The Perioperative Surgical Home: Of Economics and Value
Rick Bushnell, MD MBA
Director, Department of Anesthesia, Shriners Hospital for Children, Los Angeles, CA and Huntington Memorial Hospital, Pasadena, CA
“If someone offers you an amazing opportunity but you are not sure you can do it, say YES, then learn how to do it later.”—Sir Richard Branson
Presented with inevitable change and opportunity, how will each of our anesthesia groups create its own future? Will you continue to commit yourself to fading traditional practice patterns and payment models? Or will you take advantage of the paradigm shifts that are already upon us?
Payers are demanding better results. The Centers for Medicare and Medicaid Services (CMS) is willing to pay. Our hospitals are begging for physician leadership and our surgeons will need anesthesiologists more than ever. Best of all, proactive physicians in the American Society of Anesthesiologists (ASA) are pointing the way. There is every reason for a great future...depending on how you respond to the challenges.
 CMS has been encouraging coordinated care and quality through the Physician Quality Reporting System and the Value-Based Payment Modifier. Those programs, along with the Meaningful Use (EHR) incentive program, will be replaced on January 1, 2019 by the Merit-Based Incentive Payment System (MIPS) and Alternative Payment Models (APMs). CMS will pay up to a four percent bonus for high self-reported MIPS scores and up to a four percent penalty for poor performers, beginning in 2019. In 2019, therefore— assuming that the overall amount of penalties assessed offset the amount of bonuses, in budget-neutral fashion—the difference between maximum positive and negative scores will be eight percent and by 2022 the difference will be 18 percent—every single year. Might I ask what return on your business investment do you need? When did you achieve that return on your personal investment portfolio? Private payers are sure to soon follow suit, but this 18 percent CMS incentive alone is strong enough that anesthesiologists should fully embrace MIPS quality and coordinated metrics. As for APMs, if you receive a “significant portion” of your Medicare payments through an eligible APM entity, you will be totally exempt from the MIPS requirements. As a “qualifying APM participant,” you will receive a five percent bonus in each of the five years between 2019 and 2024. From 2026 onward, you will be eligible for 0.75 percent increase in your annual Medicare payments—half a percent more than physicians who merely satisfy MIPS.
CMS has been encouraging coordinated care and quality through the Physician Quality Reporting System and the Value-Based Payment Modifier. Those programs, along with the Meaningful Use (EHR) incentive program, will be replaced on January 1, 2019 by the Merit-Based Incentive Payment System (MIPS) and Alternative Payment Models (APMs). CMS will pay up to a four percent bonus for high self-reported MIPS scores and up to a four percent penalty for poor performers, beginning in 2019. In 2019, therefore— assuming that the overall amount of penalties assessed offset the amount of bonuses, in budget-neutral fashion—the difference between maximum positive and negative scores will be eight percent and by 2022 the difference will be 18 percent—every single year. Might I ask what return on your business investment do you need? When did you achieve that return on your personal investment portfolio? Private payers are sure to soon follow suit, but this 18 percent CMS incentive alone is strong enough that anesthesiologists should fully embrace MIPS quality and coordinated metrics. As for APMs, if you receive a “significant portion” of your Medicare payments through an eligible APM entity, you will be totally exempt from the MIPS requirements. As a “qualifying APM participant,” you will receive a five percent bonus in each of the five years between 2019 and 2024. From 2026 onward, you will be eligible for 0.75 percent increase in your annual Medicare payments—half a percent more than physicians who merely satisfy MIPS.
Our hospital administrative partners, who are subject to their own increasingly important value incentives, are begging for anesthesia’s help. If they haven’t yet realized the value of your perioperative skill set, then it’s time for you to offer to show them. Administrators are overworked, under-inspired and dealing with their own mandates to coordinate care and share outcomes data. Hospitals are also subject to their own system of CMS penalties, caps and bundled payments. You may not personally know it yet, but your management and vision are in demand and needed outside the operating room. Your new management target is the 20 percent of sickest patients presenting for surgery. These are the patients at highest risk for readmission and anesthesiologists need to see those patients in clinic beforehand. This is the time and place for medical leadership.
Fortunately for our specialty, the ASA is pointing the way to the concept of the Perioperative Surgical Home (PSH). For the ASA, this is the moral and medical core of the future of our specialty. Who better than anesthesiologists to understand the physical challenges posed to patient physiology by surgery? Who better to coordinate the preoperative work-up, the acute intraoperative care and the post-discharge medical management? Establishing an Anesthesia PSH clinic is medically and politically valuable to your group.
