Strengthening Your Anesthesiology Group
Will Latham, MBA
President, Latham Consulting Group, Inc. Chattanooga, TN
“Most people choose unhappiness over uncertainty.” — Timothy Ferris
Anesthesiology groups are facing unprecedented challenges. How will the Affordable Care Act affect them? What will happen when ACOs get up and running? Should our group sell to an investment group? Should we pursue hospital employment?
These are truly uncertain times.
 Unfortunately many groups are in a reactive mode, struggling with how to deal with threats and opportunities in the marketplace. This is often because their governance and management processes were formed at a time when there were fewer stressors and challenges. Some group are sprinting towards relationships that appear to offer financial reward and some level of security, but at the same time have the potential to severely limit the group’s and the physician’s autonomy.
Unfortunately many groups are in a reactive mode, struggling with how to deal with threats and opportunities in the marketplace. This is often because their governance and management processes were formed at a time when there were fewer stressors and challenges. Some group are sprinting towards relationships that appear to offer financial reward and some level of security, but at the same time have the potential to severely limit the group’s and the physician’s autonomy.
While there are situations where employment may be appropriate, many groups that pursue this course are “choosing unhappiness over uncertainty.”
If your group intends to remain independent, or if you are independent now and are still trying to decide which long-term option to choose, there are two steps that you can do to reduce uncertainty. You can’t eliminate the environment threats, but you can significantly strengthen your organization’s ability to cope with such threats.
Strengthen Group Governance
The first step is to strengthen your group’s governance. You can find a number of resources to help you do this on our website at www.lathamconsulting.com (choose “Resources” and then “Special Reports”), including Special Reports on:
- Practical Governance for Medical Groups
- Characteristics of Effective Boards
- A Code of Conduct Improves Behavior
However, many groups have never established even basic agreements about how they will decide things and govern their practice. Many groups still suffer from what we call “the dirty little secret.” This “secret” goes like this—once decisions have been made by the group, many physicians believe that supporting the decision is optional depending on whether or not they like the decision. If they didn’t vote for it, they feel like they don’t have to do it, support it or adhere to it!
As you may have already discovered, this can prevent a group from moving forward on important decisions and initiatives.
How can the group improve its ability to make and stick to decisions? Group members must ask themselves three fundamental questions. We believe these are the most important questions that any group can ask itself:
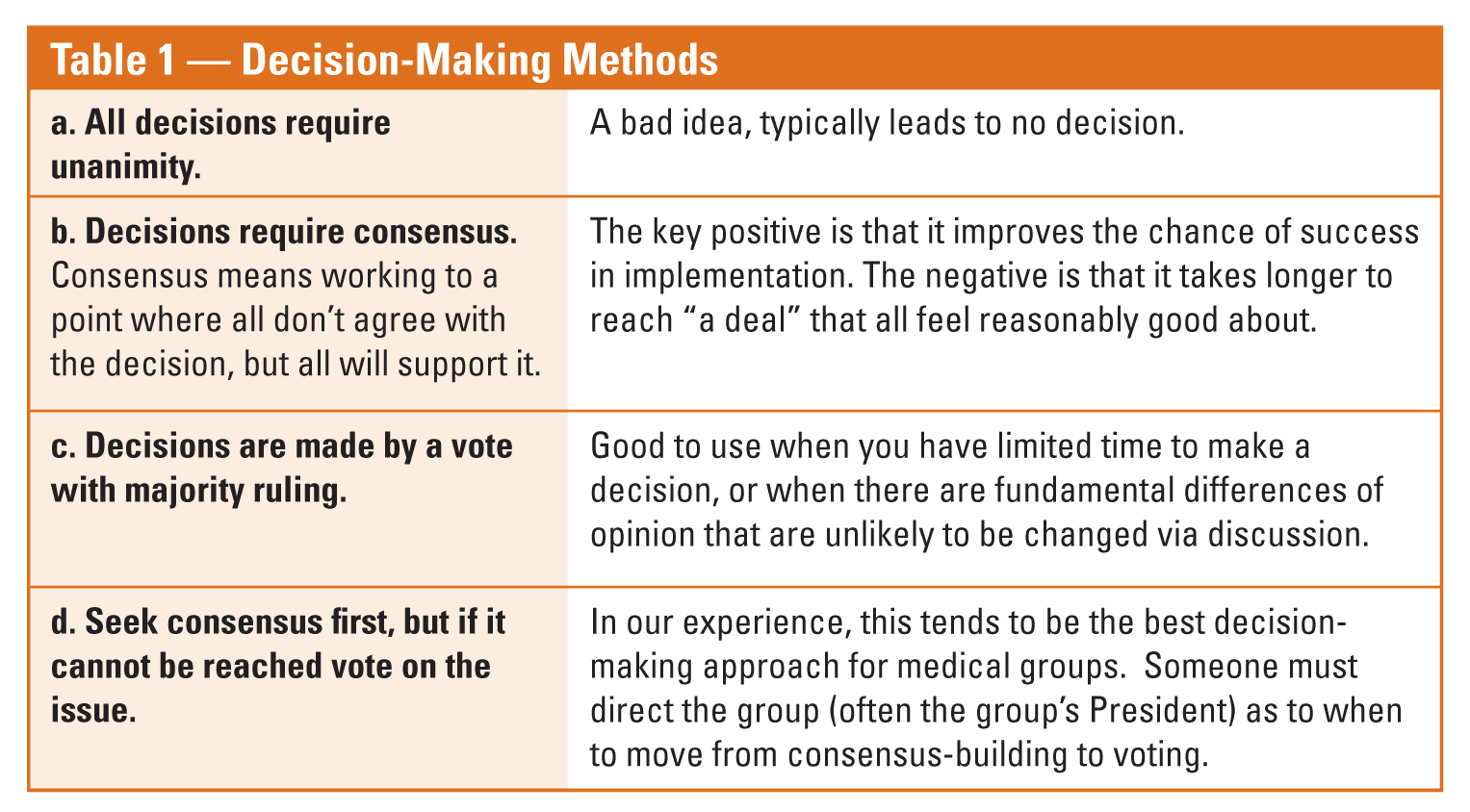
- How will the group make decisions? It is critical that the group agree on how it will make decisions. Typically the group has four choices as outlined in Table 1. In our experience, the best option is to seek consensus first, and then vote if consensus cannot be reached. Often the president is charged with the responsibility of determining when the group should move to vote.
