What Do We Really Know About ICD-10’s Potential Impact on Anesthesia?
Jody Locke, MA
Vice President of Anesthesia and Pain Management Services
Anesthesia Business Consultants, Jackson, MI
On October 1, 2015, a major change to diagnosis coding was rolled out with the International Classification of Diseases and Health Related Problems 10th revision (ICD-10), and virtually all payers (except workers compensation and auto carriers) have agreed to implement the new codes. There was serious concern that the complexity of the new code sequence (69,000 codes instead of the previous list of 14,000) would have a significant impact and increase the number of claims denied for medical necessity. Fortunately, the Centers for Medicare and Medicaid Services announced a 12-month grace period, presumably to give practices time to get up to speed with the logic of the new codes.
 Curiously though, there was little or no similar guidance from other major payers and plans. Many practices across the country have spent considerable time and resources to improve the quality of their diagnostic coding, but others have not. Some have reduced the percentage of claims not meeting the specific requirements of ICD-10 to 10 or 15 percent, but many have found it a herculean challenge to obtain and document the details of a patient’s diagnosis to the level of specificity required by ICD-10, especially since many surgeons have taken a rather apathetic view of the new requirements. So, now that the CMS grace period has ended, what should we expect? Are we about to see denial rates increase dramatically or is this going to be another example of a policy change for which the advance press is far worse than the actual implementation?
Curiously though, there was little or no similar guidance from other major payers and plans. Many practices across the country have spent considerable time and resources to improve the quality of their diagnostic coding, but others have not. Some have reduced the percentage of claims not meeting the specific requirements of ICD-10 to 10 or 15 percent, but many have found it a herculean challenge to obtain and document the details of a patient’s diagnosis to the level of specificity required by ICD-10, especially since many surgeons have taken a rather apathetic view of the new requirements. So, now that the CMS grace period has ended, what should we expect? Are we about to see denial rates increase dramatically or is this going to be another example of a policy change for which the advance press is far worse than the actual implementation?
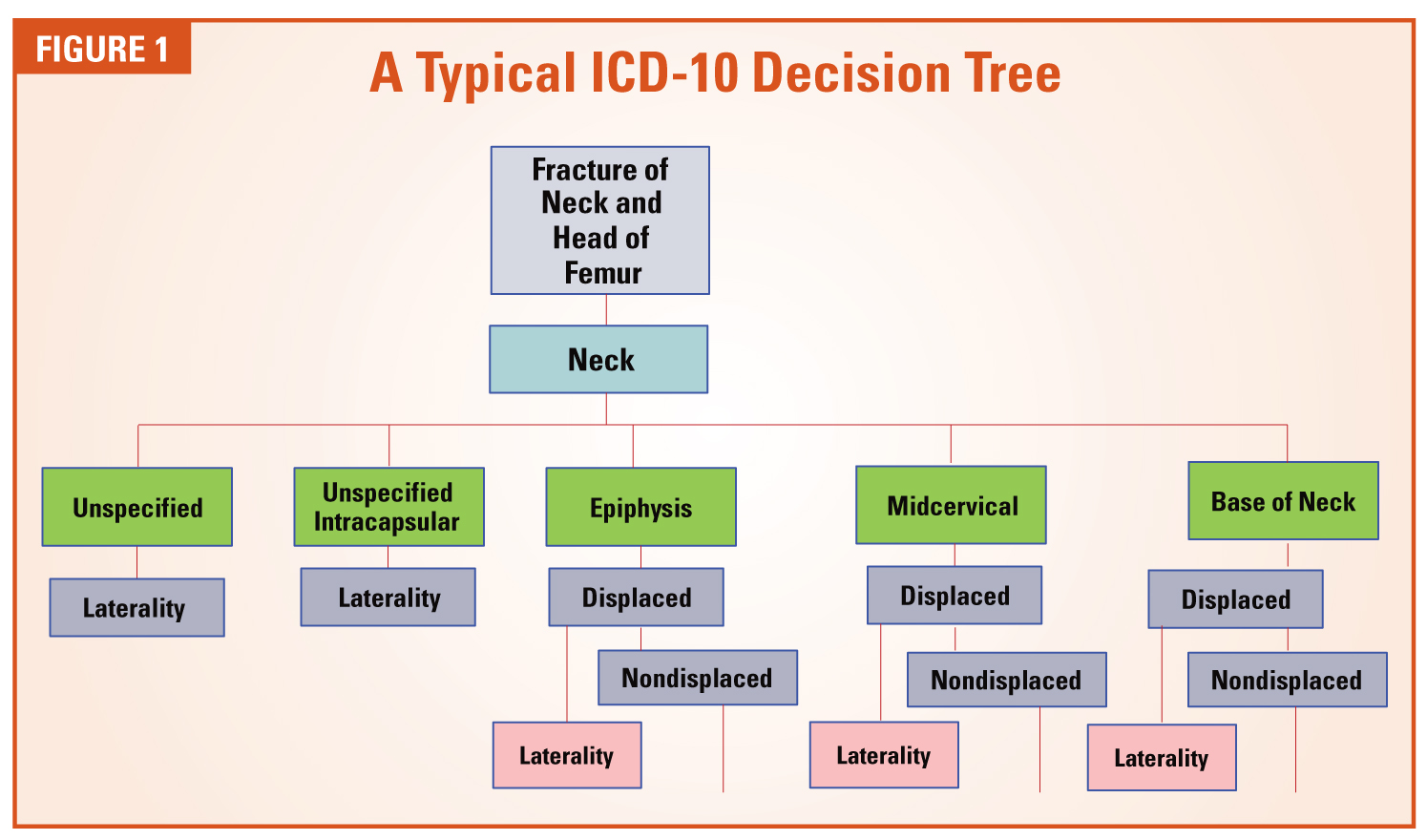
