292 x 2 135-164 minutes 99291 x 1 and 99292 x 3 Important Coding Requirements
- Only one physician may bill for critical care services during any one single period of time even if more than one physician is providing care to a critically ill/injured patient. Documentation in the patient’s medical record must support the specific time that the physician was present at bedside or engaged in work directly related to the individual patient.
- Physicians assigned to a critical care unit (hospitalist/intensivist) may not report critical care based on a “per shift” basis.
- Claims for seemingly improbable amounts of critical care on the same date are subjected to review to determine if the physician has filed a false claim.
- Services cannot be reported as a split/shared service when performed by a physician and a nonphysician provider (NPP) in the same or another group practice.
- Physicians in the same group practice, with the same specialty, may not report 99291 for the same patient on the same calendar date. The initial critical care time, billed as CPT code 99291, must be met by a single physician or qualified NPP. This may be performed in a single period of time or be cumulative by the same physician or qualified NPP on the same calendar date.
- CPT Code 99292 (subsequent critical care visits) are for additional critical care time performed on the same calendar date. The service may represent aggregate time met by a single physician or physicians in the same group practice and in the same medical specialty in order to meet the duration of minutes required for CPT code 99292. The aggregated critical care visits must be medically necessary and each aggregated visit must meet the definition of critical care in order to combine the times.
- Concurrent care by more than one physician representing different specialties is payable if the services meet critical care requirements, (i.e., must be medically necessary and non-duplicative time and services.)
- Hospital emergency department services are not payable for the same date as critical care services when provided by the same physician or physicians of the same specialty.
- Critical care services will not be paid on the same calendar date that a physician reports an unbundled preoperative procedure with a global surgical period, unless the critical care is billed with modifier -25 to indicate that a significant, separately identifiable E/M service was performed. An ICD-9-CM code in the range 800.0 through 959.9 (except 930-939), which clearly indicates that the critical care was unrelated to the surgery, is acceptable documentation.
- Postoperative critical care may be paid in addition to a global fee if the patient is critically ill and requires the constant attendance of the physician, and the critical care is unrelated to the specific anatomic injury or general surgical procedure performed. In order for these services to be paid, two reporting requirements must be met. Codes 99291/99292 and modifier “-24” (Unrelated evaluation and management service by the same physician during a postoperative period) must be used, and documentation that the critical care was unrelated to the specific anatomic injury or general surgical procedure performed must be submitted. An ICD-9-CM code in the range 800.0 through 959.9 (except 930-939), which clearly indicates that the critical care was unrelated to the surgery, is acceptable documentation.
Resources
- AMA/CPT 2014 Critical Care Services
- http://www.cms.gov/Regulationsand-Guidance/Guidance/Manuals/Downloads/clm104c12.pdf, Section 30.6.12
- http://www.cms.gov/Regulationsand-Guidance/Guidance/Manuals/Downloads/clm104c12.pdf, section 100, Teaching Physician
Joette Derricks, CPC, CHC, CMPE, CSSGB serves as Vice President of Regulatory Affairs and Research for ABC. She has 30+ years of healthcare financial management and business experience. She is a member of MGMA, HCCA, AAPC and other associations and a regular speaker at practice management conferences. She can be reached at Joette.Derricks@AnesthesiaLLC.com.
-
M&As Still Going Strong: Position Your Anesthesia Practice
Analogies make us stop and think. Sonya Pease, MD, chief medical officer of TeamHealth, invites us to consider that customers of service industries such as restaurants reward outcomes rather than work processes in this Communiqué’s lead article, Working for Tips…. Much as patron satisfaction is key to success in the restaurant business, patient satisfaction is an outcome that physician compensation is going to reflect, whether we believe that patients are appropriate judges of quality medical care or not.
Patients’ perception of the caliber of the care they receive is determined in part by their doctors’ communication skills. Implementing multimodal pain and post-operative nausea and vomiting programs are very important, and so are the clinician’s self-introduction and expressed concern for the patient’s comfort. Think about the waiter’s keeping customers informed about delays and asking whether they need anything. These are skill sets most physicians “didn’t learn in residency but it is imperative we learn [them] and use [them] going forward,” as Dr. Pease writes.