- What is expected of each physician once a decision has been made? This is the crucial question. The best groups answer this question by agreeing that once a decision has been made in the agreed-upon decision-making method, every physician (whether they agreed with the decision or not) will actively and fully support the decision, to include encouraging others to support the decision. “Fully support” means doing what they have agreed to, actively promoting implementation, and not sabotaging the decision.
- What are a physician’s options if he or she still doesn’t like the decision? There should be only three options:
- Do it anyway—that’s group practice.
- Try to get it changed in the appropriate forum, but keep adhering to the decision until it is changed.
- Self-select yourself out of the group.
This last option is the one that causes people heartburn, but without it people will believe they have the option to stay with the group while not adhering to group decisions.
We know that it is unrealistic to believe that all physicians will adhere to the commitment to leave the practice if they don’t adhere to group decisions. However, by asking and answering these questions, the group can remind outliers that they all agreed to support group decisions once they were made. Since many physicians consider themselves the last “gentlepersons” in the world, and that their word is their bond, this often brings them back into line.
Groups also frequently develop formal processes to deal with those that don’t live up to their commitments. These processes might include a “Code of Conduct” that outlines acceptable physician behavior. They also typically develop a step-by-step process that the group can use to resolve physician issues. An example of such a process can be found at the end of this article.
A few years ago we worked with a group that had this discussion at the beginning of their strategic planning retreat. One of the physicians said, “So, if we make a decision, we are really going to do it?” I responded in the affirmative, to which he replied, “Well, I guess I will have to pay attention at this meeting!”
If your group is having a problem making (and sticking to) decisions, it is probably because your group has not asked, and answered, these three critical questions.
Group Strategic Planning
A second step in strengthening your group is to develop a group-endorsed strategic plan.
Decisions facing anesthesiology groups today are significant and have long-range implications.
Each of these decisions require substantial resources and lead times. In addition the decisions are often interrelated.
But the significance of the needed decisions is only one factor highlighting the importance of long-range planning. Without planning, physicians in anesthesia groups rarely have a common vision of the direction their firm is moving. This can result in inefficient utilization of resources, lack of direction for the administrative staff, and lack of any progress for the group.
Why is long-range planning important?
- Significant changes in the environment can hurt or help the group. Planning helps identify these issues and prepare for them.
- The planning process allows each physician to communicate his or her vision of the future, and work to develop consensus in their objectives and goals.
- Key issues are highlighted, discussed and resolved.
- The plan provides direction to and sets priorities for the administrative staff for implementation.
- The planning process and completed plan improves communication to both physicians and staff.
- If progress is tracked against the plan, performance measurement can be improved.
- Physician recruitment may be enhanced as potential recruits can quickly understand if their long-range goals are in line with the group.
 Resistance to long-range planning is normally the result of at least one of the following factors:
Resistance to long-range planning is normally the result of at least one of the following factors:
- Physicians do not understand the importance or benefits of longrange planning.
- The physicians have no clear decision-making process to initiate planning.
- Planning has been tried, but the physicians are not convinced of its benefits.
In each of these instances, group leadership should communicate the need for and benefits from long-range planning and then work to implement a process to develop the plan.
What Is Strategic Planning?
All organizations, at one time or another, struggle with the following questions:
- Where are we going?
- How will we get there?
- Why do we want to do it as a group?
To answer these and other important questions, many anesthesia groups are turning to a formal strategic planning process for their organization.
