Reporting Postoperative Pain Management in 2014
Kelly D. Dennis, MBA, ACS-AN, CANPC, CHCA, CPC, CPC-I
Perfect Office Solutions, Inc., Palmetto, FL
According to Recent Advances in Postoperative Pain Management (Nalini), approximately eighty (80%) percent of patients experience postoperative (or acute) pain after surgery, and pain is one of the most common medical causes of delayed discharge after surgery. Although there have been major breakthroughs in postoperative pain management (POPM), many factors are considered before deciding on the type of pain therapy provided to surgical patients, including co-morbidities, psychological status, exposure to analgesic therapies, and the type of surgical procedure. Studies indicate postoperative pain is associated with, but not limited, to gynecological and orthopedic procedures and have found recovery is faster and fewer complications are experienced when the acute pain is treated aggressively. During the past twenty years, new technologies to aid postoperative pain control have gained widespread use. (Medscape)
Control of POPM is truly a team effort between the surgeon and the anesthesia provider. It is important for anesthesia coders to pay careful attention to changes regarding coding and documentation for POPM as changes may affect an anesthesia provider’s ability to bill separately for these services. Of note, there were a number of text changes in the National Correct Coding Initiative (NCCI), Anesthesia Services section found in Chapter II, Pages II-7 through II-12 in Version 18.0 (effective January 1, 2012) and Chapter II, Pages II-6 through II-15 in Version 19.0 (effective January 1, 2013). These changes outline under which circumstances acute pain management is payable and emphasize the requirement of documentation from the surgeon requesting assistance from an anesthesia provider. Further, a recent proposed draft Local Coverage Determination (LCD) by Noridian Administrative Services, LLC regarding POPM indicated “Providers should not expect separate payment for the establishment of epidural or other pain blocks unless the block is placed following discharge from PACU due to documented inadequate pain control.” As originally written, the Noridian LCD would have drastically changed the way anesthesia providers are paid for anesthesia services. Both the American Society of Anesthesiologists (ASA) and a number of anesthesiologists who serve on their state Carrier Advisory Committee (CAC) worked with Noridian to ensure they had a clear understanding of acute pain management services and the significant changes in the original language of the draft LCD before it became effective on 11/11/13. In the final version, Noridian outlines expected documentation for Medicare Part B as follows:
Reimbursement for the control or management of acute pain in the immediate postoperative period is generally packaged into the payment for the surgical procedure. However, if a need for transfer of pain management is documented and ordered by the surgeon and the accepting provider documents the need for and acceptance of transfer of care, separate reimbursement may be made for the service.
Presumably, both the NCCI changes and the Noridian LCD are based on the premise of the Centers for Medicare and Medicaid Services (CMS) Medicare Claim Processing Manual, Chapter 12— Physicians/Non-Physician Practitioners that postsurgical pain management by the surgeon is included in the global surgical package. However, the NCCI recognizes the ability of the surgeon to “request the assistance of the anesthesia practitioner if the degree of postoperative pain is expected to exceed the skills and experience of the operating physician to manage it.” NCCI also indicates POPM procedures may be “administered preoperatively, intraoperatively, or postoperatively.”
Although postoperative pain is the responsibility of the surgeon and payment is bundled into the surgeon’s global fee, anesthesia services may be reported separately if there is a request by the surgeon for an anesthesia practitioner to provide POPM and anesthesia for the surgical procedure is not dependent on the efficacy of the regional anesthetic technique. The ASA Relative Value Guide® (RVG™) indicates that the following conditions apply:
- Anesthesia for the surgical procedure was not dependent upon the efficacy of the regional anesthetic technique;
- Time spent on pre- or postoperative placement of the block is separated and not included in reported anesthetic time; and
- Time for a post surgical block that occurs after induction and prior to emergence does not need to be deducted from reported anesthesia time.
The RVG also suggests documenting the surgeon’s request, however, and according to the NCCI the “surgeon is responsible to document in the medical record the reason care is being referred to the anesthesia practitioner.” This provision requires a written request from the surgeon—which indicates there must be communication between anesthesia and surgical staff to ensure the requirements for POPM are well documented for each patient on a case-by-case basis.
