eAlerts
-
Independent Anesthesia Group Practice: A Short Manifesto
Will Latham, MBA
President, Latham Consulting Group, Inc., Chattanooga, TN“Most people will choose unhappiness over uncertainty. -Tim Ferris
 Anesthesia groups are facing great challenges in today’s environment. I am sure you are aware of these various challenges so I won’t belabor them.
Anesthesia groups are facing great challenges in today’s environment. I am sure you are aware of these various challenges so I won’t belabor them.The question is: What do we do now?
Some groups are throwing in the towel and selling out. It seems as though every few weeks another independent anesthesia group has sold out to one of the national companies. I wonder if they are “choosing unhappiness over uncertainty.”
But other groups continue to pursue independence. Why do they want to follow this path?
Benefits of Independence
Liberty – from the Latin libertas, meaning freedom of the people to participate rather than be ruled.
Over the past year I have worked with many anesthesia groups as they develop their strategic plans or negotiate mergers. One question that is often expressed by some group members is “why should we work so hard to stay independent? It feels like I am an employee already, so why don’t we go ahead and sell out?”
While this sentiment is typically expressed by those nearing the end of their careers (who are often attracted by the financial pay-off they will receive if the group is sold—money that they might not otherwise have received), sometimes younger physicians express the same thought.
Here are some of the key reasons that these groups are choosing to pursue independence:
- Elect your leaders: In an independent group, you get to decide how your governance system is structured and are able to vote on who will lead the group. As an employee you have no say in selecting group leaders (no matter what they tell you).
- Decide with whom you will practice: As an independent group, you get to decide who to add to your practice. As an employee, you don’t get to decide and may not even be asked for input.
- Retain control: As an independent group, you maintain control over the operation of the group, including such items as staffing levels, use of midlevels, scheduling, vacation, compensation p lans and retirement plans.
As an employee, you have a “boss,” and that individual has hiring and firing authority over you. If you are terminated, for whatever reason (even standing up to the employer for mistreating members of the group), don’t expect your associates to stand up for you. If they do so, they risk their position and have to go home and tell their spouse that they are moving. - Undiluted contact with the hospital: Hospital relationships are always challenging. As an independent group, you contract directly with your hospital (sometimes using external resources to help). You choose how much risk to take in these negotiations.
But if you are employed, someone else does much of the negotiating. Naturally, they don’t want to lose the contract or relationship, but if they do, what happens to you? You have to move, because that is what your noncompete agreement requires. - Protection from being arbitrarily fired: Most group shareholders are protected from being arbitrarily fired from their group. (Being fired typically requires a super-majority vote, which is sometimes a good thing and sometimes a bad thing.) If external organizations want a group member fired, the group ultimately makes the decision. As an employee, the “boss” makes that decision.
Many will take exception to these benefits of independent practice. But when you speak to such individuals, ask them how they make their money, and you will likely find that they make it by getting you to sell out. Almost everyone out there who offers advice on whether or not to sell your practice is incentivized for you to do the deal.Who is in Charge?
Some of the group members advocating selling out make the argument that “control is just an illusion—we are getting so big that I already feel like an employee of a big corporation—so why don’t we go ahead and sell out now?”
It is true that many groups are growing (and need to grow larger, as I discuss below). Growth typically results in the need for a more “corporate-like” atmosphere (more formal, more organized, more policies and procedures, etc.). However, I believe the real question is not “will we get more corporate-like?” but instead “who do you want to have at the top of the corporation?”
Who do you want on top:
- A hospital executive (whose goal is to appease the surgeons)?
- A “stock” executive (whose goal is to cash out)?
- Other physicians who you get to elect and who will more likely have your interests in mind at all times?
Independence Requires Work
Liberty means responsibility. That’s why most men dread it. – George Bernard Shaw
Making the decision whether or not to continue to be independent is an important first step. However, if your goal is to stay independent, there is work to be done. As the old saying goes, “even if you are on the right track you will get run over if you stand still.”
So, what are anesthesia groups doing to create more robust organizations? Here are some of the steps that we have seen anesthesia groups take to improve their prospects for the future:
- Improve governance: The most successful groups create a culture where all group members agree to support group decisions (or, if they don’t, are driven out of the organization) and then develop a governance system that:
- Creates a right-sized decision-making body
- Specifies the authority (hiring/firing, spending money, entering into contracts, deciding on key strategic issues) of each part of the governance structure
- Enhances group communication using multiple communication tools
- Develop strategic plans: Many anesthesia groups are now using a well-known business process called strategic planning to help them set their practice’s future direction. “Strategic planning” is a buzzword for a relatively straightforward process of defining the purpose of the group (why it exists), setting objectives (where it wants to go), and mapping a plan to meet those objectives (how it plans to get there). The most effective groups develop such plans and review and update them on an annual basis.
- Get bigger: In today’s healthcare market, bigger is often better in terms of providing cost-effective care and retaining autonomy. Single specialty mergers offer one of the few ways that anesthesia groups can “fight back” against a threatening environment. I believe that you can never be too rich, too thin or too big. Yes, growth will entail compromise and change, and you will have to give up some control in a larger group, but what’s the choice—employment? Circle the wagons and shoot out.
- Play politics: Plato is reported to have said “Those who are too smart to engage in politics are punished by being governed by those who are dumber.” Good works alone won’t protect you from threatening forces. This is why the most effective groups support their leaders with the time to be as fully involved with the hospital as possible.
- Pursue lucrative business: Some anesthesia groups get comfortable providing service at one location or in one system, even though having all the eggs in one basket puts them at great risk. Other groups receive substantial stipends that can put their hospital relationship at risk.
Anesthesia groups that are working to strengthen themselves for the future are actively looking for new business all the time, even if it is “inconvenient.” Such business is often in the form of ambulatory surgery centers which, if obtained, can improve the group’s payer mix, add staff to decrease call frequency and potentially reduce dependence on the hospital stipend. - “Simulate” the predators: Progressive anesthesia groups are paying attention to what predatory groups are doing (or say they are doing) so they can preemptively simulate their offerings. This does not mean the anesthesia group has to do everything the predatory groups are doing, but the group does have to show progress to hospital leadership to avoid the dreaded “request for proposal.”
- Deal with disruptive physicians: While this may seem to be a minor point as compared to the other initiatives outlined above, disruptive physicians create three enormous challenges for groups:
- Disruptive physicians threaten the entire group’s relationship with the hospital. Frankly, predatory groups do not allow this to happen and terminate or transfer disruptive physicians quickly.
- Disruptive physicians sap leadership time that could be spent on more valuable activities.
- Other members of the group become demoralized when they see that nothing is done to deal with disruptive physicians.
Therefore, the most effective groups have systems and processes to quickly and effectively deal with disruptive physician behavior. This could include creating a code of conduct by which the group can measure behavior, establishing an internal review process, and creating a formal process to deal with disruptive situations (see “Disrupting the Disruptive Physician” in the Winter 2018 issue of Communiqué).Time for Action
“Many a false step was made by standing still.” – Fortune Cookie
Is there a risk in staying independent? Of course there is.
However, look at the historical track record of companies that acquire medical practices. If you are too young to remember the acquisition activities of the 1990s, take a few minutes and Google such companies as PhyCor, MedPartners and OrthoLink.
To achieve the benefits of independence outlined above, it is time to move from worrying to working. Review these steps to determine what your group needs to work on to secure its future.
Will Latham, MBA, is president of Latham Consulting Group, Inc., which helps medical group physicians make decisions, resolve conflict and move forward. For more than 25 years Mr. Latham has assisted medical groups in the areas of strategy and planning, governance and organizational effectiveness, and mergers, alliances and networks. During this time he has facilitated over 900 meetings or retreats for medical groups; helped hundreds of medical groups develop strategic plans to guide their growth and development; helped over 130 medical groups improve their governance systems and change their compensation plans; and advised and facilitated the mergers of over 120 medical practices representing over 1,200 physicians. Mr. Latham has an MBA from the University of North Carolina in Charlotte. He is a frequent speaker at local, state, national and specialty-specific healthcare conferences. Mr. Latham can be reached at (704) 365-8889 or wlatham@lathamconsulting.com. -
Anesthesia Services RFPs: Reality, Unicorns and Cognitive Bias
Mark F. Weiss, JD
The Mark F. Weiss Law Firm, Dallas, TX, Los Angeles and Santa Barbara, CAThink back in time to a job interview. You dressed for success, put a wide smile on your face, and were on your best behavior.
In the advertising world, they call them “reviews.” In healthcare, we call them requests for proposal or “RFPs” for short. They’re the same thing.
If you’re the incumbent anesthesia group, your relationship with the hospital or other facility, including, if you have one, your exclusive contract, is at risk. There’s little doubt about it. If you’re an outside aspirant, there’s an opportunity to expand your business to an additional location. Or, no matter who you are, maybe you’re just being played.
As in the course of a job interview, in an RFP situation, everyone is on their best behavior. On all sides.
The hospital or ambulatory surgery center (ASC) is telling lies about how great it will be to provide services at the facility, and how supportive the administrators will be. And at the antipode, the outside aspirants for the exclusive contract are puffing about the quality of their anesthesiologists and CRNAs, and about what great service they’ll provide. And, like the administrators, their representatives will be wearing suits and ties and shiny shoes, just like on a job interview.
But the incumbent anesthesia group suffers from the maxim, “familiarity breeds contempt,” that is, from the fact that it is well known to the facility’s administrators and influential surgeons, warts and all.
Being not as well known, the aspirant anesthesia groups pitching their wares are all rainbows and unicorns, sugar and spice, with a snuggly puppy or two tossed in for good measure.