Then that pesky, repetitive, timeless question arises, “But how do I get paid for being in clinic?” If perioperative management of the sickest patients is such a great thing, who is willing to support that anesthesiologist? Will CMS and private insurance pay; will anesthesia groups internally reimburse and will hospitals share the savings back with anesthesia groups?
Believe it or not, CMS is willing to pay. “Yes,” there are fee-for-service codes. “Yes,” they will pay for both preop and post-discharge management. “Yes,” you can use these codes for your clinic time. And just as you suspected, “No,” it’s not enough. But let’s explore the initial math of fee-for-service clinic appointments.
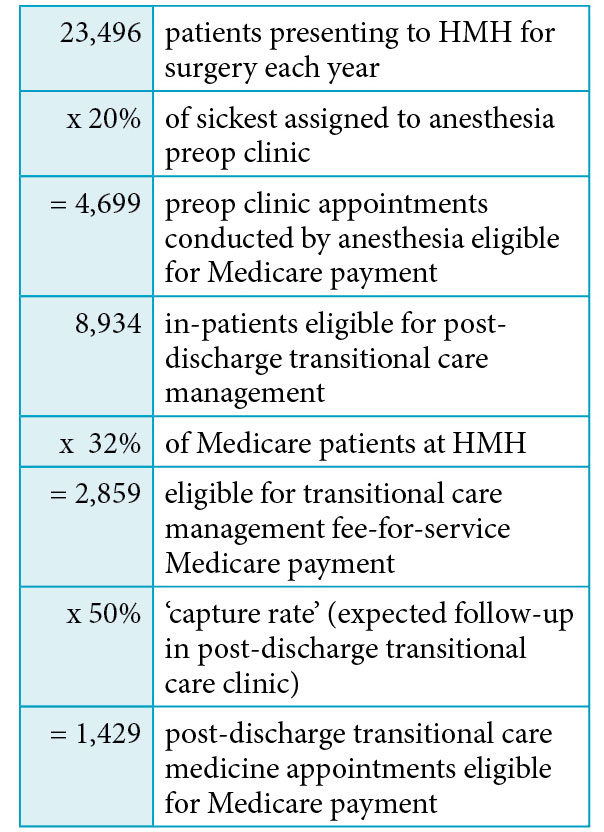
Consider our southern California hospital, Huntington Memorial (HMH), with 14,562 outpatient and 8,934 inpatient surgeries per year (total 23,496). Because of our PSH proposals, HMH will strongly encourage surgeon triage and risk stratification of these patients. HMH will soon mandate the appearance of all patients in preop clinic before elective surgery and assign the 20 percent of sickest to be seen by an anesthesiologist. Our Pacific Valley Medical Group (PVMG) anesthesia group will station one full time equivalent (FTE) anesthesiologist in clinic targeting the 20 percent of sickest patients, clearing, medically optimizing or canceling them as indicated. The goal is for our anesthesiologists to also see these same 20 percent of sickest patients in post-discharge clinic.
So based on the assumptions below,* let’s do the math on just three of the various revenue streams that could be used to support our private practice, full-time equivalent PSH clinic anesthesiologist.
The Fee-for-Service Payment Model:
CMS Payment for Pre-Operative Evaluations Current Procedural Terminology (CPT®) Codes for Los Angeles (locality #0118218) in 2016:

Post-Discharge Transitional Care Management Reimbursement Codes:

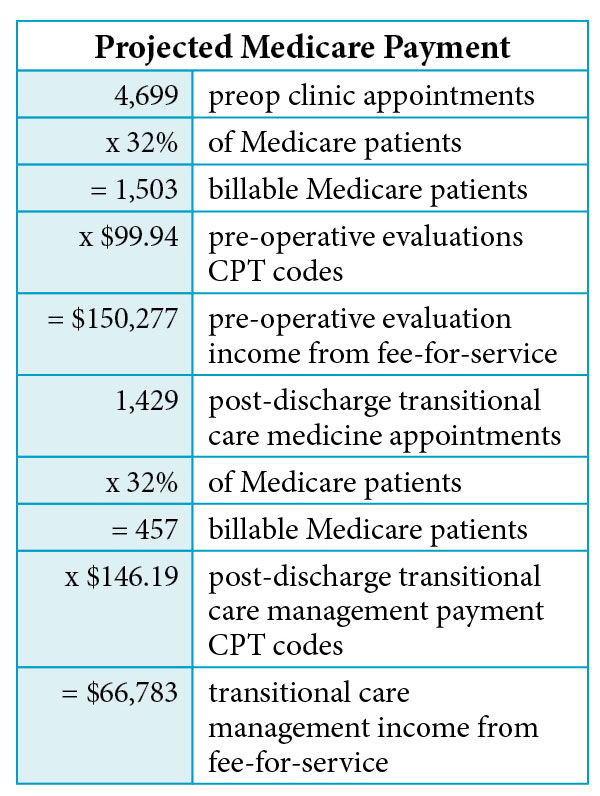
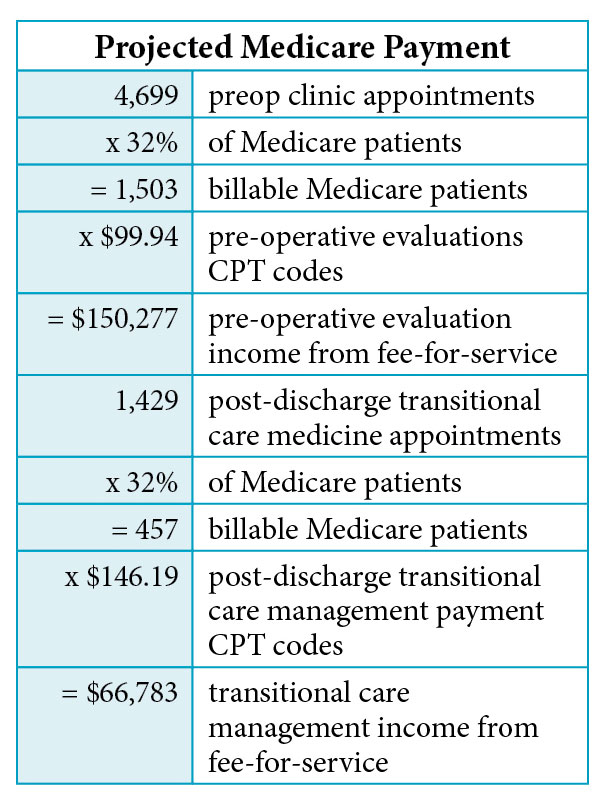
For the purposes of the revenue projection below, we’ll assume an average mix of CPT codes submitted to CMS. Let us also assume Medicare patients constitute 32 percent (actual HMH payer mix) of clinic appointments.
Using the above averages to project Medicare perioperative clinic payment:
Anesthesiologists should understand these codes and their associated compliance criteria.
At-Risk Medicare Payments to Anesthesia Practice, 2019-2022 Onward
Groups must quantify the contribution of the PSH to their practices. The Medicare MIPS at-risk numbers for our PVMG anesthesia practice are:

Assuming that PVMG qualifies for the maximum MIPS amount in each of the five years 1919-2023:

