2016 Coding Updates for Anesthesia
Kelly D. Dennis, MBA, ACS-AN, CANPC, CHCA, CPC, CPC-I
Perfect Office Solutions, Inc., Palmetto, FL
When you received your 2016 Current Procedural Terminology (CPT) and American Society of Anesthesiologists (ASA) Relative Value Guide (RVG) books or discs, you probably noticed there were no new anesthesia code additions or deletions listed for this year. Since the CPT book usually arrives before the RVG, you may not have taken a good look through your RVG or may not have ordered a 2016 RVG as there were no coding changes. However, there are a number of important updates in the RVG New/ Revised RVG Coding Comments section which are not included in the Anesthesia section of the CPT. These comments may affect the way anesthesia coders assign procedure codes in the upcoming year. As this article will not include all updated comments, be sure to order your 2016 RVG. I’ve chosen a few that are certain to have an impact on 2016 coding for anesthesia services.
Let’s start with 00218, “Anesthesia for intracranial procedures; procedures in the sitting position” with a base value of thirteen units. As you may know, base unit values increase as the difficulty of a procedure increases. The new coding comment indicates “This code may be reported for anesthesia for any intracranial procedure performed with the patient in the sitting position.” For example, although the sitting position for cranial surgery is associated with a high incidence of air embolism (Schubert), a craniotomy or craniectomy for evacuation of a subdural infratentorial hematoma may be performed with a patient in the sitting position. Rather than assigning 00210 “Anesthesia for craniotomy or craniectomy for evacuation of hematoma” with a base unit value of ten, coders will assign 00218. This code assignment also depends on the anesthesia provider clearly indicating on the anesthesia record that the patient was in the sitting position.
 Coders cannot capture billable services that are not indicated on the anesthesia record, even if they are marked on an internal billing sheet. Billing sheets are not usually considered as part of the patient’s medical records. There is no universal anesthesia record and a typical anesthesia billing company sees a number of different records, so coders must determine where on each record anesthesia providers document special positioning, which can be quite challenging with paper records and handwritten notes. With a paper record, the clearest way to document is a legible note in the remarks or comments section. Electronic anesthesia records (EARs) are much easier to read and may have a field summary, which typically includes an area to document when the patient is in the sitting, or any other special position. If the EAR doesn’t have a field summary, look within the body or comments section. If you are not sure where this information is documented, learn where patient positioning information is documented in your practice.
Coders cannot capture billable services that are not indicated on the anesthesia record, even if they are marked on an internal billing sheet. Billing sheets are not usually considered as part of the patient’s medical records. There is no universal anesthesia record and a typical anesthesia billing company sees a number of different records, so coders must determine where on each record anesthesia providers document special positioning, which can be quite challenging with paper records and handwritten notes. With a paper record, the clearest way to document is a legible note in the remarks or comments section. Electronic anesthesia records (EARs) are much easier to read and may have a field summary, which typically includes an area to document when the patient is in the sitting, or any other special position. If the EAR doesn’t have a field summary, look within the body or comments section. If you are not sure where this information is documented, learn where patient positioning information is documented in your practice.
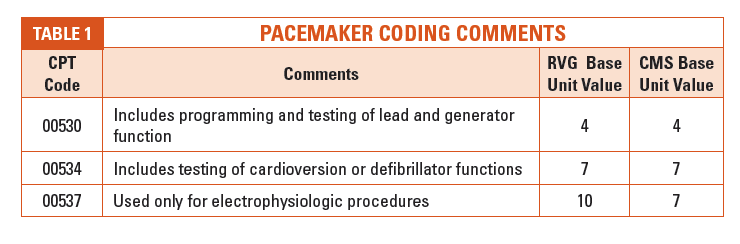
There were substantial changes to pacemaker coding comments under CPT codes 00530, 00534 and 00537 (See Table 1). The comments describe anesthesia for pacemaker services and indicate when it is acceptable to report the higher base unit values for active testing of an implantable cardioverter defibrillator (ICD) device or electrophysiologic (EP) testing. So it is important that (1) coders understand the difference, and (2) anesthesia providers are giving enough information to the coders to allow proper anesthesia code selection.