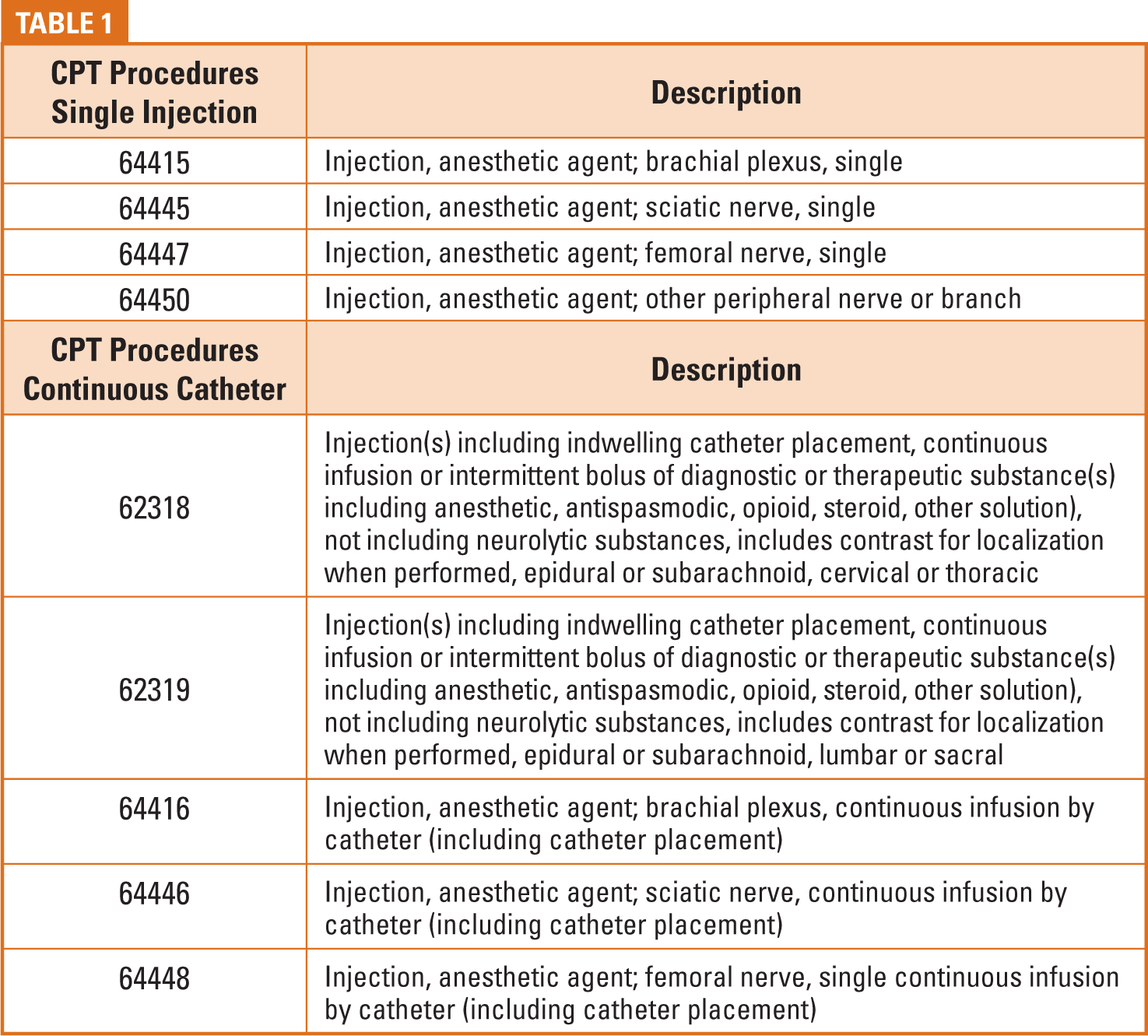
Procedure coding will depend on the site of the injection area and placement of either a block(s) or a continuous catheter. See Table I for some of the more common Current Procedural Terminology® (CPT) codes associated with POPM services. A -59 modifier should be appended to indicate that the service or services were distinct procedural services from the anesthesia provided for the surgery. Remember—if the block/catheter was used for the surgery the procedure is not separately billable, although discontinuous anesthesia time may be reported for the time spent placing the block/catheter. For example, if a carpal tunnel procedure is being performed with a wrist block, a code from the CPT anesthesia section (01810 + anesthesia time for both the anesthesia during the wrist surgery and time related to placing the wrist block) is reported. No separate code is reported for the wrist block.
