eAlerts
-
WHAT MAKES FOR SUCCESS IN AN ANESTHESIA PRACTICE?

In our competitive society we all want to know how we are doing. Few of us are so confident in our endeavors as to not want some kind of feedback or approbation, especially those of us in the service business. The challenge is knowing what sources to trust. Too often, ulterior motives or our own naiveté cloud reality, making it hard to distinguish the important from the trivial. How often do we only hear what we want to hear? At least in our business we have some objective measures of success. So long as we keep growing and our clients maintain their franchises we are happy. The question is, what makes for success in an anesthesia practice? The persistent dissonance and drone of life in the operating room tends to dull one's senses to everything but the matter at hand. When the case goes well all is right with the world, or so it seems. How often, though, is the rising tide a harbinger of a major storm? Perhaps more often than most of us would care to admit.
Our clients used to obsess about their collections. A good month was defined simply in terms of a high deposit. Heaven forbid we came in below expectations, though. Little did I know that those were the good old days! Now, we are all so focused on the underlying factors that generate those collections that the actual numbers on the reports are almost anticlimactic. The world of anesthesia practice management has definitely evolved from its cash-based accounting roots to an accrual-based model of cost accounting. Sometimes I feel like a stockbroker: even a hint of bad news can send clients in paroxysms of anxiety. Disaster seems ever-present. As an organization we spend more time than ever helping our clients formulate strategies that will turn adversity into opportunity.
The entire vocabulary of practice management has changed in the past few years. Discussions of gross and net collections rates have given way to talk of manpower and staffing models. We hear much more about productivity and benchmarking than we do about Accounts Receivable management performance. But if there is one topic which defines the new era by virtue of its novelty and lack of understanding; it is customer service. As each topic unfolds across the country it is ever more clear that we must all be constantly updating our toolset if we want to succeed and thrive in the years ahead. As always, we hope you find our authors' treatment of these new frontier topics timely and informative. We go to great lengths to tap into those industry observers who we believe have their fingers on the pulse of the market. May you find ways to put these invaluable ideas to effective use in your practice!
Tony Mira,
President & CEO -
Customer Service - Get It Yourself!
Jerry Ippolito
Vice President & Principal, The Surgery Management Improvement Group, Inc.Customer Service - Get it yourself!
That was the headline in last Sunday's paper here in my Southwest Florida community. This community is burgeoning with population growth and still recovering from last year's hurricanes. There are not enough workers to meet the demand and any breathing creature can obtain a job in the service and construction industry - but what is the work ethic and professionalism of that worker? Customer service - let's look at our everyday lives. Whether booking a hotel reservation, questioning a bill, trying to get the TV-cable repaired, or working with your bank - just think of how difficult it is to speak to a person - typically the "customer" the guy who's spending the money with the option of taking business elsewhere, is directed to voice-mail; hears, "push one for this" ;"push two for that" ; or best yet, must pay additional fees to speak to a person - How Do You Feel, When You the Customer are Treated That Way?
In healthcare we speak a lot about "the customer and providing customer service" . Several of my hospital clients have "Customer Relations Specialists" - I think these individuals are intended to assist patients with service related issues, however I've never really been able to understand what these specialists really do. In other instances, my hospital clients have "Physician Liaisons" - these individuals are intended to assist physicians based at a hospital with service related issues. Humorous as it may seem, as an anesthesiologist have you ever been approached by the Physician Liaison at your hospital and asked,"how are we doing" - probably not. However in my world of Operating Room Management Consulting I do encourage OR Team Leaders and Directors of Surgical Services to take on that duty -"how are we doing?" . The phenomena however is that we talk a lot about customer service and we have customer service specialists of every species, BUT HAVE WE DEFINED WHO THE CUSTOMER IS? According to Webster the customer is:
- one who purchases a commodity;
- one with expectations of outcomes.
Some years ago I participated in a CQI (Continuous Quality Improvement) program where the second definition was more commonly used; in fact the second definition, in my mind, is the most appropriate. We all have needs and rely on performance and fulfillment of expectations by others - WE ARE ALL EACH OTHER'S CUSTOMERS.