If cardioversion or defibrillator functions are not tested, coders are referred to CPT 00530, with a base value of four units. Documented testing of cardioversion or defibrillator functions increases the base value to seven units and is reported with CPT 00534. If an EP procedure is performed, CPT 00537 with a base unit value of ten is the appropriate anesthesia code. Coders should review these codes and circumstances with providers to ensure documentation supports the anesthesia code selected and reported, and be aware the Center for Medicare and Medicaid Services (CMS) has assigned a lower unit value than the RVG for EP procedures (See Table 1). The anesthesia codes for pacemaker related services are not listed in the MLN Matters article “National Coverage Determination (NCD) for Single Chamber and Dual Chamber Permanent Cardiac Pacemakers” (Number MM9078) as requiring a -KX modifier (indicating “Requirements specified in the medical policy have been met”) for Medicare patients, although the surgeon may be required to report a -KX modifier.
Another common area of interest to anesthesia coders is related to extracorporeal shock wave lithotripsy (ESWL). When I first started in anesthesia more than 32 years ago, it was common to see treatment for lithotripsy while the patient was immersed in a water bath; however, now it may be more common to see other types of ESWL treatment. According to Dr. Grasso, “In first-generation lithotriptors (Dornier HM3), the patient was placed in a water bath. However, with second- and thirdgeneration lithotriptors, small waterfilled drums or cushions with a silicone membrane are used instead of large water baths to provide air-free contact with the patient’s skin.” The 2016 comment for CPT 00872 indicates, “Use only when patient immersed in water bath. With small water filled drums/cushions, see 00873.” As there is a base unit value difference of two units between these codes, coders should ensure they are reporting as instructed. If you are not certain whether your practice’s facilities still use water bath or not, it’s time to check!
CPT codes 36221–36626 describe non-selective and selective arterial catheter placement and diagnostic imaging of the aortic, arch, carotid and vertebral arteries. The 2016 ASA Crosswalk revises the reported anesthesia code for each of these procedures to 01916, “Anesthesia for diagnostic arteriography/venography” with a base value of five units. This is a substantial change from 2015 crosswalk codes ranging from six to ten base units.
Aside from multiple valuable comment and crosswalk code revisions, it is noteworthy that the 2016 RVG no longer includes ASA standards and guidelines relevant to coding and billing in the back of the book. The bad news is that it is no longer a matter of flipping through to the end of the RVG to access information when coders need to provide “proof” of why we do the things we do. The good news is the ASA provides all current version of their standards and guidelines on the ASA website (See Resources). While the information is not as convenient, unless you have internet access, keep in mind there is added value to having access to the most up-to-date information ASA provides.
 Trying to keep up with ongoing changes to the Physician Quality Reporting System (PQRS) coding is a constant challenge for coders. There were no changes to the 2016 requirements for reporting cross-cutting measures, although a number of new cross-cutting measures have been added. However, PQRS coding is a different story.
Trying to keep up with ongoing changes to the Physician Quality Reporting System (PQRS) coding is a constant challenge for coders. There were no changes to the 2016 requirements for reporting cross-cutting measures, although a number of new cross-cutting measures have been added. However, PQRS coding is a different story.
You may have noticed in CPT Appendix B – Summary of Additions, Deletions and Revisions that there were textual changes to Category II Code 6030F (removing “cap and mask and sterile gown and sterile gloves and a large sterile sheet and 2 percent chlorhexidine” from the code description), and there were no Category II code deletions—but that doesn’t mean anesthesia coders don’t have to worry about deleted PQRS codes. Although Measure #44 (Category II Code 4115F) is still listed as a valid code, CMS removed this measure from claimsbased reporting. Code 4115F is still a valid code for registry reporting along with CPT 00562. In a nutshell, effective January 1, 2016, Measure #44 is no longer reportable if your anesthesia practice is using claims-based PQRS reporting.
Similarly, although Category II Codes 4250F and 4255F (Measure #193) are both still listed in the 2016 CPT, 2015 will be the last reporting year for this measure. Measure #193 has been retired and, it too, will no longer be reportable effective January 1, 2016. These changes, announced in the final physician fee schedule rule, which was published in the Federal Register on November 16, 2015, leave claims-based reporting anesthesia groups (estimated at 80 percent) only one PQRS measure specific to anesthesia – Measure #76 (Category II Code 6030F). Since anesthesia providers do not have nine measures across three domains, they will automatically be subject to the Measures Applicability Validation (MAV) process (unless they make a measure applicable to themselves by reporting it even once “unsuccessfully,” e.g., by appending the -8P modifier that shows that the measure wasn’t performed and doesn’t indicate that there was a valid reason for the non-performance. Many anesthesiologists unfortunately fell into this trap, which deems them to have failed PQRS altogether, for payment year 2016 based on 2104 reporting.)