Anesthesia groups should be willing to invest a portion of their at-risk revenues to comply with CMS quality and practice mandates.
Costs to Hospital of Preventable Readmissions
Hospitals must quantify the contribution that anesthesiologists can make to hospital cash flow. The Medicare preventable readmissions at-risk numbers for HMH are:



The total potential savings to HMH is projected to be $1,056,684 over three years which justifies PSH support for anesthesiologist involvement. This incentive projection peaks around $100,000 in the third year and is used in summary calculations below.
Hospital Savings Accrued through Decreased Length of Stay**:
New York University (NYU) School of Medicine has now demonstrated that patients who attend their preop evaluation clinic have significantly shorter length of stays (LOS) and observed-to-expected LOS ratios than those who do not attend clinic.
For the NYU study’s financial analysis, 28,828 surgical encounters were included. There were 17,593 patients who attended clinic and 11,235 who did not. The mean variable direct cost per case was $5,754 for patients seen in the preoperative clinic and $7,127 for those who were not. The resulting savings were more than $1,373 per case.
Assuming much and applying the NYU numbers to HMH’s Medicare population: Hospitals should be willing to invest and incentivize to support the PSH FTE anesthesiologist in the PSH in an attempt to lower readmission rates and costs.
The Total of Annual At-Risk and Potential Cash Flows Available for Support:

This is our bottom line result using only a Medicare population (32 percent of inpatient surgeries). Certainly if we included private payer patients, the total potential savings and cash flows would be much larger. Based on these financial calculations, hospitals and practices have all the financial motivation they need to form joint ventures.
Possibly more important, you now have an objective analytic process by which to work your own numbers. By projecting your own practice’s contribution, you can approach your own Accountable Care Organization (ACO) with objective financial cause for an appropriate percentage of future bundled payments. An anesthesiologist presence in the PSH is negotiating power.
My strong suggestion is that hospitals and anesthesia practices contribute to a financial plan that supports one FTE clinic anesthesiologist. The joint hospital/practice financial plan should be monitored closely by all parties and adjusted accordingly. The stated goal of the financial plan should be an effective system of incentives and support, not an excessive revenue stream for the anesthesia practice or physician. Excess funds should be qualified and retained in a separate pool for use as additional personnel or performance incentives.