In the world of the operating room we typically regard the surgeon as the customer. Ironic as it is, we seldom consider the patient first. As a consultant I have the opportunity to work with several dozen hospitals each year in many communities around the country - indeed the patient is the primary customer (even more ironic in today's world is that the payor is beginning to usurp this position). As I sit in restaurants, ride on planes, read local papers I'll continuously hear / read about residents' perceptions of the local hospital. I've had the honor of working with several very prestigious community medical centers around the country; if physicians are not on staff at these centers, they can not build or sustain a practice - if they are not on staff at these centers,they are not considered quality doctors - THE PATIENT IS HIGHLY SELECTIVE, and rightfully so!
In the world of OR we often speak of the three or four legged stool - the four customers; the four constituencies with expectations; even here we forget about the patient - aren't there really at least five customers:
- Patient - Expectations of: Quality care; Hospitality; Affordability; Accessibility
- Hospital Administration - Expectations of: Increased business; Increased Margins; Decreased Costs; Maximized utilization of resources
- OR Staff / Nursing - Expectations of: Ability to deliver quality patient care; Competitive compensation; Reasonable working conditions; Job satisfaction; Reliable and predictable workschedules
- Surgeons - Expectations of: Quality patient care; Sufficient OR access to meet practice needs; Maximized / efficient use of time; Experienced OR staff who can anticipate case needs; Equipment and technology meeting procedural needs; Ability to generate a livelihood comparable to similar specialists
- Anesthesiologists - Expectations of: Quality patient care; Optimized utilization of time; Competitive compensation and lifestyle; Predictability of schedules.
If any one customer's or constituent's expectations are fully satisfied (the 100 percent level) then fulfillment of other's expectations will suffer.
I hope we're now all agreed that the patient belongs in the center of our universe as professionals in the field of healthcare. Let's move on to the "nuts-and-bolts" of developing customer satisfaction in the OR. Let's first talk about the surgeon as we always hear that the surgeon is the customer. Typically the surgeon (or medical staff in general) wants to be regarded as a patron or customer of the hospital; the customer maintains the option to shop elsewhere. The hospital-business will not survive without the physician (and patient) customer(s). As in the retail environment the physician-customer maintains an expectation that the vendor (hospital) delivers a quality product. However, unique to the hospital setting is that the product is truly a service vs. a tangible product; physician-customers place primary emphasis on the hospital meeting their service oriented expectations. Physician-customers typically "Want what they want, when they want it" . The physician customer typically forgets that even in the most service oriented, traditional environment (whether Ritz Carlton, Nieman Marcus or Lexus dealership) hours of operation, dress codes, pricing strategies, rules of conduct, (etc.) exist and are required to effectively and reliably meet the majority of customers' expectations. Too frequently physicians / surgeons expect the administrative team (and anesthesiology) to meet 100 percent of expectations 100 percent of the time on terms established by the physician-customer at any given point in time. This mind-set, if allowed, diminishes the ability to optimize service to the other customers (patients, nursing, anesthesiology, administration). Compromise is key.
Now what you've been waiting for - does anesthesiology ever get to be the customer and what role does anesthesiology play in meeting customer service / satisfaction requirements? Surgeons will gravitate to those hospitals and ASCs where a superior level of anesthesiology care is provided - where there is choice. Patients are generally unaware of the level of care / expertise provided by the anesthesia service and really don't make decisions based on this factor. Doctors, I know this is going to hurt, but I now have to drop the bomb - in my nearly thirty years in healthcare and fourteen years in consulting, I can not site an instance where an anesthesiologist referred a case to a hospital (pain management or a personal referral aside). Indeed, quality anesthesiologists and CRNA (AA's) are in short supply these days and do have numerous job / practice opportunities, but typically anesthesiology's decision of where to "perform / take a case: requires a career and geographic move - very different from the surgeon's opportunities. Doctors, we just have to "bite-the-bullet" and deal with reality. I spend a sizeable amount of my time in consulting and interviewing anesthesiologists around the country and all too frequently I'll hear: "My income is decreasing because they (meaning hospital administration) have lost the outpatient business" . In polite terms I'll ask, "What role did anesthesiology play in retaining that business?" Generally I'll continue with the anesthesiologist and ask, "Do you consider yourself a consulting specialist? " Almost universally the anesthesiologist responds "Yes" - well then, don't consulting specialists need to garner referrals; develop and protect referral sources? It then begins to sink in. In the old days and still in some pockets of the country, anesthesiologists teamed up with surgeons and followed the surgeon all around town providing anesthesia for the surgeon's case. The surgeon was treated as a customer or client of the anesthesiologist; the anesthesiologist was expected to provide a certain level of service (I know I'm rubbing salt in the wound - sorry). Today the model has greatly changed and rightfully so due to the economics of healthcare - one surgeon's practice can not support an anesthesiologist at today's reimbursement levels. So then, the anesthesiologist, all the more, needs to expand and further develop the practice base - the anesthesiologist requires more clients / customers to generate the expected livelihood; the anesthesiologist needs to: "Market to the Customer; Build the Business".