Coders should check the documentation carefully and ensure they understand when POPM is separately reportable and that there is an understanding of the procedure being performed. For example, several terms are used to describe a “brachial plexus” block—such as “interscalene,” “infraclavicular” or “supraclavicular”— which should not be confused with codes with a similar sounding description (such as “suprascapular”). A “popliteal” block procedure note, without a description of the anatomy is not helpful in determining the correct code to report. A “popliteal fossa” injection is reported with CPT code 64445 (sciatic nerve), whereas a “saphenous popliteal” is reported with CPT code 64450 (other peripheral nerve block). Also, transversus abdominis plane (TAP) blocks do not have a specific procedure code. CPT code 64450 may be used; however, CPT code 64425 may be appropriate for TAP blocks performed for inguinal hernia repair when the ilioinguinal/iliohypogastric nerves are anesthetized. (Mariano) If coders are unclear about the services provided, they must confirm ALL questionable details!
If ultrasound guidance is utilized and appropriately documented, CPT code 76942 [Ultrasound guidance for needle placement (eg, biopsy, aspiration, injection, localization device), imaging supervision and interpretation] may be reported separately with a -26 modifier (if applicable). Documentation of the use of ultrasound alone is not sufficient —according to CPT Non-obstetrical ultrasound coding guidelines, “Use of ultrasound, without thorough evaluation of organ(s) or anatomic region, image documentation, and final, written report, is not separately reportable.” A retrievable image should be available, along with a procedure note describing the use of ultrasound for placement of the block. It is also important for anesthesia coders to remember that codes obtained from the surgery and radiology section are flat-fee and, although no time is reported separately, documentation must support the time the block was placed (i.e. 7:21 to 7:34) to clearly indicate that it was separate from the reported anesthesia time when applicable.
Reporting daily management of postoperative pain will vary, depending on the services provided. According to the NCCI, “CPT code 01996 may only be reported for management for days subsequent to the date of insertion of the epidural or subarachnoid catheter.” CPT 01996 would not be reported for other types of continuous catheters, such as CPT codes 64416, 64446, or 64448. Coders should determine whether the documentation supports an Evaluation and Management (E&M) service, including the chief complaint (related to postoperative pain) and at least two of the three required elements for subsequent hospital care (History, Examination, and Medical Decision Making). Keep in mind that if the surgeon has transferred responsibility for postoperative pain management to an anesthesia provider, only one physician or qualified healthcare professional should report these services.
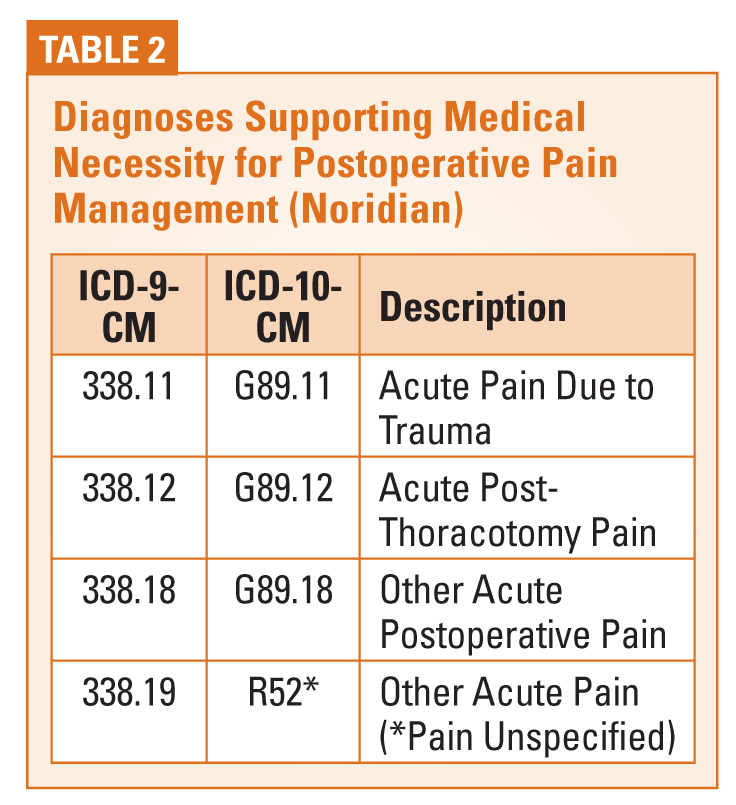
Acute pain diagnosis codes are separately identified in the 338 section of the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM), although there has been some confusion regarding reporting a diagnosis code from this section. According to ICD guidelines, “Routine or expected postoperative pain immediately after surgery should not be coded.” However, the guidelines also state that “If pain control/management is the reason for the encounter, a code from category 338 should be assigned as the principal or first-listed diagnosis” and “may be reported as the principal or first-listed diagnosis when the stated reason for the admission/encounter is documented as postoperative pain control/management”. As routine pain management is provided by the surgeon, it is my opinion a category 338 code should be reported when anesthesia is requested to provide POPM. Note in Table 2, published in the final Noridian LCD, category 338 is recognized in the list of ICD 9 codes that support medical necessity. Since ICD-10 isn’t too far away, the table has been updated to include these conversion codes.
