Proposed Meaningful Use Stage 2—What it Means to the Anesthesia and Pain Communities
Abby Pendleton, Esq., The Health Law Partners, P.C., Southfield, MI
Stephanie P. Ottenwess, Esq., The Health Law Partners, P.C., Los Angeles, CA
On March 7, 2012, the Centers for Medicare and Medicaid Services (CMS) published its Notice of Proposed Rule Making (NPRM, or proposed rule) for Stage 2 user requirements for the Medicare/Medicaid Electronic Health Record (EHR) Incentive Program (“meaningful use,” or MU) in the Federal Register. 77 FR 13698.1 There is a three pronged focus to the Stage 2 criteria: standardizing data formats to dramatically simplify how information is both captured and shared across disparate IT systems in order to be better able to coordinate care with other physicians; ensuring that patients be able to access and easily download their healthcare records and images for their own use; and expanding the scope of tracked quality metrics to include specialists and to reflect and improve specific patient outcomes as well as care coordination.

Although subsequent to the final rule establishing Stage 1 MU criteria CMS repeatedly assured the medical community that the needs of specialists would be addressed in the Stage 2 requirements, the Stage 2 proposed rule still falls short for certain specialists including anesthesiologists. Indeed, although CMS itself boasts that the Stage 2 criteria have greater applicability to many specialty providers with the addition of objectives with respect to:
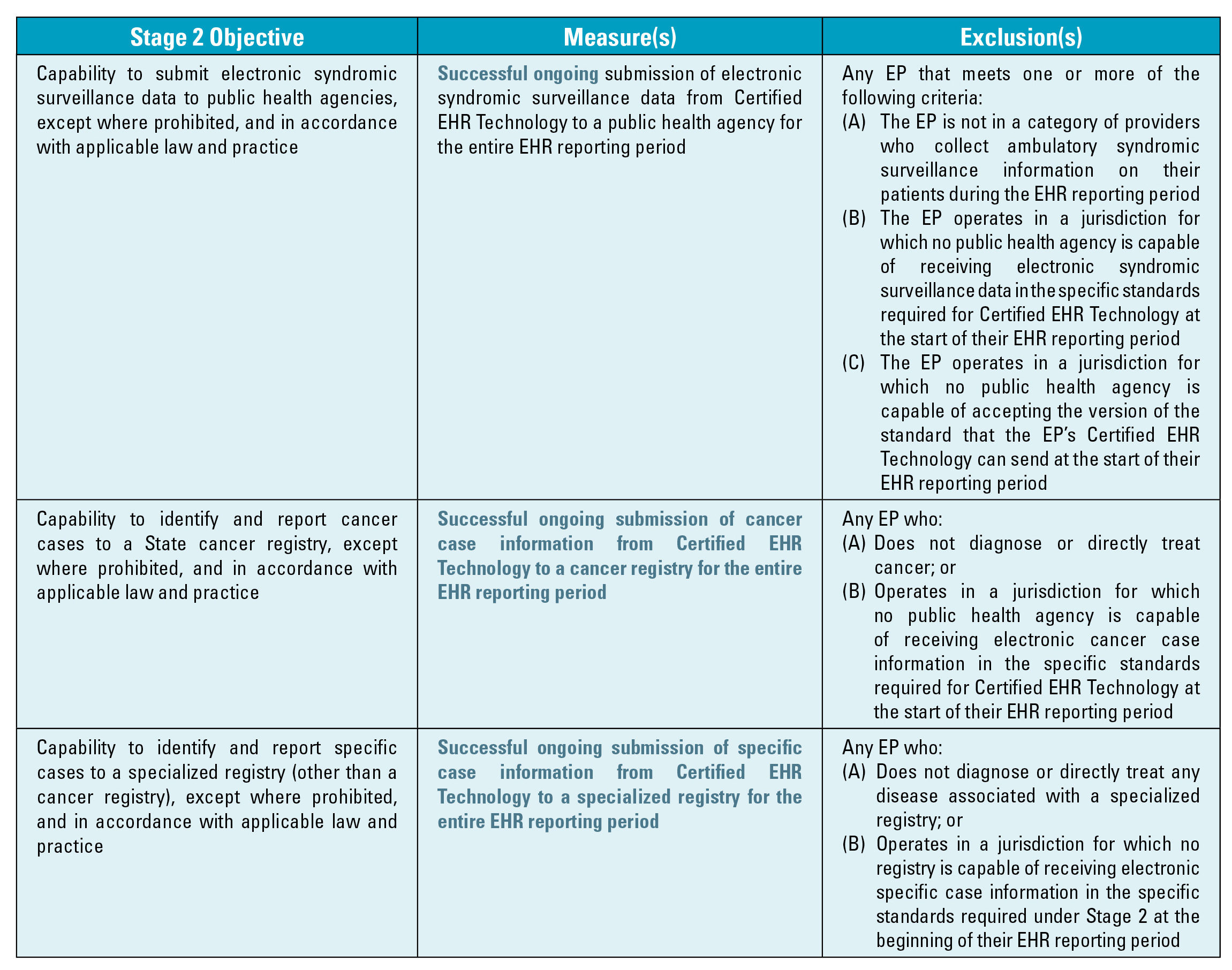
- Imaging results and information accessible through certified EHR technology;
- Capability to identify and report cancer cases to a State cancer registry; and
- Capability to identify and report specific cases to a specialized registry (other than a cancer registry), these objectives are not generally applicable to anesthesiologists or pain specialists.