As we wrap this up, let's focus on anesthesia's role in customer service in the operating room as well as anesthesia's position as a customer. In general, customers' expectations, regardless of who the customer is, will not be met unless expectations are reasonable and clearly defined. Most frequently for anesthesia this is defining how many sites are staffed by hour of day and day of week; this CAN NOT be a moving target if customer service is to be effectively delivered. Only as a few examples, as a customer, anesthesia should be able to rely on:
- Development of clearly defined and agreed to expectations with regard to sites staffed;
- Competitive compensation and lifestyle for services rendered delivering to expectations (potentially requiring a hospital stipend);
- An OR committee (or governance body) having developed effective scheduling policies and procedures and further, consistently enforcing them;
- Surgeons' offices effectively communicating with OR scheduling;
- Surgeons effectively communicating with anesthesia with regard to difficult cases or sick patients;
- Nursing effectively implementing preadmission screening protocols that have been developed jointly with anesthesia;
- Charts being complete on the day of surgery;
- Patients being appropriately prepared for surgery in either a Day-surgery unit or on the hospital floor;
- Ability to transport the patient to the OR in a timely manner in order to have on-time case starts;
- Surgeons reporting to the OR on time for on-time case starts;
- Experienced OR staff and appropriately set-up cases in order to reduce case times;
- Experienced charge nurses working with anesthesia to run the day's schedule;
- Experienced PACU staff who can function with relative independence;
- Lots of other stuff...
In providing customer services anesthesia should be expected to:
- Be current in state-of-the art anesthesia care with an emphasis on ambulatory anesthesia;
- Maintain reasonable flexibility with regard to agreed expectations - maintain an attitude of meeting or exceeding expectations;
- Assure consistent and reliable staffing for all anesthesia sites agreed to;
- Collaborate with nursing to develop state-of-the-art preadmission guidelines; agree as a group to established guidelines;
- Screen all ASA III and above patients and visit with all inpatients prior to the day of surgery;
- Develop processes to administer anesthesia consults for the preadmission unit;
- Call patients on the evening prior to surgery;
- Be as familiar as possible with patients' conditions prior to the day of surgery;
- Review patient charts at least the day prior to surgery;
- Proactively work with nursing in schedule planning and management;
- Begin reviewing the schedule with nursing several days prior to surgery;
- Facilitate getting patients into the OR for on-time case starts;
- Facilitate expediting turnaround time;
- Maintain an effective medical direction model where CRNA direction is based on case complexity, patient acuity and CRNA skill level;
- Be promptly available to CRNAs during on-going cases;
- Be promptly available to CRNAs cases to expedite induction and emergence;
- Develop a staffing model and service agreement model whereby anesthesia staffing requirements of OR-peripheral sites does not disrupt OR staffing;
- Develop a Q/I and education model for all anesthesiologists, CRNAs and hospital staff (RNs; RTs) where appropriate;
- Assign lead individuals to foster skills and business development in key services such as cardiac / vascular,OB, ambulatory, pain (potentially neuro, trauma, pediatrics);
- Play a key role in developing and sustaining YOUR OWN BUSINESS by focusing on what is required to develop a marketable and financially viable surgical program with increasing case volume;
- Focus on delivering the highest level of patient care with respect for the patient's time; provide hospitality; Focus on defining expectations and then exceeding those client / customer expectations and your business / anesthesia practice will flourish(1).