ICD-10 has taken an aspect of clinical documentation that was vestigial and incidental and made it a focus and priority. This, in and of itself, is huge. Now, let us consider the change in structure and logic. ICD-10 introduced concepts that had never been considered before, such as “episode of care.” When picking an ICD-10 code for trauma or fractures, the coder must confirm whether the procedure represented the first time a patient was being treated for the condition, a subsequent treatment, or treatment of complications or sequelae. Many of the early ICD-10 training programs simply focused on the requirement to document laterality, wherever applicable, but this is just one of many new requirements. In most cases, physicians simply have to provide a greater degree of specificity in their diagnosis. The following three examples highlight the basic nature of the new requirements:
- Most physicians used to report that the elderly patient had a cataract. ICD-10 requires the provider to indicate that it was an age-related nuclear cataract of the right or left eye.
- It is no longer adequate to indicate that the patient had appendicitis. ICD-10 requires an indication of the nature and extent of peritonitis.
- What used to be reported as a femur fracture now entails an entirely new checklist of qualifying factors as indicated in the ICD-10 Decision Tree shown in Figure 1.
When ICD-10 was implemented, it was often noted that the new codes would give payers a powerful tool to better evaluate the appropriateness of the medical necessity for each procedure. From a claims adjudication perspective, diagnosis can be defined as the reasonable justification for the service performed. In order for payment to be approved, the CPT code must be justified by an appropriate and relevant ICD-10 code. In simple terms, tonsilitis justifies the removal of the tonsils. Of particular concern to anesthesia providers was the inference that payers would have the ability to compare the ICD-10 code reported on the anesthesia claim to that on the surgical claim. In fact, this potential has consumed much of the discussion since last October. In fact, a certain paranoia has set in, that if the anesthesia diagnosis does not match the surgical diagnosis exactly, then the claim will be denied.
The fact is that most anesthesia claims are submitted well before the surgical claim. Typically, anesthesia claims are only held when the entire episode of care is being questioned. The prospect of payers holding anesthesia claims to be matched against the surgical claim poses significant logistical claims to payers and would, admittedly, have a material impact on anesthesia cash flow. Most observers of American healthcare do not believe this is a serious possibility, but no one knows for sure, and we cannot dismiss the possibility that payers will use ICD-10 as an excuse to deny a higher percentage of claims.