The proposed Stage 2 criteria establish that anesthesiologists and pain physicians are still stuck in the unenviable position of being required to demonstrate they are meaningful users of Certified EHR Technology – a difficult, if not impossible proposition for most – or face Medicare or Medicaid payment adjustments starting in 2015. As such, this article attempts to boil down the voluminous 455 page NPRM, highlight the changes that have been made to Stage 1 criteria and identify the similarities and differences between Stage 1 and 2 Meaningful Use. On the basis of the majority of this reading audience, the focus is exclusively on the proposed changes to the Medicare version of the EHR Incentive Program for eligible professionals (EPs)2.
Background
On July 13, 2010, CMS issued the final rule defining the meaningful use of EHR that specified the Stage 1 criteria EPs, eligible hospitals and critical access hospitals must meet in order to qualify for an incentive payment, calculation of the incentive payment amounts, and other program participation requirements. The final rules implemented the EHR incentive program requirements under the Health Information Technology for Economic and Clinical Health Act of 2009 (HITECH Act), the health care information technology provisions enacted as part of the American Recovery and Reinvestment Act of 2009 (ARRA). Under the EHR incentive program, Medicare and Medicaid incentive payments totaling as much as $27 billion from 2011 to 2021 will be available for payment to EPs and eligible hospitals for the “meaningful use of certified EHR technology.” The HITECH Act provisions are designed to serve the dual goals of improving health care through increased efficiencies and improved care decisions, while also stimulating economic recovery.

EPs who qualify for Medicare incentives can receive up to $44,000 per EP over a five-year period, while EPs who meet Medicaid patient volume requirements and qualify for Medicaid incentives can receive incentives of up to $63,750 per EP over six years. (EPs who qualify for both incentive programs must choose one.) In the Stage 1 final rule, CMS indicated that the Medicare and Medicaid EHR Incentive Programs would consist of 3 different stages of meaningful use requirements, with each stage requiring increasing use of EHRs and electronic information exchange. The three stages are:
- Stage 1 (which began in 2011 and remains the starting point for all providers): “meaningful use” consists of transferring data to EHRs and being able to share information, including electronic copies and visit summaries for patients.
- Stage 2 (to be implemented in 2014 under the proposed rule): “meaningful use” focuses on advanced clinical processes, including standards such as online access for patients to their health information and electronic health information exchange between providers.
- Stage 3 (expected to be implemented in 2016): “meaningful use” focuses on demonstrating that the quality of health care has been improved.
Stage 2—Anesthesiologists and Pain Physicians Must Still Comply
In the Stage 2 NPRM, there were no proposed changes to the hospital based eligible professional definition, and thus most anesthesiologists will continue to fall within the definition of an EP. Notably, however, CMS does ask for comment on situations where EPs who are classified as hospital-based and working in specialized hospital units have independently procured and utilized EHR technology that is completely distinct from that of the hospital. The focus of the comments should be on whether specialized hospital units are using stand-alone EHR technology as opposed to using the facilities and equipment of the hospital. This situation could be applicable to anesthesia groups, especially those that include pain specialists who have their own pain clinics where they are using stand-alone certified EHR technology.