(1)Depending on expectations, payor mix and OR efficiencies / case times there may always be a need to approach hospital administration for a subsidy payment to deliver on expectations.
-
Assessing Operating Room Efficiency
Jody Locke
Vice President of Anesthesia and Pain Management Services, ABCThe measurement of operating room efficiency used to be one of those arcane sciences reserved for a special breed of consultant with experience in balancing the political and practical requirements of the daily management of a suite of operating rooms, but not any more. Given the impact of inefficient operating room management on anesthesia coverage and call requirements, O.R. utilization is rapidly becoming a key factor in an anesthesia practice’s need for financial support. While the causes of inefficient operating room utilization tend to be complex and directly related to a hospital’s need to compete for surgeon allegiance in increasingly competitive markets, it is not uncommon for anesthesiologists to be invited to join the fray. The concept of an anesthesiologist or an anesthesia department designee playing some role in O.R. management is not new. Many practices have had a “floor person,” “Clinical Day Director,” or “Captain of the Ship” for years. Typically, these have been ombudsmen providing a customer service rather than aggressive managers empowered to actively modify surgeon behavior. The problem is simply that for all their experience in the arena, most anesthesiologists have yet to develop the necessary tools and strategies to make them effective agents of change.
From an anesthesia perspective all discussions of operating efficiency ultimately hinge on the economics of coverage and call. This takes some overeager practitioners right to a discussion of profitability. From a management perspective, however, an exploration of benchmarks and metrics may be more useful in the strategic positioning of anesthesia as a contributor to the solution of declining productivity. Establishing a common vocabulary of performance utilization is deceptively complex. It is not uncommon to hospital administrations to view any data from the anesthesia practice with a healthy dose of skepticism. As in so many exercises in change, management time must be spent educating all the stakeholders so that they agree on the problem, accept the metrics and share some ownership for the process.
Most observers would agree all metrics should be viewed and tabulated by anesthetizing location. Let us further assume,for the sake of this discussion,that an anesthetizing location is an actual or virtual location that requires dedicated anesthesia personnel for part or all of a 24 hour period. By this definition each operating room is an anesthetizing location, as is the delivery suite, the Cystoscopy room, or any other physical space where anesthesia services might be required. The definition becomes a little less clear when the dedicated personnel are required to provide a variety of non-operating room services. Each practice must work through its own definition of N.O.R.A. (Non-Operating Room Anesthesia) requirements.
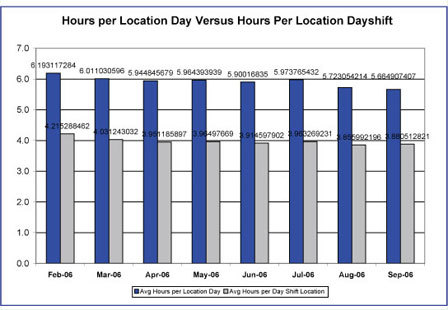
One school views operating room efficiency through the absolute lens of a particular metric such as cases, units or minutes per anesthetizing location day. There is considerable discussion across the country as to appropriate points of reference. There is some data to support an optimal number of cases per location day, but as even the most casual observer of the specialty will note not all cases are of equal acuity or duration. Others prefer to focus on total ASA units billed per location per day (base, time, modifier and incidental units) and will site the magic number 50 as an ideal productivity benchmark. Still others prefer to measure and monitor minutes. Actual anesthesia time has the advantage of corresponding, more or less, to the operating room time captured by the hospital staff. Discussions of anesthesia time can take a number of directions depending upon how important it is to identify when activity occurs. It has been suggested that an operating room that generates 6 hours of anesthesia time between 7 AM and 3 PM is running at optimum efficiency. Obviously, all benchmarks and standards must be adjusted to meet the particular requirements and challenges of the facility.
Proponents of such metrics argue that while they may not be a perfect measurement of every situation at least they provide a consistent frame of reference. They lend themselves to an objective comparison of facilities. An operating room that consistently generates 40 ASA units per location day is clearly less efficient than one that generates 50 or more units.