The MAV applies to both claims-based and registry-based reporting, though the methodology differs. With claims-based, as there is only one applicable anesthesia measure (#76), as long as your provider meets the 50 percent threshold and also reports at least one “cross-cutting measure” if any apply (see below), no penalty should be assessed. Keep in mind that a claim with an -8P modifier, which indicates the action was not performed and no reason was documented, does not count toward the 50 percent threshold—or successful performance. Surprisingly, many anesthesia providers who successfully performed and reported PQRS in 2014 received a 2016 penalty notice (based on a two year look back period) and it appears other specialties experienced the same issue. Fortunately, the American Medical Association (AMA), Medical Group Management Association (MGMA) and the ASA are aware of the problem and are working toward a potential solution.
Unfortunately, anesthesia practices that do not place Swan Ganz or Central Venous Pressure (CVP) lines have no associated claims-based PQRS measures. According to the PQRS help desk (Quality Net communication to author), “if you are not able to report Measure #76 via claims, you are required to hire a registry for reporting the other applicable measures or a Qualified Clinical Data Registry (QCDR).” Although claims-based reporting of PQRS measures has not gone away, if you can’t report the only anesthesia PQRS measure left, registry reporting allows your anesthesia practice to report enough anesthesia specific performance measures to avoid payment penalties in 2018.
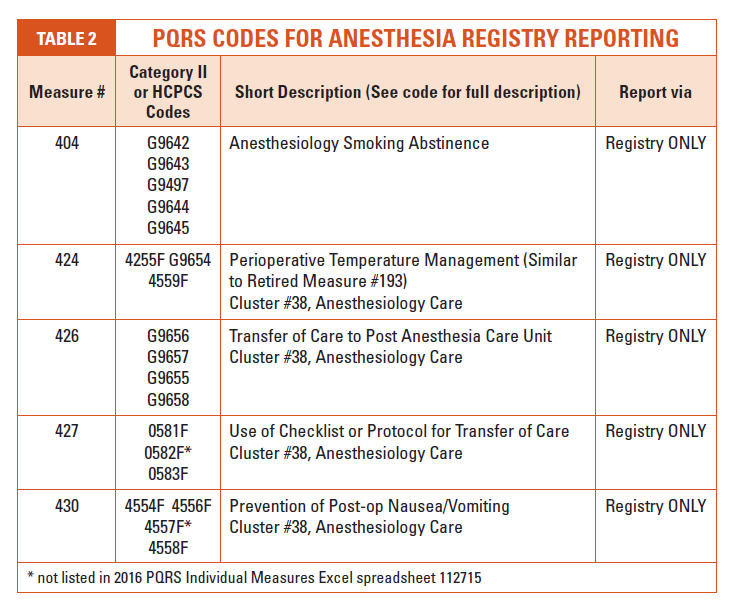
Similar to Measure #193, many of the registry-related PQRS codes include “G” codes as listed in the Healthcare Common Procedure Coding System (HCPCS) book. In 2016, there are no longer anesthesia clusters related to claims-based reporting. Cluster Number 38, Anesthesiology Care (for Registry-Based Measures), includes Measures #424, #426, #427 and #428 (See Table 2).
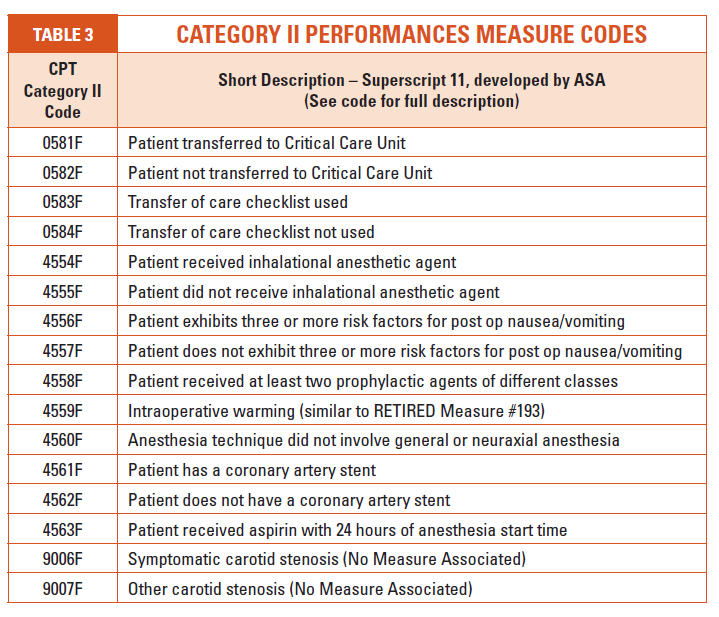
Also, take a few minutes to thumb through the Category II performance measure codes listed in the 2016 CPT. The ASA has been working on developing specific measures relative to quality reporting of anesthesia services (see superscript number 11 under Category II footnotes). Many of these codes appeared in the 2014 CPT and several may look familiar to anesthesia coders. Codes listed in Table 3 are Category II performance measure codes developed by the ASA, although these codes are reported only through a registry.