The quality of the outcome in anesthesiology care depends, too, on the pre-operative work. Identifying and treating anemia before surgery, in Dr. Pease’s example, can have a “profound impact on patient outcomes as well as costs.” Analogously, solid preparation for the type of corporate restructuring of which we are seeing so much—take-overs, mergers, practice sales or offers of hospital employment—by identifying one’s group’s strengths and weaknesses is key to successful negotiations and reorganizations. In Pre-Op Your Anesthesia Practice, Howard Greenfield, MD of Enhance Healthcare provides a practical checklist for an anesthesia group “preoperative assessment” with such familiar categories as “age” (e.g., length of hospital contract), “height/weight” (e.g., number of MDs/CRNAs/AAs) and “past surgical history” (e.g., change in group governance), as well as a “review of systems” in which “neurological” encompasses the “group’s ability to communicate internally … and externally….”
A fundamental question in the pre-op assessment of a practice is its net worth. Mark Weiss, Esq. explains succinctly that an anesthesia practice is worth exactly as much or as little as a willing buyer will pay—and how its value may differ according to the perspectives of the senior and junior anesthesiologists who are considering selling.
There are still many alternatives to a sale or acquisition, Mr. Weiss reminds us in What’s Your Anesthesia Group Worth? And Why It Might Not Make Any Difference. One of those involves forming or joining a management services organization (MSO), as discussed by self-styled MSO “evangelist” William Hass, MD, MBA in Management Service Organizations and Anesthesia Practices Today and in the Future. Another might focus on expanding The Role of Anesthesiologists in the Intensive Care Unit. Jody Locke reviews the requirements for realizing the potential of the ICU for anesthesia practices.
As always, we devote a portion of the Communiqué to reporting clinical services in compliance with the ever-evolving rules laid down by Medicare and other payers. Articles in this issue range from the general principles of good documentation described by Darlene Helmer in Improving the Documentation of Anesthesia Procedures to the very specific review of Field Avoidance and Special Positioning by Kelly Dennis. If you are involved in providing pain medicine or critical care services, you will also want to read the articles by Neda Ryan, Esq. and Joette Derricks.
We hope that all our readers are having a successful summer. We look forward to bringing you new information this fall.
With best wishes,
Tony Mira
President and CEO -
The Role of Anesthesiologists in the Intensive Care Unit
Jody Locke, MA
Vice President of Anesthesia and Pain Management Services, ABCFor all the time most anesthesiologists spend in the operating room and the Post-anesthesia Care Unit (PACU) there is a curious firewall when it comes to the Intensive Care Unit (ICU). Most anesthesia practices are actively pursuing ways to generate additional revenue and further strengthen their relationship to administration and yet rarely do such considerations include any discussion of the ICU. As a large national billing company with hundreds of clients across the country, we only bill for a few clients that cover the ICU. One might therefore ask, “Are these practices visionaries of a future reality or isolated exceptions?” What is the opportunity and what would be involved in exploring it? Why are the very physicians who promote themselves as ideal managers of the entire perioperative continuum not pursuing a more active role in the ICU? It would appear to be a logical and integral part of the Perioperative Surgical Home.
The scope of billable services for an intensive care unit is limited to specific intensive care service Current Procedural Terminology® (CPT) codes, (99291 and 99292), subsequent hospital visit codes (99231-99235) and a relatively short list of interventional modalities including the insertion of arterial lines, CVPs and Swan-Ganz catheters. In certain, limited situations there could also be an opportunity to bill for ventilator management. Anesthesiologists who provide anesthesia to cardiac patients must be careful in their use of these codes, however, because ventilator management is included in the scope of cardiac anesthesia.
The ICU codes are time-based. Code 99291 is intended to reflect an hour of management of a critically ill patient. As a practical matter, not all patient encounters last exactly 60 minutes and so CPT established a convention whereby the code can be used for any encounter lasting longer than 34 minutes or less than 74 minutes. The second code, 99292, is intended to reflect each subsequent half hour of care. Key to code selection is the acuity of care. Once patients are stabilized and no longer at significant risk, then subsequent hospital visit codes must be used. (For further information, see Joette Derricks’s article Reporting Critical Care Services on page 18.)