Let’s start with the truth: professional services are not, and cannot, be a commodity. But it’s also true that many have fooled themselves (or, more likely, others) into believing that they are. In fact, there’s an RFP industry ready to help.But, even if you’re a true believer in the commodity theory of healthcare, an RFP process for anything other than fixed items (such as for 3.72 million screws meeting Mil-Spec MS51861-1C) is a ridiculous way to make a decision. A way that exists only in a world in which those bureaucrats known as facility administrators are rewarded by visible, yet lazy, action, situated in a universe devoid of the knowledge that not taking visible action can be action just the same. A way in which decisions are made based on the lies that they’re told and the lies that they tell themselves.
Are these lies moral failings? Usually not. They’re generally more akin to resume embellishments, nicely pressed suits and shiny shoes. But either way, they’re a fiction, a phantasy and perhaps even fraud.
So what to do in the real world in which my thoughts about the craziness of the process have (unfortunately) little weight?
Everyone, from incumbent to aspirant to the consultant hired to “run” the RFP (and, who must assess the risk of doing so because there can be no truly effective indemnification from the facility), must assess the reality of the RFP against the three categories into which I divide them:
- True RFPs: These are genuine searches for the best-quality provider with a favorable ratio of quality to cost. This type of RFP is the closest in relationship to the traditional form used in industry and government. It is commonly seen in situations in which the current or sometimes very recently former group has “blown up” and can no longer provide coverage. It’s also frequent in scenarios where the current group has completely lost the facility’s trust.
- Fictitious RFPs: These RFPs belie the fact that hospital administrators are not interested in the merits of any response; they have already decided to whom they will award the contract. Yet, for one political reason or another, they’ve decided to issue a phony RFP to project a patina of “fairness” to the medical staff, to the hospital’s own board, to some third party—or perhaps to you.
- Fulcrum RFPs: Consider this the weaponized RFP. As the name implies, the increasingly common fulcrum RFPs are designed to create leverage. The facility intends to renew with the present group but uses the RFP as a tool to dictate terms by fiat and to pressure the group into negotiating against its own best interests out of fear of replacement. Nonetheless, the facility is open to competing proposals.
Although no outside assessment of category can be completely reliable, clues often abound. And category dictates strategy.If you’re the incumbent, you must have a strategy to avoid, deflect and defeat an RFP.
You must create an Experience Monopoly™1, not just perform in a service role. You must also develop a propaganda strategy, deployed over time, to educate and sway the administrators and to continuously garner the support of key influencers.
You must develop a true business that is broader than based simply on one hospital, so that you can negotiate from a place of strength. And you must have taken action to secure the cohesiveness of the group.
Is that enough to guarantee that there will never be an RFP, or that if there were one, you’d come out on top? No. There is no such guarantee anywhere. But those actions are required just the same or you’re wasting time, blowing the home team advantage (losing the headwind of confirmation bias on the part of the facility’s administration) and working against your own best interests.
Optimally, you need to have the ability to walk away, to say to the facility’s CEO, “no thanks, we won’t be submitting a proposal. But hey, good luck with that unicorn!” Developing the required structure takes time. It takes playing the long game. If you haven’t already started playing it, start today.
If you’re a hospital administrator reading a copy of Communiqué as background research for an RFP, remember what Richard Feynman, the famous physicist, said: people are easily fooled, and the easiest person to fool is yourself. Cognitive biases abound. And that unicorn may just be an ass wearing a fake horn.
If you’re on the outside looking at the opportunity that exists to expand your business to another facility, understand how to play to the administrators’ cognitive biases (e.g., “the existing group is dysfunctional,” and, for new CEOs, “you need to demonstrate leadership”). But be very careful about what you promise, because in the event that you “win,” you’ll actually have to deliver. It takes more effort to continue to play the unicorn after the audience knows it’s a trick.
Yes, you can count on a honeymoon period, again cognitive bias (it’s confirmation bias) on the part of the administration, but at some point your unicorn horn will fall off, you’ll be seen in the harsh light of reality, and, damn it, there’s probably a wart or two where that horn used to be.
Then, you’ll need to be on the lookout for yet another cognitive bias—buyer’s remorse. If it kicks in, know that the administrators are incapable of blaming themselves, so they’ll naturally have to blame you. Your only hope is that there’s some junior administrator to throw under the bus as a sacrifice to the hospital’s board. (In my experience, this is usually the CFO, but sometimes it’s a vice president.)
Whether you’re the incumbent or on the outside, if you “lose” the RFP, then, if you’ve developed the larger business that I advise is required, it might turn out to have been a win in disguise, for winning the race to the bottom is like a participation trophy at the local recreation center: it isn’t a real win.
And there’s also always a chance that you were defrauded in the course of the RFP, either by the facility or by the consultants brought in to stage the RFP process. Don’t want to be a direct party to the legal imbroglio? Then consider that, depending on the facts, “bid rigging” and misrepresentation in a fake or fraudulent RFP can lead to criminal prosecution under various state and federal laws.
1 An Experience Monopoly™ is the overall combination of the way that your group delivers services and the experience that you provide to the facilities, to the other members of the medical staff, to their patients and to the community at large, that creates a benefit that competitors, even if they understood what was being provided, would not be able to duplicate.
Mark F. Weiss, JD, is an attorney who specializes in the business and legal issues affecting physicians and physician groups on a national basis. He served as a clinical assistant professor of anesthesiology at USC Keck School of Medicine and practices with The Mark F. Weiss Law Firm, a firm with offices in Dallas, Texas and Los Angeles and Santa Barbara, California, representing clients across the country. He can be reached by email at markweiss@advisorylawgroup.com. -
Ambulatory Anesthesia: Everything You Wanted to Know But Were Afraid to Ask
Howard Greenfield, MD
Co-Founder and Principal, Enhance Healthcare Consulting, Aventura, FLJody Locke, MA
Vice President of Anesthesia and Pain Practice Management Services Anesthesia Business Consultants, LLC, Jackson, MI The steady migration of surgical cases from traditional inpatient to non-traditional outpatient and ambulatory venues has required anesthesiologists and CRNAs, the quintessential service providers, to continuously reinvent themselves to adapt to evolving market conditions and customer expectations. The assumptions and strategies that helped many anesthesia groups build successful partnerships with hospitals may no longer serve them well in today’s dynamic ambulatory environment.Today’s medical mantra is “value proposition.” Anesthesia providers are no longer being asked simply to provide safe and effective anesthesia care. They are also expected to create value for the facility. The ability to generate this value requires close collaboration with the facility’s leadership, staff and surgeons.
If there is one overarching distinction between traditional hospital agreements and ambulatory agreements, it is the availability of subsidy money. While most hospitals are willing to provide financial support for unprofitable business lines, this is rarely, if ever, the case in the ambulatory environment. This reality of ambulatory anesthesia means that the anesthesia practice must make sure the arrangement with an ambulatory surgery center (ASC) makes financial sense before proceeding.
Is it time for anesthesia practices to evaluate and pursue ambulatory opportunities? The answer is yes, but caveat emptor: buyer beware. Never has it been so important to exercise rigorous due diligence and to objectively evaluate the potential benefits and risks. In the past, relationships with most ambulatory facilities would only enhance an anesthesia practice. This is no longer the case. The three rules of success are: 1) know what you are getting yourself into; 2) make sure the numbers make sense; and 3) monitor performance closely and continuously.
Types of Ambulatory Practices
While we tend to think of ambulatory anesthesia as a generic term, the fact is that no two ambulatory facilities—and therefore, no two ambulatory anesthesia agreements—are the same. To understand the challenges and opportunities associated with this new anesthesia frontier, it is useful to think in terms of five subsets of facilities and types of cases. These categories offer a framework for the key financial and strategic issues that anesthesia practices should consider before signing an agreement with a new facility:
- Hospital-owned outpatient facilities that are physically part of the hospital campus, billed with a place of service code -22;
- Freestanding ASCs that represent a joint venture between a hospital and surgeons, billed with a place of service -24 modifier;
- Surgeon-owned freestanding ASCs, also billed with a -24 modifier, but which may have different financial objectives than the hospital joint venture facilities;
- Single specialty centers, such as an endoscopy center, an eye center or a center for reproductive medicine, billed with a -24 modifier;
- A doctor’s office, billed with a place of service -11 modifier. Anesthesia provider to be asked to cover dental or plastic surgeons’ offices.
A Range of Realities
The challenges of successful anesthesia practice management in any of these types of facilities can be significant. The fact that ambulatory cases are shorter, of lower acuity and turn over faster may seem advantageous, but these characteristics create an entirely different set of customer expectations than those in hospital operating rooms (ORs). To understand this difference, think of email and texting. When people talked on the phone and sent documents by mail or messenger there was no expectation that things would happen instantly. The advent of texting and email has created an expectation of an instant response. Today’s well-run surgery center epitomizes the application of business principles to medicine, where the real measure of success is customer service, efficiency and profitability.
Smaller facilities with smaller staffs tend to require and encourage a collaborative approach to care delivery. Some anesthesiologists and CRNAs perform better than others in an environment where efficiency and throughput are a primary objective. These high-velocity facilities require high-velocity providers. Anesthesia practices will find that only a select subset of anesthesiologists and CRNAs work well in such settings. This is the place for skilled providers with proficiency in regional anesthesia and acute pain techniques. Contracts can easily be lost because of incompatible staff assignments.
Beyond these staffing considerations, the anesthesia practice must also deal with the economic realities of an ambulatory environment. Logistics and resource deployment can be far more challenging, especially if the practice covers multiple outpatient facilities in addition to its primary hospital. In the main hospital OR, a team of providers can be assigned to cases as needed, with an expectation that, on average, there are enough cases or subsidy to cover staff costs.