Inevitably, the question arises: Which metric is best? “Best” is a relative term because all valid data has some value if it is applied judiciously. A determination of the most appropriate metric or approach for a particular setting should hinge on two separate issues: reliability and credibility. Many anesthesiologists put great stock in measuring total ASA units per location day, because they know how they get paid for anesthesia, but such an approach may be viewed with great suspicion by hospital administrators who do not understand how anesthesia basic values and time units are determined. In other words, if a particular metric does not serve the goal of providing common coinage for a discussion of management options it will serve no practical purpose.
Another school of thought is more concerned with the relationship between coverage commitments and actual production patterns. In this variation on the theme actual hours of anesthesia time are divided by total hours of staff coverage. Such an approach factors in such issues as call and distinctions between short and long rooms. The advantage of such a perspective is that it can be customized to any particular configuration of anesthetizing locations. The disadvantage is that all applications become relative.
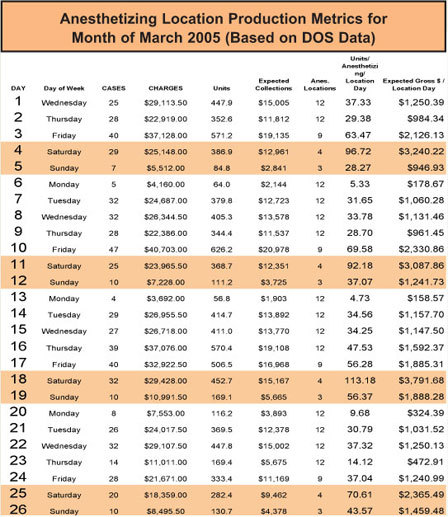
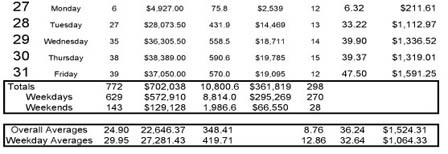
Included below are examples of each of the two approaches to the measuring of operating room productivity. Not every anesthesia practice will want to develop the tools to generate such reports, although more practices should probably be exploring the possibilities than are currently doing so because too often it is the initiation of a serious subsidy discussion that triggers the need to look at productivity. Practices that have been monitoring O.R. metrics over time have much greater conversance with their applicability and relevance. The fact is that as is true of the administration of anesthesia, it is difficult to manage what one does not measure. While anesthesia practices have traditionally focused on the measurement and management of billings and collections, more and more are beginning to realize that the one piece of the equation they did not choose to monitor is the one that has the greatest impact on the income and lifestyle of the members.
It has been said that you cannot manage what you do not measure. Anesthesiologists know this intuitively, because the availability of reliable physiologic data about a patient’s response to the trauma of surgery and anesthesia plays such a critical role in the consistent outcomes of today’s practitioners. The converse is also true: what you do not measure, you cannot manage. Anecdotal discussions tend not to support serious change. If O.R. productivity is an issue for your practice then an investment in the tools and resources to capture the data and monitor it closely is a small price to pay for the opportunity to be part of the solution rather than a victim of the problem.
-
Surgeon Satisfaction: A 360 Degree Perspective
Hugh Morgan
CMPE Director, AtlantiCare AnesthesiologyWhy has surgeon satisfaction become as important to health care leaders as clinical and financial outcomes? Each year, health care facilities throughout the world spend hundreds of thousands of dollars on surgeon satisfaction surveys in an attempt to arrive at the elusive answers to what truly satisfies a surgeon? The thought being that if the surgeon is satisfied, then the patient will be satisfied and business will be good. Practically every American industry, to include healthcare and business, is brimming with thousands of articles, theories and studies about the critical importance of customer satisfaction in steering organizational success. The dilemma is that the act of satisfying is in as much a subjective action as it is a subjective assessment. To satisfy, and in turn be satisfied, is a personal perspective that can typically be shared and appreciated, but likely not universally scripted and accepted. In many ways, customer satisfaction follows the simple Golden Rule; treat others as you want to be treated.