Transitioning From Stage 1 to Stage 2 Meaningful Use
In the NPRM, CMS proposes a continuation of the existing paradigm in which an EP enters the program at Stage 1, regardless of the year of entry, and spends two years in each stage before proceeding to the next. Importantly, however, CMS proposes an extension of Stage 1, giving providers an additional year for implementation of Stage 2 criteria. Thus, those EPs who successfully participated in 2011 will have until 2014 to move into Stage 2. The reasoning behind this extension is to allow the needed time for vendors to develop and providers to implement certified EHR technology that can meet the new Stage 2 requirements. The additional time to achieve Stage 2 objectives is critical given the higher performance thresholds of Stage 2. With proposed regulations coming out now and final regulations expected this summer, it would have been nearly impossible for EPs to start Stage 2 by January 1, 2013. Certainly, this additional time will give providers the opportunity to emphasize quality over quantity in meeting meaningful use objectives.

In Stage 1, EPs are required to meet, or qualify for an exclusion to, all of the 15 core objectives and 5 out of the 10 menu measures for a total of 20 objectives. In the proposed rule, CMS proposes to maintain the same core and menu measures structure of meeting or qualifying for an exclusion of a total of 20 objectives but increases the number of core objectives to 17 and requires that EPs meet 3 of the 5 menu objectives. CMS is also proposing that, beginning in 2014, meeting exclusions from individual menu set measures will not reduce the total number of menu set measures that need to be reported. In other words, EPs will need to report on 5 of 10 menu set measures, regardless of whether they qualify for exclusions. However, those EPs qualifying for more than 5 exclusions will need to report on all of the menu set measures that are possible to report as well as the remaining exclusions.