This is not the case with outpatient and ambulatory facilities, especially if they need anesthesia only a few days a week or if anesthesia is needed for only a few cases per day. Large practices with multiple outpatient relationships often create a separate scheduling function to ensure that their providers meet their obligations at the various facilities in a timely manner. The economics of ambulatory anesthesia are not always as favorable as one might expect. Practices often focus on general production data that does not allow the practice to compare business lines or assess their profitability. Standard billing reports that simply show basic anesthesia values such as cases, units, charges and payments by month—even if they include a breakdown by facility—will never be adequate to manage an expanding and dynamic book of ambulatory business.Numbers Tell the Story
The use of normalized data is essential for understanding each ambulatory setting’s value to the practice as a whole. The fact that collections at one facility are twice as high as at another says nothing about their real value. As any manager responsible for multiple business lines will attest, business lines must be compared using the same criteria and benchmarks. This consistency is especially important in practice management in anesthesia. There is discussion in the field about which type of normalized metric is most useful. We will discuss common examples and weigh their value, including yield per unit, yield per hour and yield per provider day.
Table 1 provides a high-level example. The table shows data for 766 ABC client ambulatory facilities across the country for calendar year 2017. The first two metrics—units per case and yield per unit—are the revenue drivers that determine the next three metrics. Yield per hour can be a useful comparative metric if the objective is to compare business lines. However, many find the last two metrics of most value in assessing a coverage agreement’s potential profitability. Based on this sample, only two types of facilities cover the cost of a physician anesthesiologist.
There are three main challenges in ASC staffing:
- The number of days per week that coverage is required. While it can be advantageous if a facility generates a few extra cases that can be done during down time, often these cases are performed during peak morning times, which means extra resources are needed for additional morning starts.
- The consistency of production. An anesthesia practice needs a guarantee of revenue to cover manpower costs. Unpredictable weekly coverage and daily swings in case volumes create a potentially risky situation.
- The average yield per clinical provider day. Production metrics must be calculated as averages over time. A few profitable days does not make for a profitable relationship.
As indicated in Chart 2, most physician- only practices find it difficult to profitably staff ambulatory facilities. The cost of a physician-only practice in the current environment is simply too high, at $2,100 per provider day. Even if the average cost can be driven down to $1,700 or $1,800 with the use of a care team model, that is still higher than the average value of $1,540 shown in Table 1. There may be offsetting strategic or tactical reasons to incur such a loss, but it is still a loss.
Making the Most of a Good Thing
Given all these challenges, then, what is the upside? The difference between a profitable arrangement and an unprofitable one hangs on three key factors: consistency of production, consistency of collections and cost of providing the requested coverage.
Consistency of Production
A practice cannot manage what it does not measure. For example, consider production consistency. In an ambulatory environment this metric should be monitored by day. Chart 1 provides a typical example. Typically, an anesthesia practice staffs for a daily number of 7:30 am starts, meaning that first-case starts determine the staffing needed for the facility. The hope and the assumption are that sufficient activity in the OR will cover the cost of the providers. While this is not always the case in the hospital, it is definitely not always the case in the ambulatory environment. The smaller the facility, the greater the challenge.
Consistency of Collections
Billed ASA units are the most useful production metric in anesthesia. Conventional wisdom holds that an optimally run hospital OR suite should consistently generate 50 billed units per location day. Table 3 represents actual production data based on date of service (DOS) for January, 2018 for a randomly selected ABC client facility. Note that most rooms do not meet the target threshold.
Cost of Providing Coverage
For this reason, it is useful to monitor actual collections per provider location day (see Table 2). While Chart 1 may bear a striking resemblance to Chart 2, the financial scale of the data makes it far more relevant to the management of the practice. The target here is based on the daily provider cost of a physicianonly practice. If we assume that the total burdened cost (base compensation plus overhead and benefits) is $490,000 and that the physician works 231 days a year, then the cost would be $2,100 per physician day. This number might be high for some practices and some parts of the country. Actual target yields will vary based on region. Practices applying this analysis are advised to use actual data.
What value does this information have for a practice? If specific business lines are underperforming, the practice has three choices:
- Accept the loss for broader strategic reasons.
- Identify opportunities to increase revenue. Subsidies are rarely an option in an ASC, but there may be other ways to enhance revenue. For example, some practices have added 10 percent to their revenue with the inclusion of additional services such as the appropriate use of nerve blocks and ultrasonic guidance in orthopedic facilities.
- Consider ways of reducing the costs of care.
In the example provided, the practice can manage with physicians only, since the average daily collections are roughly equal to the cost of the physicians (see Table 2). However, as shown in Table 3 this is rarely the case. Many factors determine the cost per anesthetizing location. Table 2 shows the basic elements of the calculation: the total cost of each category of provider, the number of weeks each works and the number of clinical location days to be covered.
This represents an ideal situation, in which a practice has the opportunity to dedicate three CRNAs under the direction of a physician. This is very rarely the case. However, changes in the staffing model may be problematic for some practices for a variety of philosophical and practical reasons. Many anesthesiologists prefer to work alone and not medically direct CRNAs. Until recently, private anesthesia groups in California rarely employed CRNAs, despite the fact that they were routinely used in academic centers, Kaiser hospitals, the military and small, rural facilities.
Qualified CRNAs may not be readily available in certain markets. As some of the nation’s largest staffing companies convert to a medical direction model, which has increased the demand for CRNAs, the supply has yet to catch up. A number of practices considering hiring CRNAs report that it is not easy to find providers who are willing to work where the practice needs them.
Changes in staffing model or the development of a new staffing model for a facility must be carefully evaluated. An anesthesia practice can’t change its culture or mode of delivery quickly. New entities are being formed on a regular basis to target the ambulatory market. Almost without exception, these entities are based on a care team model, where anesthesiologists supervise CRNAs or anesthesiologist assistants.
Critical Metrics
In this era of rapid change, metrics matter. There can be no doubt about the value of clinical data in the OR. Most providers pride themselves on being able to make timely and accurate clinical decisions in a matter of seconds. Why, then, do so few practices fail to apply this same principle to the management of their practices? It is probably the result of a perception that, unlike anesthesia delivery, anesthesia practice management is not a time-critical exercise. No one talks about hours of boredom punctuated by moments of sheer terror in the anesthesia board meeting. However, practices that don’t monitor key metrics closely can make some costly mistakes.
Three distinct management metrics are often confused in the assessment of anesthesia staffing: provider productivity, OR utilization and profitability. Each has its place in the ongoing evaluation of any coverage arrangement.
Provider Productivity
Provider productivity is the term most commonly misused. Technically, it is a measure of the manner in which a provider completes their assigned cases. In other words, if there are only three cases on the schedule and the anesthesia provider completes them all satisfactorily, then they have achieved 100 percent productivity. This said, different fewer units in the completion of the same number of cases than their colleagues, which could be considered a measure of productivity, but very few practices seriously monitor such measures.
OR Utilization
Most practices are actually interested in OR utilization. This is a comparison of actual to potential production. If an OR is open for cases for eight hours a day, then the optimal utilization is typically considered to be six hours. Utilization metrics are normally calculated as a percentage of potential. Six hours of billed anesthesia time during an eight-hour shift would represent 75 percent utilization. It can be useful to compare actual billed hours of anesthesia time to coverage requirements. This is especially useful in that manpower and staffing is always a function of the facility’s coverage requirements.
Profitability
Profitability is not always an easy concept to apply to an anesthesia practice in which providers simply get paid based on collections net of expenses. If it costs you $.50 to make a hamburger and you sell it for $2.00 then your profit is $1.50 per burger. While most practices do not think this way, profit is defined as revenue generated minus the expense of providing the service. If it costs the practice $2,130 per provider day and the practice generates $1,700 per day, then the arrangement is unprofitable. However, if the cost can be reduced to $1,580, then the same level of revenue would result in a profitable arrangement. However, unless you have this information you cannot really know whether the arrangement is profitable or not.
It used to be that success in anesthesia was defined simply in terms of collections. A favorable payer mix and busy ORs were all a practice needed to be successful. Life is no longer so simple. Anesthesia providers must now learn the arcane science of cost accounting. For each venue or line of business, the practice should be able to clearly monitor both the revenue potential and the actual cost. Table 3 is an example of what this might look like. It is based on actual data for a practice in the western United States. Because this is a physician-only practice that allows providers to work as much or as little as they want, the cost part of the equation has yet to be established. Even so, this data clearly demonstrates the financial value of each facility.
Strategic Considerations
The five categories of ambulatory practices shown in Table 1 represent a continuum of management opportunities and challenges. Increasingly, anesthesia practices are actively pursuing new venues and lines of business to diversify. The good news is that well-managed outpatient venues can increase the yield per day and offset hospital coverage and call obligations. The problem is that not all outpatient venues are such a good fit. Adding venues and case volume for the sake of growing a practice can be a very bad idea, especially if new venues require additional manpower and staffing whose costs are not covered by additional revenue potential.Most American hospitals now provide care on an inpatient and outpatient basis. This is considered essential in the current environment. How they achieve the objective or provide a more customer-friendly environment for healthy patients undergoing relatively minor procedures may vary greatly. Some will try to create the look and feel of an ambulatory environment in existing ORs. When this occurs, anesthesia is essentially a captive participant to the change. The hope is that the facility restructuring will increase cases and improve the payer mix.
For the anesthesia practice, such developments tend to represent a difference of degree rather than of kind. The outpatient unit’s focus and business objectives may be more specific, but the outpatient ORs are typically managed by the same people and in the same manner as the inpatient rooms.
The freestanding surgery center that is a hospital joint venture with a group of surgeons represents the next step in the migration of surgical cases from the hospital to the freestanding environment. Various factors may motivate such an arrangement. Every administration is competing for surgeon allegiance. The establishment of a patient-friendly facility with convenient ingress and egress may be one way to accomplish this. The joint venture may be a preemptive strike to keep the surgeons from building their own facility and competing with the hospital.
