Are You Ready for ICD–10?
Joette Derricks, CPC, CHC, CMPE, CSSGB
Vice President of Regulatory Affairs & Research, ABC
On October 1, 2014, the United States health care system will undergo a major transformation. We will transition from the decades-old Ninth Edition of the International Classification of Diseases (ICD-9) set of diagnosis and inpatient procedure codes to the Tenth Edition of those code sets—or ICD-10. The Tenth Edition is the version currently used by most developed countries throughout the world. ICD-10 allows for greater specificity and detail in describing a patient’s diagnosis and in classifying inpatient procedures, so reimbursement can better reflect the intensity of the patient’s condition and diagnostic needs.
This transition will have a major impact on anyone who uses health care information that contains a diagnosis and/or inpatient procedure code, including hospitals, physicians, other providers, payers, clearinghouses, billing companies, etc.
The change will affect all covered entities as defined by the Health Insurance Portability and Accountability Act of 1996 (HIPAA). Covered entities are required to adopt ICD-10 codes for services provided on or after the October 1, 2014 compliance date. For inpatient claims, ICD-10 diagnosis and procedure codes are required for all stays with discharge dates on or after October 1, 2014.
 Note that the transition to ICD-10 does not directly affect provider use of the Current Procedural Terminology (CPT) and Healthcare Common Procedure Coding System (HCPCS) codes.
Note that the transition to ICD-10 does not directly affect provider use of the Current Procedural Terminology (CPT) and Healthcare Common Procedure Coding System (HCPCS) codes.
About ICD–10
The World Health Organization (WHO) publishes the International Classification of Diseases code set, which defines diseases, signs, symptoms, abnormal findings, complaints, social circumstances, and external causes of injury or disease. The ICD-10 is copyrighted by the WHO (http://www.who.int/whosis/icd10/index.html). The WHO authorized a U.S. adaptation of the code set for government purposes. As agreed, all modifications to the ICD-10 must conform to WHO conventions for the ICD. Currently, the United States uses the ICD code set, Ninth Edition (ICD-9), originally published in 1977, and adopted by this country in 1979 as a system for classification of morbidity data and subsequently mandated as the Medicare claims standard in 1989 in the following forms:
- ICD-9-CM (Volume 1), the tabular index of diagnostic codes
- ICD-9-CM (Volume 2), the alphabetical index of diagnostic codes
- ICD-9-CM (Volume 3), institutional procedure codes used only in inpatient hospital settings
In 1990, the WHO updated its international version of the ICD code set for mortality reporting. Other countries began adopting ICD-10 in 1994, but the United States only partially adopted ICD-10 in 1999 for mortality reporting.
The National Center for Health Statistics (NCHS), the federal agency responsible for the United States’ use of ICD-10 developed ICD-10-CM, a clinical modification of the classification for morbidity reporting purposes, to replace our ICD-9-CM Codes, Volumes 1 and 2. The NCHS developed ICD-10-CM following a thorough evaluation by a technical advisory panel and extensive consultation with physician groups, clinical coders, and others to ensure clinical accuracy and usefulness.