Historically, anesthesia practices have relied on documentation by the anesthesia provider to support the surgeon’s request for POPM, such as a procedure note or anesthesia record indication of the surgeon’s request. In the current environment, coders rely on the documentation guidelines as outlined in the NCCI and the recommendations listed by the ASA. Documentation in the medical record must support the surgeon’s transfer of care and this requirement means that anesthesia practitioners should request written, rather than verbal, communication. According to Dr. Peter Dunbar, who serves on the Noridian CAC for Washington State, standing orders from surgeons will be acceptable as long as they are both surgeon and procedure specific.
Resources
American Society of Anesthesiologists (ASA) Relative Value Guide® (2013) Reporting Postoperative Pain Procedures in Conjunction with Anesthesia (Pages 58 – 65) http://www.asahq.org/For-Members/~/ media/For%20Members/Standards%20and%20Guidelines/2012/REPORTING%20POSTOPERATIVE%20PAIN%20PROCEDURES%20IN%20CONJUNCTION%20WITH%20ANESTHESIA.ashx
Centers for Medicare and Medicaid Services, Internet Only Manual (IOM), Chapter 12 http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf
Current Procedural Terminology®, Professional Edition (2013), American Medical Association
International Classification of Diseases, Ninth Revision,Clinical Modification (ICD-9-CM)® (2013)
Mariano, Ed (MD), Billing for Regional Anesthesia http://www.edmariano.com/billing-for-regional-anesthesiaMedscape
Medscape, CSI: Investigating Acute Postoperative Pain: Improved Outcomes and Clinical Horizons http://www.edmariano.com/billing-for-regional-anesthesiaMedscape
National Correct Coding Initiative, Chapter Two, Version 19.0, Anesthesia Services https://www.cms.gov/Medicare/Coding/NationalCorrectCodInitEd/ Downloads/NCCI_Policy_Manual.zip
Nalini V, Sukanya M, Deepak N, Recent advances in Postoperative pain management. Biology and Medicine. Yale J Biol Med. 2010; 83:11– 25 http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2844689/#!po=70.4545
Noridian Administrative Services, LLC, Proposed/Draft Local Coverage Determination (LCD): Nerve Blockade: Somatic, Selective Nerve Root, and Epidural (DL33188) http://www.cms.gov/medicare-coverage-database/license/cpt-license.aspx?from=~/overview-and-quick-search. aspx&npage=/medicare-coverage-database/details/lcd-details.aspx&LCDId=33187&ContrId=246&ver=4&ContrVer=1&CntrctrSelected=246*1&Cntrctr=246&name=Noridian+Administrative+Services%2c+LLC+(02102%2c+MAC+-+Part+B)&DocType=Proposed_NRTF&DocStatus=Draft&LCntrctr=83*1%7c242*1%7c246*1%7c241*1%7c245*1%7c243*1%7c248*1%7c244*1%7c247 *1%7c142*1%7c129*1%7c124*1%7c130*1%7c125*1%7c131*1%7c126*1%7c135*1%7c127*1%7c133*1%7c128*1%7c134*1&bc=AgACAAIAAAAAAA%3d%3d&
Noridian Administrative Services, LLC – Link to LCD L33188 from CMS website http://www.cms.gov/medicare-coverage-database/ details/lcd-details.aspx?LCDId=33188&ContrId=246&ver=10&ContrVer=2&Date=11%2f11%2f2013&DocID=L33188&SearchType=Advanced&bc=KAAAAAgAAAAAAA%3d%3d&
Kelly Dennis, MBA,ACS-AN, CANPC, CHCA, CPC, CPC-I has over 30 years experience in anesthesia and speaks about anesthesia issues nationally. She has a Master’s Degree in Business Administration, is certified through the American Academy of Professional Coders, is an Advanced Coding Specialist for the Board of Medical Specialty Coding and serves as lead advisor for their anesthesia board. She is also a certified health care auditor and has owned her own consulting company, Perfect Office Solutions, Inc., since November, 2001.