There is a critical management concept at work here that can have a significant impact on anesthesia. Hospitals must serve a range of customers and, therefore, strive to develop policies that provide a consistent level of service. The hospital will try to schedule cases together as efficiently as possible to maximize the return for a day’s work. They want surgeons to complete cases as expeditiously as possible. Surgeons, by contrast, may want to do a couple of cases in the morning, go to their office and then come back for a case or two in the afternoon. The result can be a significant amount of unproductive downtime for the anesthesia providers.
Each of these types of facilities must be evaluated on its own merits. It can be dangerous to assume that what worked at facility A will now have the same results in facility B. Herein lies one of the trickiest aspects of the ambulatory anesthesia market. How do you determine that covering a facility will be a good deal?
It all starts with the data. If the facility can provide reliable payer mix and volume information, the practice can project revenue. Clearly defined coverage requirements will allow for the formulation of a staffing model. However, such detail often is not available. This can be a big problem. Miscalculating revenue can be very serious. Facilities in rampup mode tend to be overly optimistic in projecting the likelihood of achieving an optimum run-rate.
Working in a doctor’s office, which does not have all of the equipment and recovery drugs for general anesthesia as a hospital or ASC, poses its own set of challenges. The doctor’s office is the extreme end of the convenience/safety continuum. Most of the resources and safeguards that make a hospital OR a safe place to provide anesthesia are typically absent in the doctor’s office. If there is an anesthesia machine, the anesthesiologist may have to provide it. The doctor’s office is the ultimate example of bowing to the surgeon’s needs. Agreeing to provide general anesthesia under such circumstances assumes that one has a very good relationship with the surgeon, that the patients are consistently healthy, and that the payer mix and volume cover the costs of the provider’s with such an environment.
As in so many aspects of business, deciding whether to provide anesthesia outside of the hospital involves a risk-benefit calculation. The specialty prides itself on its safety. Morbidity and mortality related to anesthesia are at an all-time low. The tragic story of Joan Rivers is a constant reminder that such standards should never be compromised.
The Real Question
Most anesthesia practices now understand that they have only three options to survive: expand, merge or sell out. There are very few practice situations where the status quo will work. Hospitals are merging. Customer expectations are changing. The economics of anesthesia are becoming increasingly more challenging. More than 75 percent of all group practices need some level of financial support to survive. So there are many reasons to actively explore practice options. The question is what options actually make sense? The logical tendency is to follow the cases as they migrate into non-traditional venues. It has become inevitable, but is it a good thing?The answer depends on the following factors:
An appropriate culture and structure is a prerequisite. Many small practices (fewer than 10 providers) simply do not have the depth of staff or the flexibility to expand, which is a limitation they may ultimately have to deal with. Other practices consist of providers who are risk-averse and therefore disinclined to take on additional coverage responsibilities. There are practices that simply feel comfortable with the practice they have and have no desire to complicate things.
The financial objectives of the members can be an essential determinant but may also be a source of great debate or conflict. For example, younger members may be very eager to expand the practice and position it for the future, while older members with an eye on retirement may not be so inclined. Obviously, any decision to expand the practice must have membership support. Many practices have watched opportunities come and go as they debated the merits.
At issue is whether the additional venue will enhance partner or shareholder compensation. This is where practice demographics really come into play. Millennials with medical school loans and big mortgages are more inclined to assume risk than those who are closing in on the end of their career. This places a special burden on management to demonstrate the value of the additional cases.
The local market is also a critical factor. Some locations are more target-rich than others. Many practices feel they must pursue every anesthesia opportunity in the local market in order to fend off potential competitors. However, not every practice that wants to expand has the ability to do so without looking at venues that are distant to the primary sites. Careful environmental scanning is an essential prerequisite for any level of expansion. Management must be aware of any and all opportunities and have the ability to assess them objectively.
A practice’s structure and infrastructure will either facilitate or complicate a successful expansion. Some practices are run in a more business-like manner than others. A decision to take on another facility requires decisiveness and strong management. The practice must have a clear chain of command and the ability to manage remote sites effectively. The practice has to be able to clearly demonstrate its ability to meet customer expectations and requirements consistently.
One of the distinct advantages that the nation’s largest staffing companies can demonstrate is their organizational structure. This allows them to prepare more impressive proposals, present more compellingly and monitor ongoing performance more consistently. It is not uncommon for an inexperienced management team to mess up the first few proposals.
Strategic thinking is a relatively new discipline for anesthesia practices. How will a practice position itself to survive in the current environment? The answers and options are not always clear. This can be the most complicated issue of them all.
Howard Greenfield, MD, co-founder and principal of Enhance Healthcare Consulting, is a board certified anesthesiologist with a thorough understanding of the financial and clinical needs of both hospitals and anesthesia providers. Throughout his career, he has worked with hospitals and providers to align incentives and develop cost-effective and timely solutions for OR management. In addition, he has expertise in optimizing anesthesia group and OR performance by working collaboratively with hospital administration, surgeons, OR nurses and anesthesiologists nationwide. He was a founding partner of Sheridan Healthcare and served as chief of anesthesia at Memorial Regional Hospital, Hollywood, FL. Dr. Greenfield received his training at Temple University School of Medicine and Jackson Memorial/University of Miami. He can be reached at hgreenfield@enhancehc.com or (954) 242-1296.Jody Locke, MA, serves as Vice President of Anesthesia and Pain Practice Management Services for Anesthesia Business Consultants. Mr. Locke is responsible for the scope and focus of services provided to ABC’s largest clients. He is also responsible for oversight and management of the company’s pain management billing team. He is a key executive contact for groups that enter into contracts with ABC. Mr. Locke can be reached at Jody.Locke@AnesthesiaLLC.com. -
How Much Call is Too Much?
Robert Johnson, MBA Principal
Enhance Healthcare Consulting, Aventura, FLAnyone who has had to leave in the middle of a family dinner because of a call from labor and delivery or tried to sleep in the call room knowing that a recently completed case is bleeding and likely to come back that night probably also wonders whether they should be working somewhere with less call responsibility.Working on call is part of the responsibility of being an anesthesiologist. It can also be an annoyance that can interfere with work/life balance. Driving back to the hospital for the second time on a beautiful Saturday afternoon, you may start to wonder whether you are on call more than others and possibly working in the wrong place. But how would you know? Your job may pay well and offer generous retirement benefits, but perhaps a job without cardiac, obstetric or trauma unit call responsibilities would make your life easier.
You might find an opportunity that pays less with fewer call days. Should you take the trade-off or keep looking?
The lack of published data on the frequency of required call responsibility among anesthesiologists makes it hard to compare professional opportunities. Surveys of compensation and time off are not hard to find. The same is not true for call.
Data is also lacking on the various types of call, including call from home (beeper call) and in-house call for hospitals that require 24/7 on-site coverage. The number of hours spent on call at the hospital also matters to many. If a position doesn’t require an obstetric beeper call rotation every other weekend, but requires in-house trauma call for the entire weekend, but only once a month, which is better? What are other anesthesiologists in your area required to do?
Colleagues often ask about the “typical” or “average” amount of call and how much call is “too much.”
The lack of national published data prompted Enhance Healthcare to conduct its own survey utilizing Survey Monkey in order to gather information about the frequency and types of call taken by anesthesiologists across the United States.Our initial assumption was that there are two basic types of call about which to ask: 1) call from home (beeper call) and 2) in-house (restricted). We wanted to understand what circumstances led to various on-call requirements and whether and where call was provided by anesthesiologists compared to CRNAs. Finally, we wanted to see whether there were any significant relationships between specialty considerations and amount or type of call. We were particularly interested in 1) obstetric services (and the number of deliveries); and 2) trauma services and trauma classification level (I, II or III).
The survey consisted of eight to 13 questions, the total number of questions depending on answers to conditional questions (see Table 8 at the end of this article). Of 155 responses received, 21 responses were eliminated due to a lack of appropriate information.
We believe, but cannot demonstrate, that the remaining 134 respondents were all affiliated with different facilities. Therefore, the survey would represent 134 providers at 134 facilities. The surveys were distributed to anesthesia professionals across the country, so we believe the results are not skewed to any particular geographic area. We also stress that the results discussed in this article were not statistically validated at the time of publication. However, we intend to do so in future articles utilizing more sophisticated analyses, such as analysis of variance (ANOVA).
Beeper or In-house
The first four survey questions asked respondents to report whether they take weekday and/or weekend call from home (beeper call) or in-house. The data revealed little or no difference in weekday versus weekend for either type of call (see Charts 1 and 2). The lack of difference between weekday and weekend values is probably due to the fact that, except for a few respondents, the same individuals who take weekday call also take weekend call.The data did show that there were three categories of call: 1) beeper only; 2) in-house only; and 3) a mix of beeper and in-house. Approximately 57 percent of respondents have (weekday and weekend) in-house call an average of five days per month. (See Table 1.) Approximately 85 percent of respondents have (combined weekend and weekday) beeper call as some component of their call an average of 7.8 days from home per month.
The combined results show that a typical provider taking in-house call could expect their facility to require an average of six days per month on-site in the hospital. A provider at a facility requiring beeper call could expect, on average, to spend eight days per month on beeper call. A limitation of the survey was that it did not ask respondents to indicate first call versus second call; however, the results suggest that the average provider at a typical facility has slightly more than one call day weekly (presumably first call) and one weekend per month.
Taking only in-house call and only beeper call represent 57 percent and 85 percent of respondents, respectively.