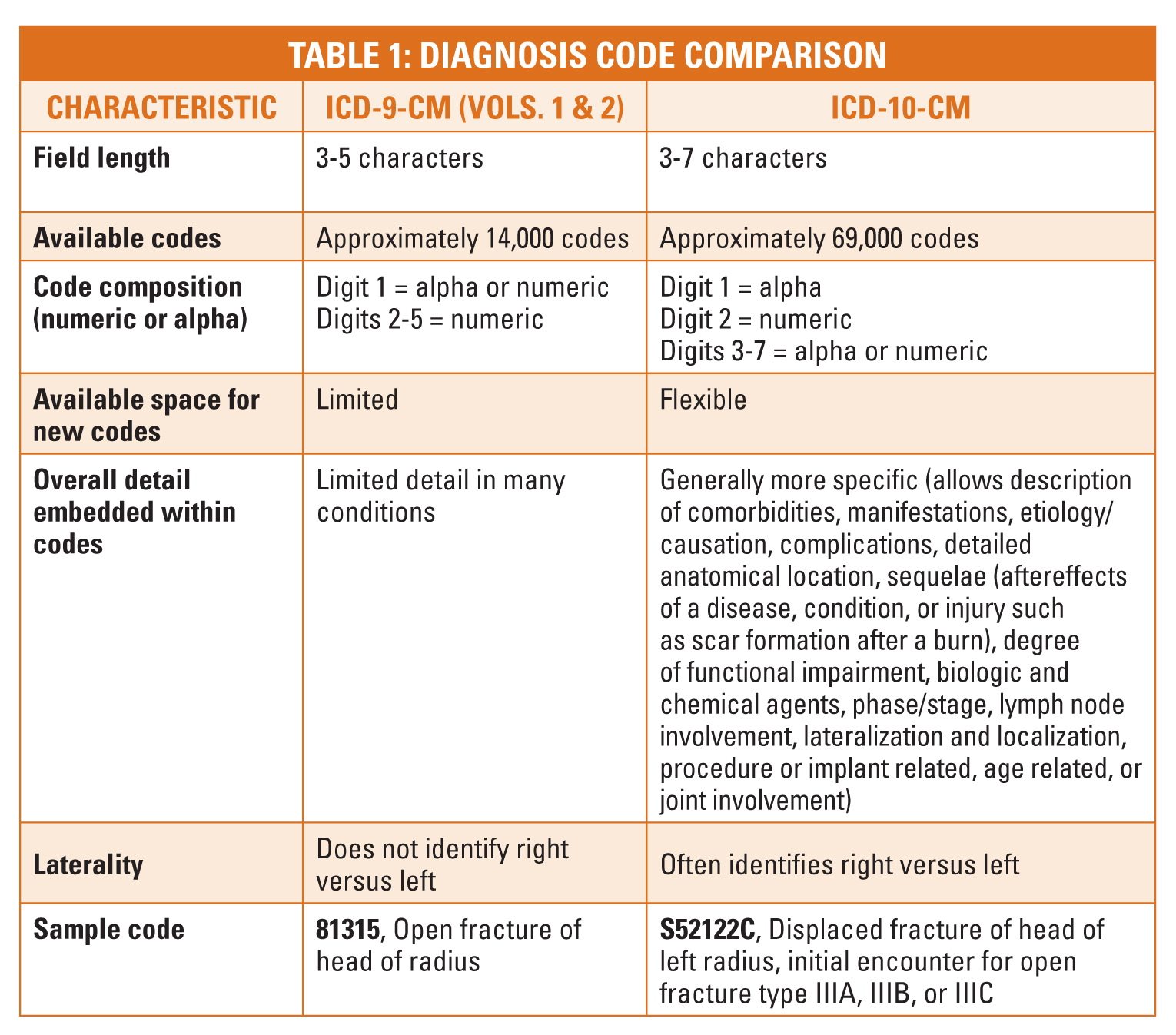
How Do ICD–9 and ICD–10 Differ?
There are several structural differences between ICD-9-CM codes and ICD-10 codes1. Table 1 below illustrates the difference between ICD-9-CM (Volumes 1 and 2) and ICD-10-CM.
ICD-10-CM/PCS consists of two parts:
- ICD-10-CM for diagnosis coding in all health care settings
- ICD-10-PCS for inpatient procedure coding in hospital settings
 )
)
The General Equivalence Mappings (GEM) are a reference mapping that attempts to include all valid relationships between the codes in the ICD-9-CM diagnosis classification to the ICD-10-CM.