Almost all of the Stage 1 core and menu objectives have been retained for Stage 2. However, multiple Stage 1 objectives have been combined into more unified Stage 2 objectives, with a subsequent rise in the measure threshold that providers must achieve for each objective that has been retained from Stage 1. According to CMS, this eliminates unnecessary accounting and reporting burden for providers by recognizing that, for providers who have been Stage 1 meaningful users already, recording these data in structured form has become a normal part of their delivery of health care. Stage 2 follows most of the existing Stage 1 core and menu objectives while adding new objectives for patient access to health information and increasing expectations for healthinformation exchange and data transfer, among other changes. Certain areas and elements in the Stage 2 rule may benefit EPs aiming for, and currently on the way to, meaningful use, whereas others may represent challenges.
Changes to Stage 1
There have been five (5) specific changes to existing Stage 1 objectives and measures including computerized provider order entry (CPOE); vital signs; test of health information exchange; e-copy and online access; and public health objectives. Some of the proposed changes are optional for EPs beginning in 2013 and mandatory in 2014 and beyond. The following chart describes the changes and their effective dates: 
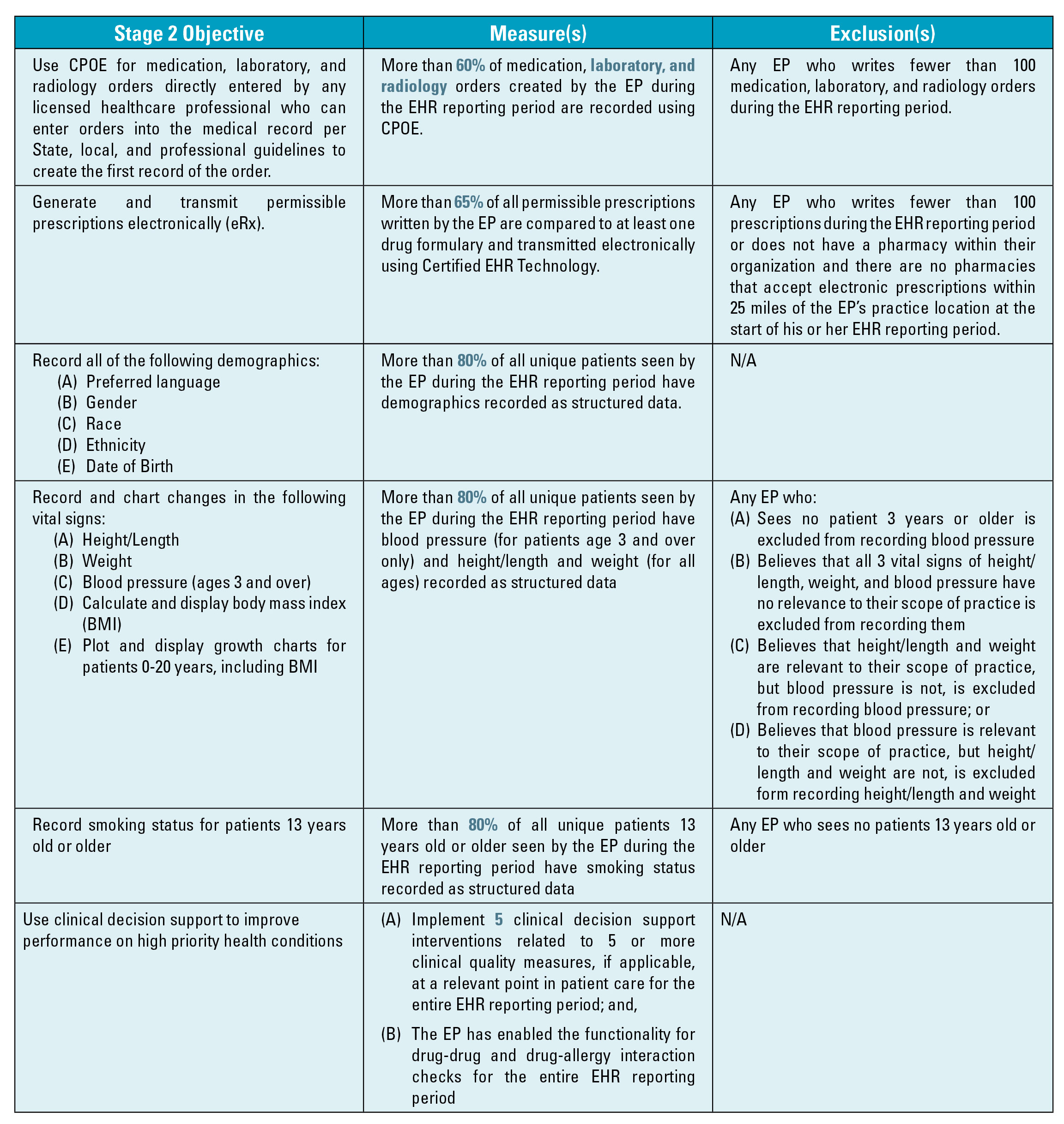
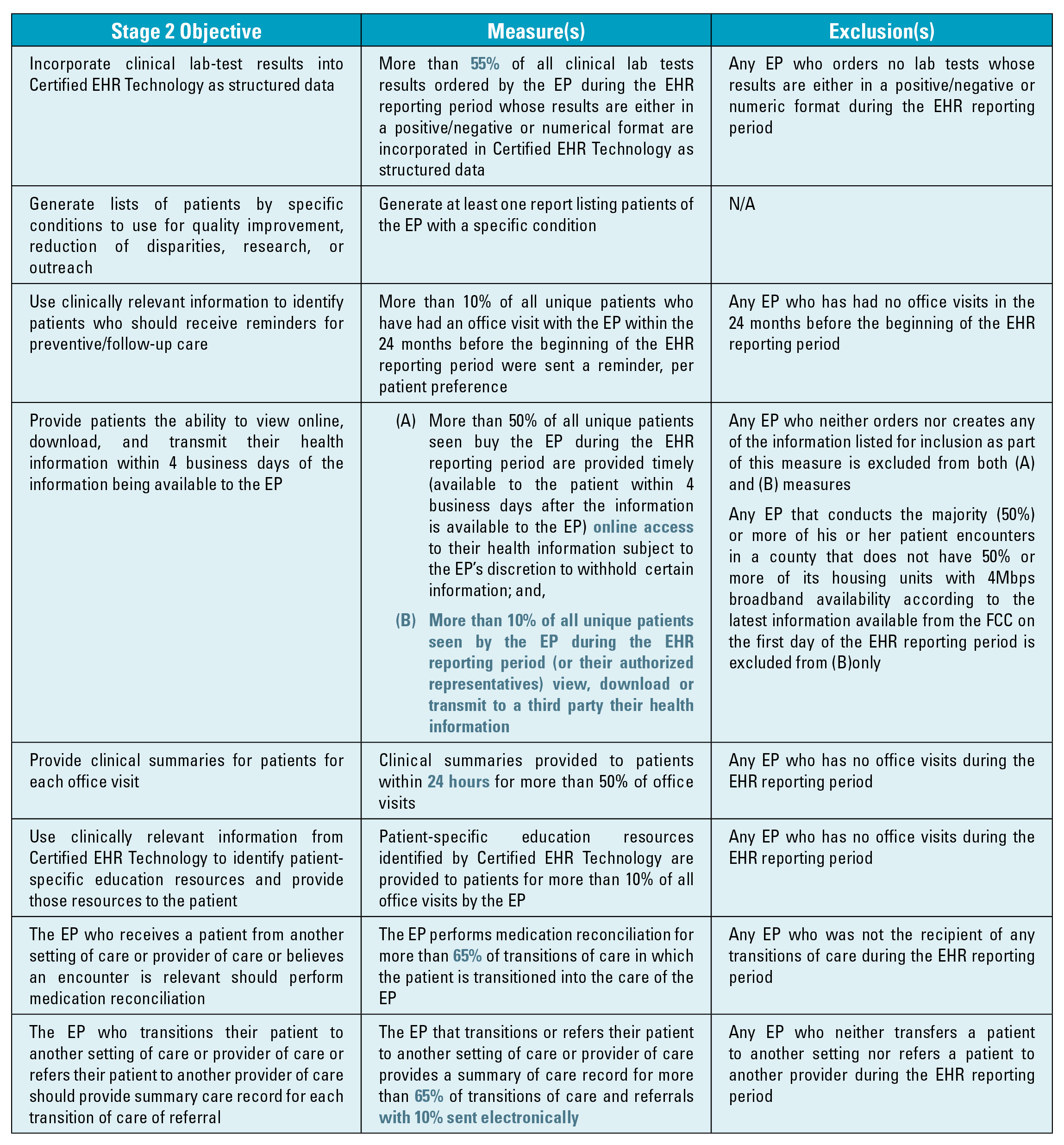
Proposed Stage 2 MU Objectives and Measures
The following table shows the proposed 17 mandatory objectives, measures and exclusions (where available). Changes from Stage 1 or new provisions are highlighted. This table is followed by a table containing the five menu set objectives.

Clinical Quality Measures
Just as in Stage 1, CMS proposes that EPs be required to report on 12 specified clinical quality measures (CQM) in order to qualify for incentive payments. CMS proposes, however, to eliminate CQMs as a meaningful use core objective and instead make reporting CQMs an inherent component of the definition of “meaningful EHR user.” The end result is that CQMs must still be reported in order for the EP to qualify as a meaningful EHR user.