Along with the number of days spent on call, time spent continuously on-site is also an issue. Since the in-house providers who responded to the survey were working an assigned shift (i.e., only 24 hours), only respondents taking call from home were asked how long they spent on-site when called in from home. Tables 2 and 3 show that, on average, anesthesiologists spend a little over four hours on a weekday and over seven hours on a weekend day on-site when called into the facility from home. The authors note that, to their surprise, the total hours spent on-site did not appear to differ significantly by specialty being covered at the facility. We are planning a follow-up study on this topic.In-house On-Call Characteristics
We asked participants whether their facility required in-house call (on-site presence 24/7). Hospitals typically refer to in-house call as “restricted call” and beeper call as “unrestricted call.” Sixtyseven percent of respondents reported that their facilities require in-house call (Chart 3). One would expect that the percentage of respondents taking in-house call, either with or without a beeper, would be close to this percentage. However, as shown in Charts 1 and 2, the combined percentage for weekday and percent difference. This may be because providers who do not take in-house call work at facilities where in-house call is required of others (e.g., obstetric anesthesiologists or CRNAs). Chart 4 compares CRNA and physician anesthesiologist providers.
On-Call Characteristics By Specialty: Obstetrics
Eighty-three percent of respondents indicated that their facilities had an obstetrics program. Annual deliveries ranged from 300 to 11,000. Table 4 shows the impact of an obstetrics program on percentages of call type. Days of call type per month do not appear to differ significantly between obstetric and non-obstetric call. (Thirteen respondents indicated an obstetrics program at their institutions but did not provide an annual number of births. Their responses were not included in calculations involving the number of births.)However, the proportions of call types were significantly different in obstetrics, particularly in the “in-house only” and “beeper only” categories. This is consistent with our finding suggesting that the size of an obstetrics program would have an impact on whether or not it had an in-house call component. Further study is warranted to separate other variables such as trauma and use of CRNAs for in-house call.
On-Call Characteristics By Specialty: Trauma
Forty-eight percent of the respondents worked at a facility with a trauma program. There were few differences in the number of trauma on-call days between facilities with and without trauma programs, with the exception of a decrease in beeper-only call from 9.6 to 8.7 days. As with obstetrics, the presence of a trauma program alone does not appear to change the number of days on call. We are planning an additional study to analyze the confounding variables of obstetrics and trauma in programs with and without CRNAs.
As seen in Table 6, trauma programs do have an impact on the proportions of call type. The most dramatic difference was seen in beeper only call in institutions with and without a trauma center (28 percent and 55 percent, respectively).
Not surprisingly, there was an apparent correlation between trauma level and number of days and types of call. (Level I and II trauma programs require 24/7 anesthesia in-house coverage.)
A preliminary view of the differences to be analyzed in future reports is shown in Chart 6. As stated earlier, the use of CRNAs has a large impact on the absolute number of physician anesthesiologists used for call, but the number also varies by trauma level.
Conclusion
How much call an anesthesiologist takes is subject to many variables. This study looked at weekdays, weekends, obstetrics and trauma. There do not appear to be differences between weekday and weekend coverage. Neither the number of days nor the hours per day required on-site for call appear to differ much between the facilities that require obstetric and trauma coverage. However, the relative proportions of call responsibility for beeper and in-house call reveal significant differences.Further study to analyze the covariant impact on this phenomenon is warranted, along with further review of the impact of the various trauma levels.
The answer to the question of how much call is too much call is: it’s complicated! At a minimum, clinicians should carefully review call requirements for any practice they are thinking of joining, with consideration for the potential impact of obstetrics and trauma on how much inhouse coverage they will be required to provide.
Robert Johnson, MBA, principal at Enhance Healthcare Consulting, is a healthcare executive with broad experience in multiple healthcare environments. He started at Johns Hopkins Hospital as a perfusionist in the cardiac operating rooms and eventually became administrator of the anesthesiology department. He has also served as senior associate chief operating officer at Duke Hospital and held positions with Baylor College of Medicine, the University of Pittsburgh and Sheridan Healthcare. As a vice president for Hospital Corporation of America, he played a critical role in leading negotiations with hospital-based physician practices. He joined EHC as a principal in 2014. He can be reached at bob.johnson@enhancehc.com or (404) 905-7014. -
Six Years On: The Growing Pains—and Remarkable Growth—of the Perioperative Surgical Home
Roseanne M. Fischoff, MPP
Economics and Practice Innovations Executive, American Society of Anesthesiologists- One regional medical center saved $1.5 million in the first year.
- A Midwest academic center reduced average length of stay (LOS) for total joint replacement patients from 4.6 to 2.1 days.
- A pediatric institution reduced the 30-day readmission rate from 8.3 percent to 7.5 percent for laryngeal cleft patients while reducing average cost by approximately 20 percent.
- An academic center reduced costs for cystectomy cases by an average of $10,000 per case.
- A major health system improved room turnover by approximately eight minutes, reduced LOS for hip/knee arthroplasty cases from an average of 110 hours to 51 hours and cut the readmission rate for hip/knee arthroplasty cases in half.
Having devised and championed the concept of the anesthesia care team in the early 1980s, anesthesiologists have been at the forefront of team-based, collaborative care for decades. As healthcare increasingly transitions from an emphasis on volume to one of value, the importance of teamwork becomes ever more crucial.The American Society of Anesthesiologists (ASA) formally introduced the perioperative surgical home (PSH) in 2012 as an innovative patient-centered model of care designed to achieve the triple aim of improving health, improving the delivery of healthcare and reducing costs.
Perhaps the strongest core feature of the PSH model is the team. Alongside the many thousands of individuals who have been involved in PSH programs throughout the country, the PSH model—and the ASA’s first two PSH Learning Collaboratives— are being increasingly embraced by a variety of influential healthcare organizations. In March 2018, the PSH Learning Collaborative was accepted by the American Board of Medical Specialties Multi-Specialty Portfolio Program, meaning that Learning Collaborative participation will be recognized for Maintenance of Certification Part IV credit by 24 specialty boards, including the American Board of Surgery. Notable PSH partner organizations include the American Academy of Physical Medicine and Rehabilitation (AAPMR), the American Academy of Orthopedic Surgeons (AAOS) and the American Urological Association (AUA).
Practice improvement examples like those at the beginning of this article continue to demonstrate that the PSH is a viable and effective care model that can be incorporated into institutions of any size and for a wide variety of procedures and modalities.
In 2014, the ASA teamed with Premier, Inc., a leading healthcare improvement company, to establish the first PSH Learning Collaborative, which brought together subject matter experts and leading institutions from across the country to learn from each other. The first Collaborative featured 44 groups, and the recently completed Learning Collaborative 2.0 comprised 57 organizations that shared insights about PSH strategies compatible with alternative payment models, including Bundled Payments for Care Improvement, Comprehensive Care for Joint Replacement, the Medicare Shared Savings Program and Accountable Care Organizations.The nearly 100 institutions and healthcare professionals who participated in the first two Learning Collaboratives reported positive outcomes that have benefited their organizations and their patients in sometimes surprisingly short periods of time. However, no matter how successful any of these nascent PSH models turned out to be, all experienced challenges that informed their actions going forward and served as learning opportunities for their peers.
The individuals below recently shared the successes and challenges of incorporating a PSH model into their institutions.
Christopher Steel, MD
White River Health System
Batesville, ArkansasEarly in their PSH program, Dr. Steel and his group formed preoperative, intraoperative and postoperative teams. They found that in team meetings, each team wanted to focus solely on outcome measures rather than consistently following the established protocols. As a result, they accomplished very little in the first few meetings. Subsequently, the team focused on precision and accuracy. The precision efforts focused on reproducibility of the protocol rather than outcomes. As a result, they were able to create PSH-driven protocols. The accuracy efforts were focused on making small changes to the protocols over time based on the patient outcomes.
Like many other organizations developing PSH models, the White River Health group quickly learned how important it was to name the right leaders. Dr. Steel was originally designated as sole director of the PSH, which he later called “short-sighted.” When his group added orthopedic surgeon Jeff Angel, MD, as co-director, the other orthopedic surgeons became more engaged and the program began building momentum.A mobile phone app helped to solve their problem of disseminating protocols to team members. This content was at first put on paper and filed in binders strategically placed throughout the hospital. When changes were made, they had to find the appropriate papers and make the change in each binder. Later, a shared computer drive proved unsuccessful because finding a local computer was difficult and the log-in process was too cumbersome. The mobile phone app turned out to be the best way for everyone involved in the patient’s care to access and review up-to-date information.
Dr. Steel indicated that identification of a payment mechanism should be a top priority for institutions that develop a PSH. It’s not necessary to have one at the outset, but eventually everyone must figure out a way for the hospital and providers to be reimbursed for the effort required to accomplish care design. Otherwise, sustained efforts and growth are unlikely.
For Dr. Steel and the White River Health System, the PSH model has, so far, delivered on its core principles. “It doesn’t matter what you call it. Every hospital should strive to improve quality and improve the experience of patients and providers,” he said. “By reducing variation, a PSH or similar model can simplify the delivery of care for the patients and the providers while meticulously ensuring improved quality and usually a decreased total cost of care.”
Leslie Garson, MD
University of California, IrvineDr. Garson was an early adopter of the PSH model at his institution and has been fine-tuning his program for several years. Like Dr. Steel and the White River Health System, identification of PSH champions was crucial for success. In Dr. Garson’s case, a surgeon champion and senior leadership support were essential. Non-physician support is also necessary as well. Preferably, this is someone with experience working with clinical pathways who can shepherd the project through the writing of clinical pathways, working with committees and completing order sets.
While leadership support and champions are critical, they are perhaps less important to continued success than collaboration and buy-in from the entire spectrum of team members. Too much reliance on a particular champion—whether a surgeon, anesthesiologist or administrator—can be disastrous if that person leaves and the clinical pathway goes with them.
Dr. Garson emphasized that clinical pathways need to be as hard-wired as possible. This means explaining to the entire team, again and again, that clinical pathways are not “cookbook medicine,” but rather a scaffold or skeleton of evidence-based care that can be endlessly modified and customized for the 20 to 30 percent of patients who need more individualized treatment protocols.