Where the customer satisfaction waters in the health care have become muddied is that the traditional customer (the patient) has joined an ever growing list of customer stakeholders to include the community, hospital administration and surgeons. Our challenge isn’t in understanding and accepting the ideas and principles of customer satisfaction, but rather in defining who we are supposed to satisfy? In recent years, a great deal of customer satisfaction endeavors in health care have been focused around the surgeons or the “revenue producing” customers. The shift in health care from patient-centric satisfaction to what I would refer to as “macro” satisfaction has placed operational burdens and unjust expectations on the specialty of anesthesiology. The industry is strewn with defeated anesthesiology groups who often times are forced to succumb to administratively supported surgical expectations. How then is it possible for an anesthesiology practice to survive and thrive in an era of surgeon-centric satisfaction?
First and foremost, an anesthesiology practice must define the diverse satisfaction stakeholders for who they are responsible to include patients, nursing, administration and surgeons. The group should seek to understand both the common and unique expectations of each stakeholder group through personal meetings and feedback surveys which ultimately produce the satisfaction criteria and goals. Although hard to believe, patient’s seem to have become the least arduous to satisfy. Typically, patient’s simply expect to be treated with compassion and respect and to receive the highest quality and safest medical care with the best possible outcome. Administration is a little more challenging to satisfy in that they usually expect anesthesiology practices to infallibly provide anesthesia services and meet fluctuating clinical coverage requirements without pause or cancellation and within the most financially insolvent manner possible. Fairly straightforward expectations, right? The quandary is that administration’s satisfaction expectations are often directly associated, if not embedded, with that of surgeon satisfaction expectations resulting in a tag-team of operational and financial burdens for an anesthesiology practice. The key is to concurrently address the administrative and surgical satisfaction expectations so that there is a clear understanding by each stakeholder as to how satisfaction expectations can directly impact anesthesiology’s ability to effectively satisfy at the expense of group operations. It is essential to arrive at a set of reasonable, achievable and mutually beneficial administrative and surgical expectations so that the satisfaction criteria are universally known and not subject to whimsical modifications. Although some satisfaction expectations are somewhat broad and inherently subjective such as, “adequate coverage” and “immediately available” it is usually more evident to notice and hear about the absence rather than the presence of satisfaction. How often have we heard that if all is quiet, things must be good?
An important facet in achieving surgeon satisfaction is the ability of an anesthesiology practice to be duly recognized by administration and surgeons as medical colleagues of the surgical staff. Too often, anesthesiology is viewed as a hospital “service” and not as a medical practice with a critical role in the overall safety and care of the patient. Although anesthesiology touches numerous clinical environments throughout a hospital, perhaps the most important and visible involvement is within the Perioperative arena. From the preoperative assessment through post surgical recovery, anesthesiology plays a vital role in the customer satisfaction of the various perioperative stakeholders, most notably the surgeons. Anesthesiology is the third cog, the others being nursing and surgery, in the wheel that effectively spins perioperative/surgical services. Like a tire, if any one of these preoperative”cogs” experiences problems, the tire goes flat and unfortunate accidents can occur. It is important then for each of the preoperative disciplines to be accountable to each other for a variety of satisfaction criteria to include patient safety, clinical competency, professional behavior and workflow efficiencies. The challenge is to develop the mutual perioperative satisfaction criteria and measurement tool for which each of the perioperative disciplines will be accountable and to encourage global participation as a means to achieving higher levels of performance and satisfaction.
Earlier this year, with input from my perioperative leadership colleagues at AtlantiCare, I initiated the development of a 360 degree Perioperative Satisfaction Survey to purposefully achieve higher levels of mutual perioperative satisfaction and drive higher levels of perioperative performance. The 360 degree approach for survey and evaluation purposes is not a new concept as business leaders have successfully used 360 surveys as a means of assessing leadership at every organizational level. Although surgeon specific satisfaction surveys had previously been attempted at AtlantiCare, the thought was that a comprehensive 360 degree survey would likely surface common satisfaction and dissatisfaction themes affecting all of the perioperative disciplines to include the surgeons. The intent was to obtain definitive feedback on the common satisfaction and dissatisfaction themes so that the leadership of each perioperative discipline could address the universal issues of the discipline rather than issues of isolated dissatisfaction. A set of mutually inclusive satisfaction criteria with basic effective scoring was developed and scoring that fell above or below acceptable targets required supportive elaboration so that dissatisfaction could be effectively addressed. The leaders of each perioperative discipline were tasked with distributing the 360 degree survey to their respective colleagues. Each perioperative discipline had the opportunity to survey each of the other disciplines as well as their own discipline. As with any feedback survey, it was important to establish deadlines for survey submission dates so that feedback is timely and action plans for improvement can be efficiently developed. The survey success is completely dependant on the level of participation or you will have developed the best satisfaction survey with no feedback to improve satisfaction or
performance.The key point is that to achieve higher levels of surgeon satisfaction is to concurrently achieve higher levels of nursing and anesthesiology satisfaction. Within the perioperative arena,none of the disciplines can achieve high levels of satisfaction without the other disciplines also being effectively satisfied. It comes down to a mutual respect and understanding of the critical roles that each discipline plays in determining the performance, culture and overall success of perioperative and surgical services. In the end, it becomes an exercise in futility to attempt to satisfy one discipline, namely surgeons, at the expense of the other two perioperative disciplines, nursing and anesthesiology.