By 2019, coders will see PQRS segue into a new quality program called the Merit-Based Incentive Payment System (MIPS). Whether you are a seasoned coder or new to the specialty, anesthesia coding will continue to be unique, interesting and challenging!
Resources
2016 Professional Edition CPT American Medical Association
2016 Relative Value Guide and Crosswalk, American Society of Anesthesiologist
Hyperlink Resources
American Society of Anesthesiologist (ASA), Standards and Guidelines
http://www.asahq.org/quality-and-practice-management/standards-and-guidelines
ASA, Physician Quality Reporting System Reporting for 2016
http://www.asahq.org/quality-and-practice-management/quality-improvement/physician-quality-reporting-system/PQRS-2016-Notice
CMS Anesthesiologists Center, 2014 Anesthesia Base Units by CPT Code [Zip 13KB] (latest published information, unchanged for 2016 and 2016)
https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PhysicianFeeSched/Downloads/2014-Anesthesia-BaseUnits-CPT.zip
CMS, Final Rule containing Revisions to Payment Policies under the Physician Fee Schedule and Other Revisions to Part B for CY 2016
http://www.gpo.gov/fdsys/pkg/FR-2015-11-16/pdf/2015-28005.pdf
CMS, 2016 Cross Cutting Measures List
https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/PQRS/Downloads/2016_PQRS-Crosscutting.pdf
CMS, 2016 PQRS Claims/Registry Measure Specifications Release Notes https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/PQRS/Downloads/2016_PQRS_IndivMeasures_ReleaseNotes_111715.pdf
CMS, PQRS MAV Process for Registry Based Reporting
https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/PQRS/Downloads/2016_PQRS_IndivMeasures_Guide_11_17_2015.pdf
CMS, PQRS Measures Codes
https://www.cms.gov/medicare/quality-initiatives-patient-assessment-instruments/pqrs/measurescodes.html
CMS, Qualified Clinical Data Registry Reporting
https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/PQRS/Qualified-Clinical-Data-Registry-Reporting.html
Ronald Hirsch, MD, FACP, CHCQM. New Guidance on Pacemakers Come with Needless Modifier: RAC Monitor, March, 2015
http://www.racmonitor.com/rac-enews/1803-new-guidance-on-pacemakers-comes-with-needless-modifier.html
Michael Grasso, III, MD. Extracorporeal Shockwave Lithotripsy, January, 2015 http://emedicine.medscape.com/article/444554-overview
MLN Matters Number MM9078, NCD for Single Chamber and Dual Chamber Permanent Cardiac Pacemakers, October, 2015
https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/downloads/MM9078.pdf
Noridian, NCD for Single Chamber and Dual Chamber Permanent Cardiac Pacemakers - Revised https://med.noridianmedicare.com/web/jeb/article-detail/-/view/10542/ncd-for-single-chamber-and-dual-chamber-permanent-cardiac-pacemakers-revised
Armin Schubert MD, MBA. Positioning Injuries in Anesthesia: An Update. Advances in Anesthesia. Volume 26, October 2008, Pages 31-65
https://www.openanesthesia.org/craniotomy_positioning_injury/
 Kelly D. Dennis, MBA, ACS-AN, CANPC, CHCA, CPC, CPC-I has over 32 years experience in anesthesia and speaks about anesthesia issues nationally. She has a Master’s Degree in Business Administration, is certified through the American Academy of Professional Coders, is an Advanced Coding Specialist for the Board of Medical Specialty Coding and serves as lead advisor for their anesthesia board. She is also a certified healthcare auditor and has owned her own consulting company, Perfect Office Solutions, Inc., since November, 2001. She can be reached at kellyddennis@attglobal.net.
Kelly D. Dennis, MBA, ACS-AN, CANPC, CHCA, CPC, CPC-I has over 32 years experience in anesthesia and speaks about anesthesia issues nationally. She has a Master’s Degree in Business Administration, is certified through the American Academy of Professional Coders, is an Advanced Coding Specialist for the Board of Medical Specialty Coding and serves as lead advisor for their anesthesia board. She is also a certified healthcare auditor and has owned her own consulting company, Perfect Office Solutions, Inc., since November, 2001. She can be reached at kellyddennis@attglobal.net.