Strategic planning has been defined as a process of developing an integrated, coordinated and consistent long-range plan of action for the organization. One of the first steps in the process is to develop a “vision” statement for the group. This statement describes the group’s preferred future and what it intends to become.
Developing this statement involves answering the following key questions. Looking out over the planning horizon (which is likely 3-5 years at the most):
- What services and specialties do you plan to offer?
- What geographic region do you intend to serve? How many locations are you likely to have?
- How big will the group become? Will you grow to fill the service needs of the market, or will you set an upper end limit on the number of physicians in the group?
- What type of relations will you have with others? Will you remain an independent group? As previously discussed, this is a very important question in today’s environment.
- What benefits do you hope to provide for the owners and employees?
The next step in the strategic planning process is to look at all forces outside of the group that could affect the group’s functioning. This step is called environmental analysis, and its purpose is to identify opportunities and threats that the group faces.
The environmental analysis looks at three areas:
- External Constituent Demands: An external constituent is a group or individual who is capable of taking action or has needs which could favorably or unfavorably impact the group. For example, a major external constituent for an anesthesiologist group might be the hospital it is associated with. It is very important for this type of a group to understand the actions that the hospital might take or the needs they have.
- Competitors: Individuals or organizations who compete for the same set of “customers” as the group are identified and analyzed for major actions which might affect the group.
- Macro-environment: The macro-environment includes large scale fundamental forces that shape opportunities and pose threats of the group. The group should review significant economic, political, demographic, and technological events and trends and their impact on the group.
Once the major actions, events or trends are identified, they should be categorized as opportunities or threats.
 Opportunities are any favorable situations in the group’s environment that support demands for a new service or permit the group to enhance its position. Threatsare challenges posed by unfavorable trends or specific events in the environment that would lead, in the absence of purposeful action, to the stagnation, decline or demise of the group or one of its services.
Opportunities are any favorable situations in the group’s environment that support demands for a new service or permit the group to enhance its position. Threatsare challenges posed by unfavorable trends or specific events in the environment that would lead, in the absence of purposeful action, to the stagnation, decline or demise of the group or one of its services.
The third major step in strategic planning is to look within to identify the strengths and weaknesses of the group. Significant areas of the practice (e.g., personnel, management, decision making) are reviewed to identify areas either capabilities that will lead to or limitations that will prevent the group reaching its objectives.
It is important to identify strengths so that they might be used in planning how to achieve objectives. Weaknesses, on the other hand, may point to the need for programs to correct them.
At this point the group has collected significant data about itself and its environment. Now it is time to put that information to use by setting objectives.
An objective is a description of some situation in the future that you would like to see come about, and which you have a reasonable expectation of accomplishing. Objectives should be developed when:
- Something is wrong (a weakness) and needs to be corrected;
- Something is threatening (a threat), and needs to be prevented;
- Something is inviting (an opportunity), and needs to be pursued.
Objectives should flow from the previous work you’ve done in developing a vision statement, identifying opportunities, threats, strengths and weaknesses, and from your vision of the future of the group.
The final step in developing a strategic plan is to develop and agree on strategies to be used to attain your objectives. Strategies are decisions and/or major action programs employed by the group to fulfill its vision. Once strategies are identified, the group can assign responsibilities and completion dates.
It is important that both the physicians and administrative staff understand that this is their plan and requires their input and participation. If your group has not developed such a plan, how does it know where it’s going?
Will Latham, MBA, President, Latham Consulting Group, Inc.,  Chattanooga, TN. Latham Consulting Group helps medical group physicians make decisions, resolve conflict, and move forward. For more than twenty-five years Mr. Latham has assisted medical groups in the areas of strategy and planning, governance and organizational effectiveness, and mergers, alliances and networks. During this time he has: facilitated over 900 meetings or retreats for medical groups; helped hundreds of medical groups develop strategic plans to guide their growth and development; assisted over 130 medical groups improve their governance systems and change their compensation plans; and advised and facilitated the mergers of over 120 medical practices representing over 1,200 physicians. Latham has an MBA from the University of North Carolina in Charlotte and is a Certified Public Accountant. He is a frequent speaker at local, state and national, and specialty-specific healthcare conferences. He can be reached at (704) 365-8889 or wlatham@lathamconsulting.com.
Chattanooga, TN. Latham Consulting Group helps medical group physicians make decisions, resolve conflict, and move forward. For more than twenty-five years Mr. Latham has assisted medical groups in the areas of strategy and planning, governance and organizational effectiveness, and mergers, alliances and networks. During this time he has: facilitated over 900 meetings or retreats for medical groups; helped hundreds of medical groups develop strategic plans to guide their growth and development; assisted over 130 medical groups improve their governance systems and change their compensation plans; and advised and facilitated the mergers of over 120 medical practices representing over 1,200 physicians. Latham has an MBA from the University of North Carolina in Charlotte and is a Certified Public Accountant. He is a frequent speaker at local, state and national, and specialty-specific healthcare conferences. He can be reached at (704) 365-8889 or wlatham@lathamconsulting.com.