By moving to an expanding code system, ICD-10 will provide governmental agencies and payers with more specific data than ICD-9. This expanded data capability will aid in:
- Capturing Quality data
- Reducing coding errors
- Analyzing disease patterns
- Tracking and responding to public health outbreaks
- Identifying fraud and abuse
Preparing for the Transition
Most hospitals, physicians groups, payers, clearinghouses, and billing companies have been preparing for the transition for several years. The conversion to ICD-10 requires adequate planning, training of coders, billers and clinical providers, converting system programs, testing and developing backup contingency scenarios. In addition, every organization needs to assess their current workflow and processes to determine if and how the conversion to ICD-10 may impact production or service to patients. For example, the pre-authorization process generally requires diagnosis information. Hospitals and physician practices need to look at how that process works today in their organization and what may need to change.
 Talk to the users and examine all documents that in any way refer to or require diagnosis information. A few questions to ask include: Do the form(s) used to record the pre-authorization requests need to change? What level of training do the employees that handle the pre-authorization require? By assessing, questioning, communicating, training, revising and implementing new or different policies and procedures now you will minimize the potential risks that the Centers for Medicare & Medicaid Services (CMS) has identified. These include potential delays in payments, increased accounts receivable and higher denial rates.
Talk to the users and examine all documents that in any way refer to or require diagnosis information. A few questions to ask include: Do the form(s) used to record the pre-authorization requests need to change? What level of training do the employees that handle the pre-authorization require? By assessing, questioning, communicating, training, revising and implementing new or different policies and procedures now you will minimize the potential risks that the Centers for Medicare & Medicaid Services (CMS) has identified. These include potential delays in payments, increased accounts receivable and higher denial rates.
Since ICD-10 is more specific, research has shown that physicians may need to document differently to ensure that the medical record has sufficient information to allow coders to assign the ICD-10 code. Many hospitals and large physician groups are putting in place a clinical documentation improvement process (CDI) at this time to help communicate and educate physicians on what additional information may be required when the conversion to ICD-10 occurs. A CDI process requires the coder to examine the physician’s current documentation and identify whether it is or isn’t sufficient to allow an ICD-10 code to be identified. Feedback is then provided to the physician on what additional information should be incorporated into the medical record documentation going forward so when the transition occurs, the complete and accurate documentation will be available and thus the risk of delays or denials will be diminished. The additional documentation is information that the physician would know at the time of the service. It includes information such as location, laterality, type of visit (initial or subsequent), etc.
 Helpful Resources
Helpful Resources
 Helpful Resources
Helpful ResourcesThe CMS has a dedicated website with some excellent tools for hospitals and physician practices of all sizes. In addition, the American Medical Association (AMA), specialty associations, major health insurance payers and clearinghouses all have information on their websites to help providers with the transition. If you have not yet heard from your coding or billing department it may be beneficial to review some basic information and then reach out and see where your organization is in regards to the ICD-10 transition.
Following are some links to learn more:
http://cms.gov/Medicare/Coding/ICD10/index.html
http://www.cdc.gov/nchs/icd/icd10cm.htm
http://www.ahima.org/icd10/whatisicd10.aspx
Joette Derricks, CPC, CHC, CMPE, CSSGB serves as Vice President  of Regulatory Affairs and Research for ABC. She has 30+ years of healthcare financial management and business experience. Knowledgeable in third-party reimbursement, coding and compliance issues, Ms. Derricks works to ensure client operations are both productive and profitable. She is a long-standing member of MGMA, HCCA, AAPC and other associations. She is also a nationally-acclaimed speaker, having presented at AHIMA, Ingenix, MGMA and HCCA national conferences. You can reach her at Joette.Derricks@AnesthesiaLLC.com.
of Regulatory Affairs and Research for ABC. She has 30+ years of healthcare financial management and business experience. Knowledgeable in third-party reimbursement, coding and compliance issues, Ms. Derricks works to ensure client operations are both productive and profitable. She is a long-standing member of MGMA, HCCA, AAPC and other associations. She is also a nationally-acclaimed speaker, having presented at AHIMA, Ingenix, MGMA and HCCA national conferences. You can reach her at Joette.Derricks@AnesthesiaLLC.com.
References
1http://www.ama-assn.org/ama1/pub/upload/mm/399/ icd10-icd9-differences-fact-sheet.pdf