“A PSH program provides the ability to implement a continuum of care plan in the perioperative period for a patient’s episode of care—be it joint replacement, colon resection or any of a myriad of other procedures—that is developed in a multidisciplinary, collaborative manner ensuring good communication and seamless care management across all touch points by all providers for that patient.”
Gary Stier, MD, MBA
Loma Linda UniversityDr. Stier and his group at Loma Linda found out early in their PSH journey that they had underestimated the difficulty of navigating the byzantine information technology (IT) landscape typical of a large medical institution. IT support is crucial, but with limited available resources at their institution, gathering data, creating analytic tools and customizing their electronic health record (EHR) for enhanced workflow presented significant challenges. In response, they mapped the IT structure and governance to better understand who in IT to talk to and how to navigate the system. Frequent communication with appropriate IT staff helped to build crucial relationships, leading to a better overall understanding of the PSH model and how it fit into the organization’s mission.
The importance of adequately sharing the vision of the PSH does not stop with IT staff. Dr. Stier stressed the necessity of educating administrators and other surgical colleagues about the PSH model, calling the process “an uphill journey.” Surgeons, for instance, are surely aware of and most likely pushing for the development of enhanced recovery after surgery (ERAS) programs and the institutional resources needed to develop them. The PSH champion must focus on educating all stakeholders that the PSH model is, in fact, a more comprehensive ERAS delivery model developed to enhance both surgical service line care and to facilitate, create and implement procedure-specific ERAS protocols.
The group also found it imperative to emphasize to their department members that the PSH model is a complementary part of the anesthesiology group’s practice. They created a voluntary anesthesiology PSH team that embraced the model and talked positively about its value to department members. By demonstrating positive outcomes, such as reduced LOS, patient satisfaction and surgical team satisfaction, and presenting an acceptable pro forma, they were better able to obtain faculty support and funding for the PSH. Regular meetings with key stakeholders ensured ongoing awareness of and support for the program.
As with any new patient care paradigm, the reality of implementing a PSH lies in the conflict between the time and resources required to perform clinical and administrative duties. In response to the challenge, Dr. Stier and his group initially performed needed administrative activities on personal time; however, once organizational funding for the PSH program was secured, the finances needed for the administrative duties were no longer an issue.
For those thinking of developing their own PSH model, Dr. Stier recommended acquiring at least a basic knowledge of project management, process improvement, study design, statistical analysis and data gathering methods, much of which can be attained through existing institutional programs, books and online resources.
Dr. Stier also recognized that focusing group efforts early on in creating and implementing timely protocols and order sets for the surgical services they partnered with would have allowed them to more effectively reduce surgical practice variation and improve outcomes sooner. In addition, publishing a paper on their PSH outcomes likely would have moved the program forward much sooner.
As the PSH Learning Collaborative moves toward its third incarnation (PSH Learning Collaborative 2020), Dr. Stier emphasized the characteristics that make it patently unique: “The numberone advantage of participating in the PSH Learning Collaborative is the collaborative nature of membership—sharing resources and building relationships. PSH teams can clearly become experts in the development and implementation of perioperative care coordination programs, perioperative chronic disease management, facilitating the creation of clinical pathways and order sets, navigating the IT landscape and financial management of such programs. Creating successful PSH programs can ensure job security and career.”The PSH Learning Collaborative 2020
Recruitment for the PSH Learning Collaborative 2020 is now under way. The collaborative will begin in May and run for two years. This iteration of the collaborative will assist facilities in PSH pilot implementation, optimization and expansion into new service lines or system-wide conversion.
It will also help facilities overcome the challenges they face with making the change to value-based payment. Organizations will be guided through participation in mandatory and elective bundles and understanding the impact that the Quality Payment Program (QPP) of the Medicare Access and CHIP Reauthorization Act of 2017 (MACRA), including the Merit-Based Incentive Payment System (MIPS) and Advanced Alternative Payment Models (APMs) will have on their organization.
This effort is important because value-based payment is quickly being adopted by private as well as public payers.
To meet the unique needs of organizations interested in healthcare redesign, institutions can choose from two participation options:
The first, the Core Collaborative, is designed for organizations interested in learning more about the PSH model of care and those in the early stages of implementing a PSH pilot.
The other, the Advanced Cohort, is designed for organizations looking to optimize or expand their PSH pilot. Advanced Cohort participants also can be part of the Bundles Payment Add-On option, which allows them to assess their facility’s benefits and risks in participating in the various bundled payment programs.
Regardless of which learning track an organization chooses, institutions will complete the program with the confidence, tools and resources to begin the next phase of PSH pilot implementation.
To learn more about the PSH Learning Collaborative 2020, visit asahq.org/psh-learn or email PSH@asahq.org.
Roseanne M. Fischoff, MPP, serves as the Economics and Practice Innovations Executive for the American Society of Anesthesiologists (ASA). In this role, Ms. Fischoff develops and implements policies and operating structure to advance the ASA’s economic and practice innovation agenda. This work includes ensuring that the interests of anesthesiologists in regulatory affairs are well represented as they intersect with payment and practice management issues. Ms. Fischoff leads the promotional, educational and advocacy efforts for the perioperative surgical home initiative. She also serves as a catalyst for product and service innovation to support ASA members engaged in redefining the future of the specialty. She can be reached at R.Fischoff@asahq.org.
 Anesthesia groups are facing great challenges in today’s environment. I am sure you are aware of these various challenges so I won’t belabor them.
Anesthesia groups are facing great challenges in today’s environment. I am sure you are aware of these various challenges so I won’t belabor them. Many will take exception to these benefits of independent practice. But when you speak to such individuals, ask them how they make their money, and you will likely find that they make it by getting you to sell out. Almost everyone out there who offers advice on whether or not to sell your practice is incentivized for you to do the deal.
Many will take exception to these benefits of independent practice. But when you speak to such individuals, ask them how they make their money, and you will likely find that they make it by getting you to sell out. Almost everyone out there who offers advice on whether or not to sell your practice is incentivized for you to do the deal. Therefore, the most effective groups have systems and processes to quickly and effectively deal with disruptive physician behavior. This could include creating a code of conduct by which the group can measure behavior, establishing an internal review process, and creating a formal process to deal with disruptive situations (see “
Therefore, the most effective groups have systems and processes to quickly and effectively deal with disruptive physician behavior. This could include creating a code of conduct by which the group can measure behavior, establishing an internal review process, and creating a formal process to deal with disruptive situations (see “ Will Latham, MBA, is president of Latham Consulting Group, Inc., which helps medical group physicians make decisions, resolve conflict and move forward. For more than 25 years Mr. Latham has assisted medical groups in the areas of strategy and planning, governance and organizational effectiveness, and mergers, alliances and networks. During this time he has facilitated over 900 meetings or retreats for medical groups; helped hundreds of medical groups develop strategic plans to guide their growth and development; helped over 130 medical groups improve their governance systems and change their compensation plans; and advised and facilitated the mergers of over 120 medical practices representing over 1,200 physicians. Mr. Latham has an MBA from the University of North Carolina in Charlotte. He is a frequent speaker at local, state, national and specialty-specific healthcare conferences. Mr. Latham can be reached at (704) 365-8889 or
Will Latham, MBA, is president of Latham Consulting Group, Inc., which helps medical group physicians make decisions, resolve conflict and move forward. For more than 25 years Mr. Latham has assisted medical groups in the areas of strategy and planning, governance and organizational effectiveness, and mergers, alliances and networks. During this time he has facilitated over 900 meetings or retreats for medical groups; helped hundreds of medical groups develop strategic plans to guide their growth and development; helped over 130 medical groups improve their governance systems and change their compensation plans; and advised and facilitated the mergers of over 120 medical practices representing over 1,200 physicians. Mr. Latham has an MBA from the University of North Carolina in Charlotte. He is a frequent speaker at local, state, national and specialty-specific healthcare conferences. Mr. Latham can be reached at (704) 365-8889 or  Let’s start with the truth: professional services are not, and cannot, be a commodity. But it’s also true that many have fooled themselves (or, more likely, others) into believing that they are. In fact, there’s an RFP industry ready to help.
Let’s start with the truth: professional services are not, and cannot, be a commodity. But it’s also true that many have fooled themselves (or, more likely, others) into believing that they are. In fact, there’s an RFP industry ready to help. Although no outside assessment of category can be completely reliable, clues often abound. And category dictates strategy.
Although no outside assessment of category can be completely reliable, clues often abound. And category dictates strategy. Mark F. Weiss, JD, is an attorney who specializes in the business and legal issues affecting physicians and physician groups on a national basis. He served as a clinical assistant professor of anesthesiology at USC Keck School of Medicine and practices with The Mark F. Weiss Law Firm, a firm with offices in Dallas, Texas and Los Angeles and Santa Barbara, California, representing clients across the country. He can be reached by email at
Mark F. Weiss, JD, is an attorney who specializes in the business and legal issues affecting physicians and physician groups on a national basis. He served as a clinical assistant professor of anesthesiology at USC Keck School of Medicine and practices with The Mark F. Weiss Law Firm, a firm with offices in Dallas, Texas and Los Angeles and Santa Barbara, California, representing clients across the country. He can be reached by email at  The steady migration of surgical cases from traditional inpatient to non-traditional outpatient and ambulatory venues has required anesthesiologists and CRNAs, the quintessential service providers, to continuously reinvent themselves to adapt to evolving market conditions and customer expectations. The assumptions and strategies that helped many anesthesia groups build successful partnerships with hospitals may no longer serve them well in today’s dynamic ambulatory environment.