For EPs, Stage 2 proposes a set of clinical quality measures beginning in 2014 that align with the existing quality programs such as measures for the Physician Quality Reporting System (PQRS) and the CMS Shared Savings Program. A major burden for providers to date has been the checkerboard of clinical quality measures that HHS programs ask providers to report. Hopefully, private payors will also adopt these measures for their quality programs since they will be already incorporated into certified electronic health records. If this occurs, it would radically reduce the complexity and burden of quality reporting for providers, and thereby increase clinicians’ focus on improvement.
The Stage 2 changes for clinical quality measures include an enhanced objective and associated measure to use clinical decision support to improve performance on high-priority conditions. This is a move from a requirement to use one decision support “rule” relevant to a specialty orclinical support “interventions” associated with high-priority health conditions. There is also a specific requirement to link each decision support intervention to one or more of the clinical quality measures reported on by a provider. Additionally, the objective to “exchange key clinical information” from Stage 1 was enhanced to provide a summary of care when a patient transitions from, or is referred to, a healthcare professional. These changes are intended to enhance the value of the clinical decision support and data exchange objectives.
The proposed rule also outlines a process by which EPs would submit CQM data electronically after their first year of Stage 1 participation, which, according to CMS, is aimed at the goal of reducing the associated burden of reporting on quality measures for providers. CMS has proposed two different approaches of CQM reporting: aggregate-level electronic reporting as a group or through existing quality reporting systems and is soliciting comments on these approaches.