The economics of ICU coverage hinge on three factors: volume of patients, payor mix and the nature of the services provided. It is not uncommon for busy academic centers with multiple step-down units to have enough patients such that the typical provider will bill for 10 or more hours of care per day. Managing a small population of post-cardiac surgery patients, on the other hand, would not typically result in very significant billings. The impact of payor mix is the same as in the operating room where the Medicare payment rate of approximately $120 per hour is at the low end of the spectrum. This implies that 10 hours of billable time for a Medicare population would result in $1200. If even a few commercial PPO patients are included in the mix, the daily yield could approach that of the operating room. Given current levels of anesthesiologist compensation, most services must be subsidized by the facility.
As an outgrowth of the PACU, critical care units are now found in all major medical facilities throughout the United States. Anesthesiologists are uniquely qualified to coordinate the care of patients in the intensive care unit because of their extensive training in clinical physiology/pharmacology and resuscitation. Some anesthesiologists pursue advanced fellowship training to subspecialize in critical care medicine in both adult and pediatric hospitals. In the ICU, they direct the complete medical care for the sickest patients. The role of the anesthesiologist in this setting includes the provision of medical assessment and diagnosis, respiratory and cardiovascular support and infection control.
Anesthesiologists also possess the medical knowledge and technical expertise to deal with many emergency and trauma situations. They provide airway management, cardiac and pulmonary resuscitation, advanced life support and pain control, all of which are essential skills to the intensivist. As consultants, they play an active role in stabilizing and preparing the patient for emergency surgery.
The staffing requirements of ICUs may also create an opportunity for anesthesia practices. Given the level of activity and service provided it may be more cost-effective for anesthesia to rotate members of the group through the unit. This might also provide greater flexibility in staffing and coverage.
Lutheran General Hospital in Park Ridge, Illinois is a useful case study. Park Ridge Anesthesia has four intensive care-trained anesthesiologists who cover the ICU five days a week. The origin of the service goes back in time to a point where the hospital believed that its patients would be better served by a single service that could provide a continuum of care to patients undergoing major surgery. The assumption was that anesthesiologists who were familiar with the care received in the operating room would be better qualified to manage post-surgical complications in the ICU. The Park Ridge anesthesia team argues this has been the explanation for the consistently low levels of post-surgical complications and high levels of patient satisfaction.
Two common factors deter most anesthesia practices from any consideration of ICU coverage. The first is the revenue potential and the second is the politics of cardiac care. Because the reality of most intensive care services is that they are inherently unprofitable, they are not viewed as good opportunities for expansion in an era when Ambulatory Surgery Centers (ASCs) and endoscopy centers have tended to be such logical places to look for additional revenue potential. Why mine the unprofitable when the profitable is so readily at hand? Ironically, chronic pain management has become the next area of exploration, despite the fact that many chronic pain practices deliver such disappointing results. The underlying thread is the potential for independence. Rare is the practice that wants to build a practice model based on the need for subsidy from the facility. There may come a point, however, where all opportunities for independent, profitable expansion are exhausted.
If the primary focus of an intensive care service is post-cardiac surgical patients then this implies competition with the cardiologists who referred the patients to the facility for surgery in the first place. The cardiovascular surgeon makes his money performing complex surgical interventions, but the cardiologist makes his money managing patients over time. I have personal experience with a Long Island heart center that brought in an anesthesiologist to manage the ICU. In that case, it was a very profitable service, but the politics ultimately made it so challenging that the doctor left the facility.
There is also a curious chicken and egg phenomenon at work here, as indicated by the following abstract for an article in Anesthesia and Analgesia: The number of anesthesiology residents pursuing critical care medicine (CCM) fellowship training has been decreasing in recent years. A significant number of training positions remain unfilled each year. Possible causes of this decline were evaluated by surveying residents regarding their attitudes toward practice and training in CCM. All 38 anesthesiology programs having accredited CCM fellowships were surveyed. Four of these and one program without CCM fellowships were used to develop the survey instrument. Four programs without CCM fellowships and 34 programs with CCM fellowships make up the survey group. Returned were 640 surveys from 37 (97 percent) programs accounting for over 30 percent of the possible residents. Resident interest in pursuing CCM training decreased as year of residency increased (P < 0.0001). Residents in programs with little patient care responsibility during intensive care unit (ICU) rotations expressed less interest in CCM training (P < 0.012). The administrative role of the anesthesiology department in the ICU also influenced resident interest (P < 0.014). Written responses to open-ended questions suggested resident concerns with the following: stress of chronic care, financial consequences of additional year of training, ICU call frequency and load, ICU role ambiguity, and shared decision-making in the ICU. A recurring question was, “Are there jobs (outside of academics) for anesthesiologist intensivists?” Most residents knew a CCM anesthesiologist they admired and knew that there were unfilled fellowship positions available. Defining the job market, improving curriculum and teaching, supporting deferment of student loans, and introducing residents and medical students to the ICU earlier may increase the interest in CCM practice among anesthesiology residents (Anesthesia and Analgesia 1993).