The steady migration of surgical cases from traditional inpatient to non-traditional outpatient and ambulatory venues has required anesthesiologists and CRNAs, the quintessential service providers, to continuously reinvent themselves to adapt to evolving market conditions and customer expectations. The assumptions and strategies that helped many anesthesia groups build successful partnerships with hospitals may no longer serve them well in today’s dynamic ambulatory environment. This is not the case with outpatient and ambulatory facilities, especially if they need anesthesia only a few days a week or if anesthesia is needed for only a few cases per day. Large practices with multiple outpatient relationships often create a separate scheduling function to ensure that their providers meet their obligations at the various facilities in a timely manner. The economics of ambulatory anesthesia are not always as favorable as one might expect. Practices often focus on general production data that does not allow the practice to compare business lines or assess their profitability. Standard billing reports that simply show basic anesthesia values such as cases, units, charges and payments by month—even if they include a breakdown by facility—will never be adequate to manage an expanding and dynamic book of ambulatory business.
This is not the case with outpatient and ambulatory facilities, especially if they need anesthesia only a few days a week or if anesthesia is needed for only a few cases per day. Large practices with multiple outpatient relationships often create a separate scheduling function to ensure that their providers meet their obligations at the various facilities in a timely manner. The economics of ambulatory anesthesia are not always as favorable as one might expect. Practices often focus on general production data that does not allow the practice to compare business lines or assess their profitability. Standard billing reports that simply show basic anesthesia values such as cases, units, charges and payments by month—even if they include a breakdown by facility—will never be adequate to manage an expanding and dynamic book of ambulatory business.

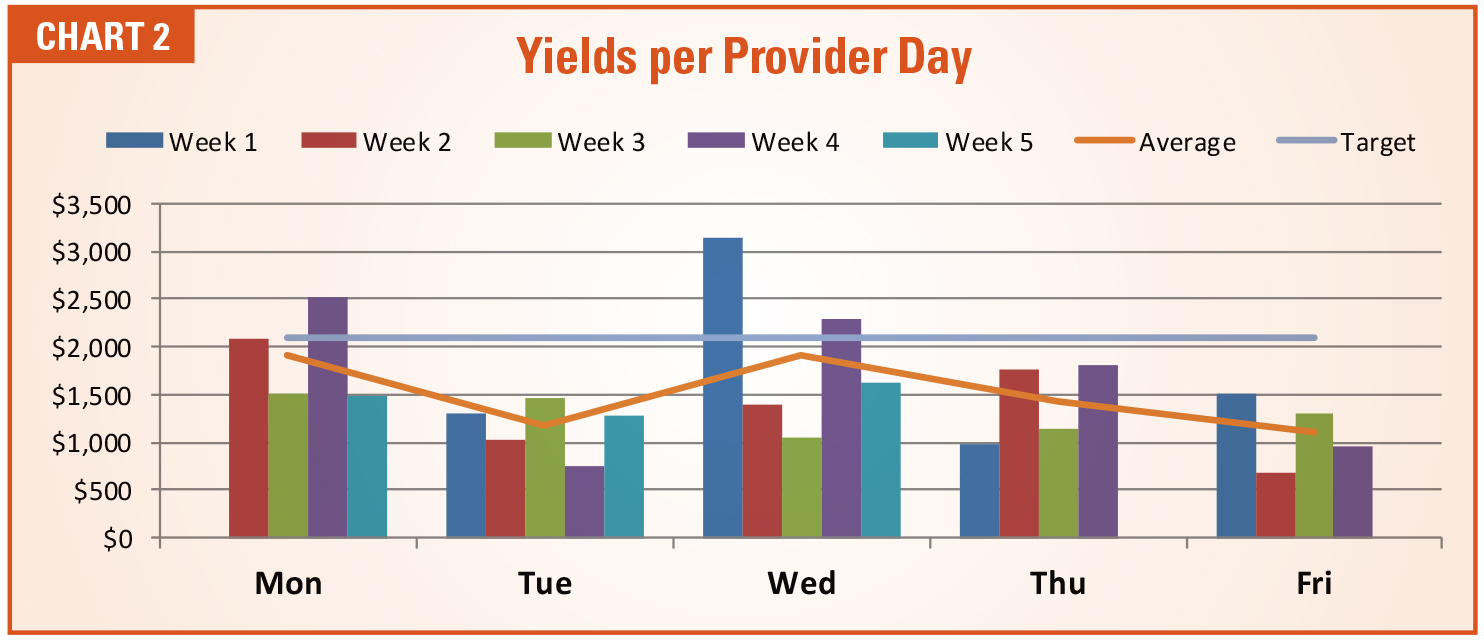


 The five categories of ambulatory practices shown in Table 1 represent a continuum of management opportunities and challenges. Increasingly, anesthesia practices are actively pursuing new venues and lines of business to diversify. The good news is that well-managed outpatient venues can increase the yield per day and offset hospital coverage and call obligations. The problem is that not all outpatient venues are such a good fit. Adding venues and case volume for the sake of growing a practice can be a very bad idea, especially if new venues require additional manpower and staffing whose costs are not covered by additional revenue potential.
The five categories of ambulatory practices shown in Table 1 represent a continuum of management opportunities and challenges. Increasingly, anesthesia practices are actively pursuing new venues and lines of business to diversify. The good news is that well-managed outpatient venues can increase the yield per day and offset hospital coverage and call obligations. The problem is that not all outpatient venues are such a good fit. Adding venues and case volume for the sake of growing a practice can be a very bad idea, especially if new venues require additional manpower and staffing whose costs are not covered by additional revenue potential. Most anesthesia practices now understand that they have only three options to survive: expand, merge or sell out. There are very few practice situations where the status quo will work. Hospitals are merging. Customer expectations are changing. The economics of anesthesia are becoming increasingly more challenging. More than 75 percent of all group practices need some level of financial support to survive. So there are many reasons to actively explore practice options. The question is what options actually make sense? The logical tendency is to follow the cases as they migrate into non-traditional venues. It has become inevitable, but is it a good thing?
Most anesthesia practices now understand that they have only three options to survive: expand, merge or sell out. There are very few practice situations where the status quo will work. Hospitals are merging. Customer expectations are changing. The economics of anesthesia are becoming increasingly more challenging. More than 75 percent of all group practices need some level of financial support to survive. So there are many reasons to actively explore practice options. The question is what options actually make sense? The logical tendency is to follow the cases as they migrate into non-traditional venues. It has become inevitable, but is it a good thing? Howard Greenfield, MD, co-founder and principal of Enhance Healthcare Consulting, is a board certified anesthesiologist with a thorough understanding of the financial and clinical needs of both hospitals and anesthesia providers. Throughout his career, he has worked with hospitals and providers to align incentives and develop cost-effective and timely solutions for OR management. In addition, he has expertise in optimizing anesthesia group and OR performance by working collaboratively with hospital administration, surgeons, OR nurses and anesthesiologists nationwide. He was a founding partner of Sheridan Healthcare and served as chief of anesthesia at Memorial Regional Hospital, Hollywood, FL. Dr. Greenfield received his training at Temple University School of Medicine and Jackson Memorial/University of Miami. He can be reached at
Howard Greenfield, MD, co-founder and principal of Enhance Healthcare Consulting, is a board certified anesthesiologist with a thorough understanding of the financial and clinical needs of both hospitals and anesthesia providers. Throughout his career, he has worked with hospitals and providers to align incentives and develop cost-effective and timely solutions for OR management. In addition, he has expertise in optimizing anesthesia group and OR performance by working collaboratively with hospital administration, surgeons, OR nurses and anesthesiologists nationwide. He was a founding partner of Sheridan Healthcare and served as chief of anesthesia at Memorial Regional Hospital, Hollywood, FL. Dr. Greenfield received his training at Temple University School of Medicine and Jackson Memorial/University of Miami. He can be reached at  Jody Locke, MA, serves as Vice President of Anesthesia and Pain Practice Management Services for Anesthesia Business Consultants. Mr. Locke is responsible for the scope and focus of services provided to ABC’s largest clients. He is also responsible for oversight and management of the company’s pain management billing team. He is a key executive contact for groups that enter into contracts with ABC. Mr. Locke can be reached at
Jody Locke, MA, serves as Vice President of Anesthesia and Pain Practice Management Services for Anesthesia Business Consultants. Mr. Locke is responsible for the scope and focus of services provided to ABC’s largest clients. He is also responsible for oversight and management of the company’s pain management billing team. He is a key executive contact for groups that enter into contracts with ABC. Mr. Locke can be reached at  Anyone who has had to leave in the middle of a family dinner because of a call from labor and delivery or tried to sleep in the call room knowing that a recently completed case is bleeding and likely to come back that night probably also wonders whether they should be working somewhere with less call responsibility.
Anyone who has had to leave in the middle of a family dinner because of a call from labor and delivery or tried to sleep in the call room knowing that a recently completed case is bleeding and likely to come back that night probably also wonders whether they should be working somewhere with less call responsibility. The lack of national published data prompted Enhance Healthcare to conduct its own survey utilizing Survey Monkey in order to gather information about the frequency and types of call taken by anesthesiologists across the United States.
The lack of national published data prompted Enhance Healthcare to conduct its own survey utilizing Survey Monkey in order to gather information about the frequency and types of call taken by anesthesiologists across the United States. The first four survey questions asked respondents to report whether they take weekday and/or weekend call from home (beeper call) or in-house. The data revealed little or no difference in weekday versus weekend for either type of call (see Charts 1 and 2). The lack of difference between weekday and weekend values is probably due to the fact that, except for a few respondents, the same individuals who take weekday call also take weekend call.
The first four survey questions asked respondents to report whether they take weekday and/or weekend call from home (beeper call) or in-house. The data revealed little or no difference in weekday versus weekend for either type of call (see Charts 1 and 2). The lack of difference between weekday and weekend values is probably due to the fact that, except for a few respondents, the same individuals who take weekday call also take weekend call.

 Along with the number of days spent on call, time spent continuously on-site is also an issue. Since the in-house providers who responded to the survey were working an assigned shift (i.e., only 24 hours), only respondents taking call from home were asked how long they spent on-site when called in from home. Tables 2 and 3 show that, on average, anesthesiologists spend a little over four hours on a weekday and over seven hours on a weekend day on-site when called into the facility from home. The authors note that, to their surprise, the total hours spent on-site did not appear to differ significantly by specialty being covered at the facility. We are planning a follow-up study on this topic.