Given current standards of electronic claims adjudication, it is far more likely that payers will focus on the degree of specificity for all claims rather than on how closely they match. Herein lies one of the greatest challenges for the anesthesia provider. The irony of ICD-10 is that it requires the anesthesiologist to provide a diagnosis that could be used to evaluate the surgeon’s diagnosis. How is the anesthesia provider going to get the necessary details, if not from the surgeon? Most anesthesia practices that have implemented a postoperative time-out” to allow the surgeon to share procedure and diagnosis have found that many surgeons simply do not understand the requirements of the new codes, nor do they seem to care. Anesthesia providers frequently report that the surgeon’s response to their queries is this: “My office staff is responsible for picking the code.”
As anesthesia providers slowly came to terms with the implications of ICD-10, many obstacles and challenges started to come to light. Despite what one might have expected, practices with electronic medical records (EMRs) and electronic anesthesia records had the hardest time meeting the new requirements. Why? They had the least ability to review and edit the details of the diagnostic descriptor. One had hoped that the EMR would provide access to the more detailed surgical operative report, but more often than not, the report did not provide the necessary detail. In many cases, the final postoperative surgical diagnosis is simply not known by the end of the case. Questions were raised, for example, about how to treat a biopsy when the pathology report was not available. Many practices attempted to implement a postoperative time-out for the anesthesia provider to confirm the details of procedure and diagnosis, but in many cases, the surgeons were not up to speed, arguing that such details of coding were “a back office function.”
The efforts to reduce the percentage of unspecified ICD-10 codes on claims continues, but one thing has become abundantly clear: If you’ve seen one anesthesia practice, you’ve seen one anesthesia practice! Every approach and strategy must be custom-tailored to the unique needs of the practice and the ability of its providers to master the logic of ICD-10. Scorecards do help. One cannot manage what one cannot measure. But scorecards (and detailed provider feedback) are only one piece of a much more complicated puzzle. Modifying provider behavior is no small challenge, and in the case of diagnosis, it is proving to be huge.
We are almost a year out from the initial rollout of the new ICD-10 codes, and there have been virtually no denials related to the specificity of the ICD-10 code or mismatches with the surgeon’s code. There is nothing that gets a provider’s attention as quickly as issues affecting cash flow. Because ICD-10 does not appear to have had an impact thus far, many providers have started to dismiss its significance.
Anesthesia Business Consultants has been very focused on educating providers about ICD-10 and has conducted dozens of in-service sessions in person and via web meetings. The company has also developed a coding application called F1RSTCode to help client providers confirm the data elements necessary to document the diagnosis.
If we draw an analogy to the administration of anesthesia, there are some useful parallels. It is often said that of the five phases of anesthesia—preparation, induction, maintenance, emergence and recovery—preparation is the most important. The goal is to identify potential risks and prepare for them. So it is with ICD-10. We will not know what the financial impact of ICD-10 will be until it happens. The best advice we offer at this point is to reduce the potential risk areas that payers could take advantage of to deny claims. Probably, things will not change too much, but we cannot know for sure. Just because we don’t think something will happen doesn’t mean it won’t. It is much better to be prepared for the worst and be relieved when it turns out payers are as reluctant to change their behavior as providers.
If you would like more information about how ICD-10 will affect your practice, please contact your client manager and ask for your detailed ICD-10 Client Coding Feedback report (ICCF).
 Jody Locke, MA serves as Vice President of Anesthesia and Pain Practice Management for Anesthesia Business Consultants. Mr. Locke is responsible for the scope and focus of services provided to ABC’s largest clients. He is also responsible for oversight and management of the company’s pain management billing team. He is a key executive contact for groups that enter into contracts with ABC. Mr. Locke can be reached at Jody.Locke@AnesthesiaLLC.com.
Jody Locke, MA serves as Vice President of Anesthesia and Pain Practice Management for Anesthesia Business Consultants. Mr. Locke is responsible for the scope and focus of services provided to ABC’s largest clients. He is also responsible for oversight and management of the company’s pain management billing team. He is a key executive contact for groups that enter into contracts with ABC. Mr. Locke can be reached at Jody.Locke@AnesthesiaLLC.com.