With the changing focus of healthcare, is the ICU a clinical opportunity that anesthesia practices should be pursuing? Three factors would appear to support a revision of traditional thinking. If we assume that other opportunities for practice expansion are slowly drying up it might be time to revisit the potential of the ICU. As an increasing number of anesthesia practices receive stipends and other forms of financial support from facilities, there is a growing concern about justifying financial support. If anesthesia can expand its scope of services this could have distinct strategic advantages. An active role in the ICU is also logically indicated by the current focus on the Perioperative Surgical Home. In an era of customer service, hospitals love the concept of accountability for quality of care. Clearly a comprehensive service that includes co-management of the ICU with surgery has great potential to accomplish this.
As is true of so many other developments in healthcare, the real challenges to changing the practice model may be more educational and strategic than financial. Sometimes changing the culture of a facility is simply a matter of clearly delineating the advantages of a new approach. Some serious stakeholder analysis might reveal significant opportunities. It is all in the packaging.
Jody Locke, MA serves as Vice President of Pain and Anesthesia Management for ABC. Mr. Locke is responsible for the scope and focus of services provided to ABC’s largest clients. He is also responsible for oversight and management of the company’s pain management billing team. He will be a key executive contact for the group should it enter into a contract for services with ABC. He can be reached at Jody.Locke@AnesthesiaLLC.com.

 Howard Greenfield, MD is a board-certified anesthesiologist and graduate of Temple University School of Medicine with anesthesia training at Jackson Memorial/University of Miami. He is an experienced clinician, and has served as Chief of Anesthesia at Memorial Regional Hospital. He became one of the original founding partners of Sheridan Healthcare. Greenfield later went on to found Enhance Healthcare with Dr. Robert Stiefel. Together, they have extensive national experience helping hospitals and anesthesia groups structure and negotiate anesthesia service agreements, optimize the revenue cycle, and implement operating room improvement initiatives. Enhance Healthcare partners are actively involved in the anesthesia merger and acquisition space. They have advised a number of anesthesia practices on strategic alternatives, and have worked with investment banking and private equity to help complete a number of group transactions. Dr. Greenfield can be reached at
Howard Greenfield, MD is a board-certified anesthesiologist and graduate of Temple University School of Medicine with anesthesia training at Jackson Memorial/University of Miami. He is an experienced clinician, and has served as Chief of Anesthesia at Memorial Regional Hospital. He became one of the original founding partners of Sheridan Healthcare. Greenfield later went on to found Enhance Healthcare with Dr. Robert Stiefel. Together, they have extensive national experience helping hospitals and anesthesia groups structure and negotiate anesthesia service agreements, optimize the revenue cycle, and implement operating room improvement initiatives. Enhance Healthcare partners are actively involved in the anesthesia merger and acquisition space. They have advised a number of anesthesia practices on strategic alternatives, and have worked with investment banking and private equity to help complete a number of group transactions. Dr. Greenfield can be reached at 

 William Hass, MD, MBA has been actively involved in anesthesia practice management for more than thirty years. He currently is the medical service organization (MSO) evangelist for PhySynergy, an MSO based in Huntsville, Alabama. PhySynegry executives had more than 100 years cumulative service in anesthesia service management. Dr. Hass is also the medical director for the Madison Surgery Center in Madison, Alabama. He can be reached at
William Hass, MD, MBA has been actively involved in anesthesia practice management for more than thirty years. He currently is the medical service organization (MSO) evangelist for PhySynergy, an MSO based in Huntsville, Alabama. PhySynegry executives had more than 100 years cumulative service in anesthesia service management. Dr. Hass is also the medical director for the Madison Surgery Center in Madison, Alabama. He can be reached at