Your Own Amazing Opportunity
You now have my calculations, projections and suggestions for generating payment support from three categories of PSH cash flows. It may take a bit of financial creativity, but the combination of fee-for-service, shared CMS savings and hospital incentives should be enough to support one FTE anesthesiologist in the PSH. A well-constructed financial plan should get most organizations to that point. But allow us to conclude by considering a calling.
At the beginning of this article, Sir Richard Branson spoke of taking advantage of “an amazing opportunity.” His reference was to business and finance. Surely those issues are important, but consider what an amazing opportunity the PSH is for medical leadership.
Anesthesia is naturally positioned at the logistical and medical nexus of surgical challenges presented to both the patient and the healthcare system. It is my postulate that this position obligates our specialty to exercise greater medical leadership than we have lately assumed. Thirty years ago patients were admitted for surgery the night before and stayed a week after the procedure. We rounded on our next day’s patients the night before and called on them the day after surgery. Today we meet complicated patients three minutes before surgery and seldom round on them afterward, if they are admitted at all. We’ve allowed ourselves to become anonymous and our reputation often now suffers from invisibility. We are often being replaced by mid-level care providers.
The PSH is the perfect position from which to reclaim the medical authority that has slipped away from anesthesiologists. We can only reassert the great value of our specialty by practicing our medical and management skills thought out the entire continuum of the perioperative surgical process. Stepping up to assume our share of the responsibility for outcomes will naturally give rise to the credibility only medical leadership can confer.
Greater anesthesia involvement promises increased day-of-surgery efficiencies, increased rapport between services, better outcomes, increased patient satisfaction and the elevated perception of our specialty. How could these things not flow from our greater ownership of all the obligations of our position? We already know we can do better than relegating ourselves to three minutes before surgery and one minute after. It is now time to pick up this cause and to once again own all of our obligations. This is the reclamation and maturation of our specialty.
It is my personal challenge that you value the opportunity for medical leadership above all cash flows. Your physician presence in the PSH is your own “amazing opportunity.” As an anesthesiologist, this is the platform upon which to practice your entire medical skill set and to exert your medical leadership.
In the fourth article of this series, which will appear in the summer issue of the Communiqué, let us consider the future of the Perioperative Surgical Home.
*Assumptions and Caveats: Some aspects of CMS programs are beyond the scope of this article. For the cause of simplicity and to focus on the major issues, many details and arguments have been reserved for another conversation. Please accept the assumptions below that we have made for the sake of analysis here.
- The limitations of data access necessarily confine this analysis to publically available Medicare data. Private data have not been included. More complete individual analysis should include billing company, individual practice and hospital data that is inclusive of private payer reimbursements.
- The stated, targeted goal is to have our anesthesiologist attend to the 20 percent of sickest patients is an arbitrary number. That number will not be initially achievable for many reasons, principally the challenge of volume. Totaling the projected pre- and post-op clinic appointments and dividing that number into the available days results in the clinic anesthesiologist attending to 23 appointments per day. This number is not feasible and reductions of volume based on actual clinic volume will likewise reduce fee-for-service revenue projections.
- Not all MIPS or APM scores will or can be improved by the PSH. It is assumed that commitment to the high level of coordinated care it takes to manage a PSH will lead naturally to commitment to all areas of quality scoring and reporting. Credit the PSH with leadership.
- Conversations concerning MIPS, APMs and Value-Based Purchasing will be taken up in another article.
**Preop Evaluation Clinics (PEC) Reduce Readmission Rates and Hospital Stays, Clinical Anesthesiology, March 23, 2016. http://www.anesthesiologynews.com/Clinical-Anesthesiology/Article/03-16/Preop-Evaluation-Clinics-Reduce-Readmission-Ratesand-Hospital-Stays/35555/ses=ogst
Rick Bushnell, MD, MBA is the Director of the Department of Anesthesia, Shriners Hospital for Children, Los Angeles, CA and a Clinical Anesthesiologist at Huntington Memorial Hospital in Pasadena, CA. Dr. Bushnell graduated from the University of Illinois College Of Medicine and attended the University of Pittsburgh Medical Center, Pittsburgh and Loma Linda University for internship and residency. He has been with Pacific Valley Medical Group since 2003 and consults with Shriners Hospital for Children, Los Angeles. He and his partner have six adopted children in Tanzania where he serves as Visiting Clinical Anethesiologist at St. Elizabeth’s Hospital for the Poor in Arusha. He can be reached at propofolstingsme@gmail.com.