-
Compliance Auditing: How Many Records Should You Review?Abby Pendleton
Wachler & Associates, P.C.As part of our desire to keep both clients and readers up to date, the Communiqué has been printing compliance information since its inception. In the Compliance Corner, we will now formally keep you abreast of the various compliance issues and/or pick out a topic that would be of interest to most of our readers.
Since the publication of the OIG Compliance Guidance for Individual and Small Group Physician Practices (hereinafter the “OIG Guidance”) in 2000, many anesthesia practices have had some experience with compliance auditing. The first of the seven compliance program elements recommended by the OIG is conducting internal monitoring and auditing through the performance of periodic audits. What does this entail for an anesthesia practice? Although physicians may not be legally required to conduct internal audits and the fact remains that the OIG Guidance is only a set of recommendations, many experts recommend that physician practices should strive to conduct internal auditing at least on an annual basis. Conducting annual audits should prove beneficial in assisting the practice in identifying issues that should be addressed or corrected thereby reducing ongoing risks to the practice. By performing an audit on at least an annual basis, the practice should avoid messy situations such as identifying a significant problem or issue that may have been occurring for a significant time period resulting in potential large overpayments received by the practice. Such circumstances can raise significant questions for the practice related to payback and disclosure obligations.
A common question facing anesthesia practices when deciding to conduct an internal audit (either by internal staff or hiring an outside consulting group) is “how many records should we review?” While there is no exact right or wrong number, it is reasonable for the practice to limit the record review to a manageable and practical number for several reasons including costs. In the OIG Guidance, the OIG suggests that an appropriate sample size may be five (5) to ten (10) records per physician in the practice. In many situations, a group’s decision to audit between 5 and 10 records per physician would be reasonable. Some outside consultants that have an economic interest in reviewing many records, may suggest too large of a sample size. The practice must keep this in mind when hiring and coordinating an audit with outside help. Outside consultants can and do provide valuable assistance and expertise for many practices, however, the practice should maintain control of the process and not simply allow the consultants to direct and select the sample size. Given that the auditors will typically identify problem areas, it is also important for the practice to conduct the internal audit under the attorney/client privilege. This process is not complicated and involves the practice’s attorney directing the auditors to perform the audit under the attorney/client privilege.
In addition to the cost issues, if the goal of the audit is early identification of issues or patterns, a large volume of records is typically not necessary. In fact, many auditors will begin to identify issues/patterns in the first 10 to 20 records. For example, in auditing anesthesia records, it usually does not take many records to identify whether the physicians are fully documenting medical direction requirements or whether anesthesia time is being rounded. In the anesthesia setting, many auditors suggest a review of a full day of cases in order to perform a concurrency review in connection with the audit. The practice will have to make a determination as to whether an independent check of concurrency is necessary.
Accordingly, while there may not be one “magic” number for compliance auditing, your practice should take a reasonable approach by selecting enough records to accomplish the goal of the audit, which in many routine compliance audit situations is to identify areas needing attention. For many practices, selecting a minimum of 5 records per physician will accomplish this goal. Of course, once issues are identified, the practice should perform specific focused follow-up audits to oversee that corrective action measures that were put into place (e.g., educating providers or establishing new policies) are working.







 performance.
performance.