Along with the number of days spent on call, time spent continuously on-site is also an issue. Since the in-house providers who responded to the survey were working an assigned shift (i.e., only 24 hours), only respondents taking call from home were asked how long they spent on-site when called in from home. Tables 2 and 3 show that, on average, anesthesiologists spend a little over four hours on a weekday and over seven hours on a weekend day on-site when called into the facility from home. The authors note that, to their surprise, the total hours spent on-site did not appear to differ significantly by specialty being covered at the facility. We are planning a follow-up study on this topic.




 Eighty-three percent of respondents indicated that their facilities had an obstetrics program. Annual deliveries ranged from 300 to 11,000. Table 4 shows the impact of an obstetrics program on percentages of call type. Days of call type per month do not appear to differ significantly between obstetric and non-obstetric call. (Thirteen respondents indicated an obstetrics program at their institutions but did not provide an annual number of births. Their responses were not included in calculations involving the number of births.)
Eighty-three percent of respondents indicated that their facilities had an obstetrics program. Annual deliveries ranged from 300 to 11,000. Table 4 shows the impact of an obstetrics program on percentages of call type. Days of call type per month do not appear to differ significantly between obstetric and non-obstetric call. (Thirteen respondents indicated an obstetrics program at their institutions but did not provide an annual number of births. Their responses were not included in calculations involving the number of births.)


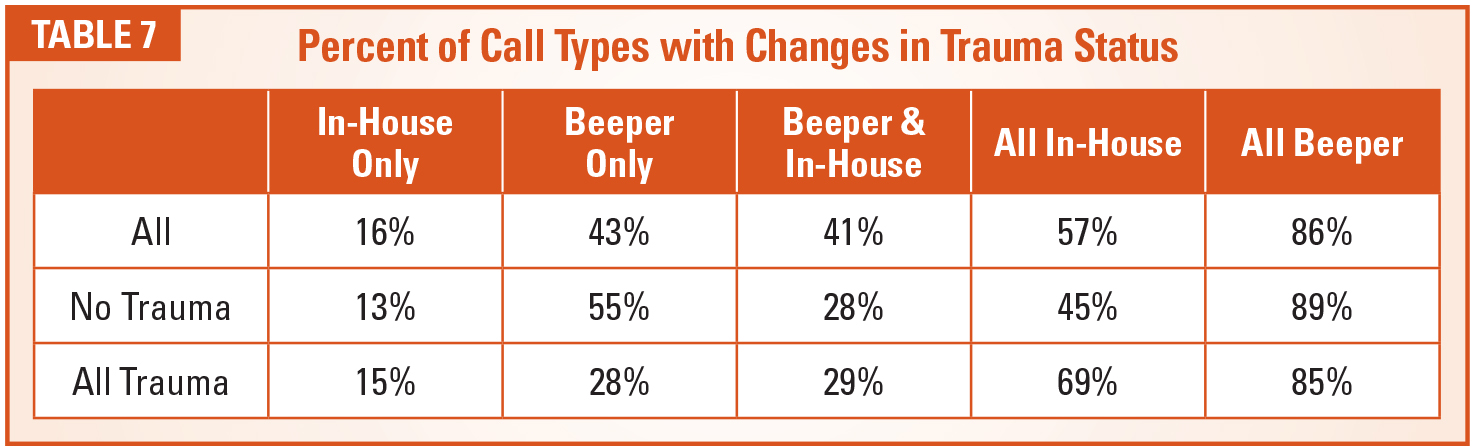


 How much call an anesthesiologist takes is subject to many variables. This study looked at weekdays, weekends, obstetrics and trauma. There do not appear to be differences between weekday and weekend coverage. Neither the number of days nor the hours per day required on-site for call appear to differ much between the facilities that require obstetric and trauma coverage. However, the relative proportions of call responsibility for beeper and in-house call reveal significant differences.
How much call an anesthesiologist takes is subject to many variables. This study looked at weekdays, weekends, obstetrics and trauma. There do not appear to be differences between weekday and weekend coverage. Neither the number of days nor the hours per day required on-site for call appear to differ much between the facilities that require obstetric and trauma coverage. However, the relative proportions of call responsibility for beeper and in-house call reveal significant differences. Robert Johnson, MBA, principal at Enhance Healthcare Consulting, is a healthcare executive with broad experience in multiple healthcare environments. He started at Johns Hopkins Hospital as a perfusionist in the cardiac operating rooms and eventually became administrator of the anesthesiology department. He has also served as senior associate chief operating officer at Duke Hospital and held positions with Baylor College of Medicine, the University of Pittsburgh and Sheridan Healthcare. As a vice president for Hospital Corporation of America, he played a critical role in leading negotiations with hospital-based physician practices. He joined EHC as a principal in 2014. He can be reached at
Robert Johnson, MBA, principal at Enhance Healthcare Consulting, is a healthcare executive with broad experience in multiple healthcare environments. He started at Johns Hopkins Hospital as a perfusionist in the cardiac operating rooms and eventually became administrator of the anesthesiology department. He has also served as senior associate chief operating officer at Duke Hospital and held positions with Baylor College of Medicine, the University of Pittsburgh and Sheridan Healthcare. As a vice president for Hospital Corporation of America, he played a critical role in leading negotiations with hospital-based physician practices. He joined EHC as a principal in 2014. He can be reached at  Having devised and championed the concept of the anesthesia care team in the early 1980s, anesthesiologists have been at the forefront of team-based, collaborative care for decades. As healthcare increasingly transitions from an emphasis on volume to one of value, the importance of teamwork becomes ever more crucial.
Having devised and championed the concept of the anesthesia care team in the early 1980s, anesthesiologists have been at the forefront of team-based, collaborative care for decades. As healthcare increasingly transitions from an emphasis on volume to one of value, the importance of teamwork becomes ever more crucial. In 2014, the ASA teamed with Premier, Inc., a leading healthcare improvement company, to establish the first PSH Learning Collaborative, which brought together subject matter experts and leading institutions from across the country to learn from each other. The first Collaborative featured 44 groups, and the recently completed Learning Collaborative 2.0 comprised 57 organizations that shared insights about PSH strategies compatible with alternative payment models, including Bundled Payments for Care Improvement, Comprehensive Care for Joint Replacement, the Medicare Shared Savings Program and Accountable Care Organizations.
In 2014, the ASA teamed with Premier, Inc., a leading healthcare improvement company, to establish the first PSH Learning Collaborative, which brought together subject matter experts and leading institutions from across the country to learn from each other. The first Collaborative featured 44 groups, and the recently completed Learning Collaborative 2.0 comprised 57 organizations that shared insights about PSH strategies compatible with alternative payment models, including Bundled Payments for Care Improvement, Comprehensive Care for Joint Replacement, the Medicare Shared Savings Program and Accountable Care Organizations. Like many other organizations developing PSH models, the White River Health group quickly learned how important it was to name the right leaders. Dr. Steel was originally designated as sole director of the PSH, which he later called “short-sighted.” When his group added orthopedic surgeon Jeff Angel, MD, as co-director, the other orthopedic surgeons became more engaged and the program began building momentum.
Like many other organizations developing PSH models, the White River Health group quickly learned how important it was to name the right leaders. Dr. Steel was originally designated as sole director of the PSH, which he later called “short-sighted.” When his group added orthopedic surgeon Jeff Angel, MD, as co-director, the other orthopedic surgeons became more engaged and the program began building momentum. As the PSH Learning Collaborative moves toward its third incarnation (PSH Learning Collaborative 2020), Dr. Stier emphasized the characteristics that make it patently unique: “The numberone advantage of participating in the PSH Learning Collaborative is the collaborative nature of membership—sharing resources and building relationships. PSH teams can clearly become experts in the development and implementation of perioperative care coordination programs, perioperative chronic disease management, facilitating the creation of clinical pathways and order sets, navigating the IT landscape and financial management of such programs. Creating successful PSH programs can ensure job security and career.”
As the PSH Learning Collaborative moves toward its third incarnation (PSH Learning Collaborative 2020), Dr. Stier emphasized the characteristics that make it patently unique: “The numberone advantage of participating in the PSH Learning Collaborative is the collaborative nature of membership—sharing resources and building relationships. PSH teams can clearly become experts in the development and implementation of perioperative care coordination programs, perioperative chronic disease management, facilitating the creation of clinical pathways and order sets, navigating the IT landscape and financial management of such programs. Creating successful PSH programs can ensure job security and career.” Roseanne M. Fischoff, MPP, serves as the Economics and Practice Innovations Executive for the American Society of Anesthesiologists (ASA). In this role, Ms. Fischoff develops and implements policies and operating structure to advance the ASA’s economic and practice innovation agenda. This work includes ensuring that the interests of anesthesiologists in regulatory affairs are well represented as they intersect with payment and practice management issues. Ms. Fischoff leads the promotional, educational and advocacy efforts for the perioperative surgical home initiative. She also serves as a catalyst for product and service innovation to support ASA members engaged in redefining the future of the specialty. She can be reached at
Roseanne M. Fischoff, MPP, serves as the Economics and Practice Innovations Executive for the American Society of Anesthesiologists (ASA). In this role, Ms. Fischoff develops and implements policies and operating structure to advance the ASA’s economic and practice innovation agenda. This work includes ensuring that the interests of anesthesiologists in regulatory affairs are well represented as they intersect with payment and practice management issues. Ms. Fischoff leads the promotional, educational and advocacy efforts for the perioperative surgical home initiative. She also serves as a catalyst for product and service innovation to support ASA members engaged in redefining the future of the specialty. She can be reached at