Payment Adjustments
Medicare payment adjustments are required by statute to take effect in 2015. CMS proposes that any Medicare EP or hospital that demonstrates meaningful use in 2013 would avoid payment adjustment in 2015. Also, any EP that first demonstrates meaningful use in 2014 would avoid the penalty if they meet the attestation requirement by October 1, 2014. This means that the EP must begin the 90 day EHR reporting period no later than July 2, 2014. Notably, CMS is proposing new exceptions to these payment adjustments. This proposed rule outlines three categories of exceptions based on:
- Availability of internet access or barriers to obtaining IT infrastructure;
- A time-limited exception for newly practicing EPs who would not otherwise be able to avoid payment adjustments;
- Unforeseen circumstances such as natural disasters that would be handled on a case-by-case basis.
EPs would be required to submit an application to CMS for an exclusion to apply. The applications would need to be submitted not later than July 1 of the year before the payment adjustment year.
CMS is also soliciting comments on additional criteria for exceptions. Most important to specialists such as anesthesiologists, CMS specifically discussed the possibility that the combination of three barriers that are common to the specialties could constitute a significant hardship. The three barriers include:
- Lack of direct interaction with patients;
- Lack of need for follow-up care for patients; and
- Lack of control over the availability of Certified EHR Technology.
CMS made it a point that they do not believe that any one of these barriers taken independently constitutes a significant hardship but considered whether any specialty may nearly uniformly face all three barriers. Clearly, this is an excellent opportunity for the anesthesia community to convince CMS during the comment period that this exclusion should apply, in large part, to anesthesiologists.
Conclusion
Pursuant to the Stage 1 final rule and the proposed Stage 2 rule, the majority of anesthesiologists and pain physicians will fall within the definition of an EP and, as such, must either demonstrate they are a meaningful user of Certified EHR Technology or face Medicare payment adjustments starting in 2015. In the Stage 2 NPRM, CMS did open the door, ever so slightly, for specialists to make their case that they should not be included in the Medicare and Medicaid EHR Incentive Programs or be subject to the payment adjustments.
There is a 60-day public comment period, until May 7, 2012, which the Anesthesia Community would be well served to aggressively continue in its efforts to convince CMS that they should be excluded from the meaningful use requirements and payment adjustments. Comments can be made at www.regulations.gov. ABC will be submitting a letter. The importance of the comment period cannot be stressed enough as the general consensus is that the final rule, expected to be released this summer, is likely to mirror, in large part, the proposed rule. The Communiqué Spring 2012 P Page 11
Abby Pendleton, Esq., is a founding partner of The Health Law Partners, P.C. and has been practicing healthcare law since 1996. She regularly provides counsel to healthcare providers and organizations in a number of areas, including but not limited to: compliance, Recovery Audit Contractors (“RAC”), Medicare and other payor audits, fraud and abuse, reimbursement matters, and HIPAA Privacy and Security, and physician staff privilege and licensure matters. Ms. Pendleton also specializes in legal issues impacting billing and management companies, anesthesia and pain management providers, hospice providers and mental health agencies. Contact her at (248) 996-8510 or apendleton@thehlp.com.
Stephanie Ottenwess is a partner of The Health Law Partners, P.C. where she practices healthcare law representing providers and suppliers in healthcare litigation, providing counsel regarding fraud and abuse, compliance and reimbursement matters; and is consulted by both healthcare facilities and practice groups for her critical evaluation of any issue affecting risk management, including EHR adoption. Contact her at (248) 996-8510 or sottenwess@thehlp.com.
1 The HHS Office of the National Coordinator for HIT (ONC) issued a companion rule identifying updates to the standards and criteria for the certification of EHR technology. Whereas CMS has regulatory purview over implementation of the EHR Incentive Program, including requirements for participants, incentives, etc., ONC has regulatory authority over the HIT certification program, including the certification criteria, standards, and implementation specifications for products used by program participants.
2 Eligible professionals under the Medicare EHR Incentive Program include: (1) a doctor of medicine or osteopathy;(2) a doctor of dental surgery or dental medicine; (3) a doctor of podiatry; (4) a doctor of optometry; and (5) a chiropractor. Hospital-based eligible professionals are not eligible for incentive payments. An eligible professional is considered hospital-based if 90% or more of his or her services are performed in a hospital inpatient (Place Of Service code 21) or emergency room (Place Of Service code 23) setting. Only a small minority of anesthesiologists provide 90% or more of their services on an inpatient basis. Outpatient procedures performed in the hospital or in an ambulatory surgery center are excluded from the 90%.