As we write this Alert on Christmas Day, we are thinking about the tumultuous year gone by. So much is changing so fast that it’s hard to stop long enough to catch our breath. Below are some of the developments through 2014 that are going to shape our future, immediate and long-term. Inclusion of a particular change or trend does not mean that it was necessarily among the most important; nor does omission mean that a given development was less momentous. There are far too many issues for an exhaustive list.
Anesthesia
The Perioperative Surgical Home (PSH). The PSH model of care—a patient-centered, physician-led system of coordinated care striving for better health, better health care and reduced costs of care—gained traction throughout 2014. In April, ASA announced the selection of Premier, Inc. to develop a first-of-its-kind learning collaborative for the PSH. The first learning collaborative cohort consists of 44 provider organizations currently...
 Since establishing ProSTAT in 1995, I have had the pleasure of working for more than 325 hospitals/health systems, physician-owned and Certified Registered Nurse Anesthetist (CRNA)-owned anesthesia practices, academic medical centers and related anesthesia businesses in 46 states and the District of Columbia.
My consulting business has evolved over the years from an exclusive focus on anesthesia group practice to one that now include hospitals and health systems (just over 150 at last count). That evolution has helped me better understand the viewpoints and value structure of hospital leaders as I spend time in their offices now discussing anesthesia challenges, solutions and strategies for the future with their perspective in mind. It is the substance of those detailed discussions that I hope to share with you in this article.
Five to ten years ago, I feel safe in saying, many (though not all) anesthesia practices didn’t place a top priority on what...
Since establishing ProSTAT in 1995, I have had the pleasure of working for more than 325 hospitals/health systems, physician-owned and Certified Registered Nurse Anesthetist (CRNA)-owned anesthesia practices, academic medical centers and related anesthesia businesses in 46 states and the District of Columbia.
My consulting business has evolved over the years from an exclusive focus on anesthesia group practice to one that now include hospitals and health systems (just over 150 at last count). That evolution has helped me better understand the viewpoints and value structure of hospital leaders as I spend time in their offices now discussing anesthesia challenges, solutions and strategies for the future with their perspective in mind. It is the substance of those detailed discussions that I hope to share with you in this article.
Five to ten years ago, I feel safe in saying, many (though not all) anesthesia practices didn’t place a top priority on what...
It is rare that a patient’s conduct drives his or her physician to terminate the relationship, but it does happen—not necessarily in anesthesiology care, where ongoing patient relationships are the exception, but certainly in chronic pain practices. Such an ending is uncomfortable for all the parties involved. There are ways, however, to make the process smoother and less fraught with risk for the practice.
First, what is the risk? Medical ethics and the medico-legal theory of abandonment establish the principle that once a patient engages a physician, that physician is under an obligation to provide the patient with continuous care and attention until the relationship is properly terminated. The patient may terminate at any time, for any reason. At least in those states that do not have legislation limiting the circumstances in which the physician may discharge a patient unilaterally, the physician may terminate for any non-discriminatory reason as long as...
 Using a cloud-based Meaningful Use Electronic Health Record (EHR) like F1RSTUse enables anesthesiologists to participate in either the Medicare or Medicaid EHR Incentive Programs. For those of us who have been doing this for the last few years, the incentive payments have been quite substantial. While data entry does require some time and commitment, the process is straightforward and provides additional non-financial rewards to the physician and patient. As physicians, we have the ability to document patient encounters, review patient records, generate patient lists and securely message our patients. In addition, there is now technology to securely message the growing number of other healthcare providers in the Direct Protocol messaging trust bundle.
Historically, anesthesiologists have been the unseen doctors behind the mask. Patients may be grateful for good care, but they may not remember much about the experience due to the amnestic effects of our medications and the fact that much...
Using a cloud-based Meaningful Use Electronic Health Record (EHR) like F1RSTUse enables anesthesiologists to participate in either the Medicare or Medicaid EHR Incentive Programs. For those of us who have been doing this for the last few years, the incentive payments have been quite substantial. While data entry does require some time and commitment, the process is straightforward and provides additional non-financial rewards to the physician and patient. As physicians, we have the ability to document patient encounters, review patient records, generate patient lists and securely message our patients. In addition, there is now technology to securely message the growing number of other healthcare providers in the Direct Protocol messaging trust bundle.
Historically, anesthesiologists have been the unseen doctors behind the mask. Patients may be grateful for good care, but they may not remember much about the experience due to the amnestic effects of our medications and the fact that much... 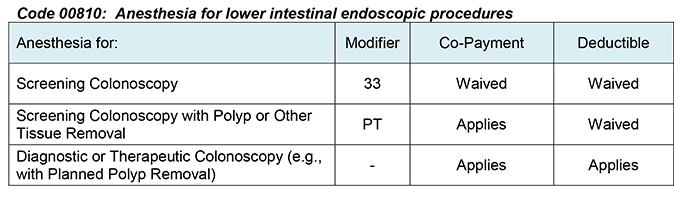 If you provide anesthesia for a Medicare patient undergoing a screening colonoscopy, you will be able to collect 100 percent of the allowable amount from Medicare and will not need to bill the patient for any co-payment or deductible, beginning on January 1, 2015. You must, however, identify the service as screening rather than diagnostic or therapeutic through the use of the appropriate modifier on your claim.
In the interest of making preventive care more widely available, a provision of the Affordable Care Act, Section 4104, waived “colorectal cancer screening test” co-payments and deductibles for Medicare beneficiaries. For the same reason—to avoid patient cost-sharing’s becoming “a significant barrier to these essential preventive services”—CMS extended the waiver of coinsurance and deductible to anesthesia services furnished in conjunction with a screening colonoscopy in the Final Rule on the Physician Fee Schedule for 2015.
As CMS observed,
A recent study in The Journal of...
If you provide anesthesia for a Medicare patient undergoing a screening colonoscopy, you will be able to collect 100 percent of the allowable amount from Medicare and will not need to bill the patient for any co-payment or deductible, beginning on January 1, 2015. You must, however, identify the service as screening rather than diagnostic or therapeutic through the use of the appropriate modifier on your claim.
In the interest of making preventive care more widely available, a provision of the Affordable Care Act, Section 4104, waived “colorectal cancer screening test” co-payments and deductibles for Medicare beneficiaries. For the same reason—to avoid patient cost-sharing’s becoming “a significant barrier to these essential preventive services”—CMS extended the waiver of coinsurance and deductible to anesthesia services furnished in conjunction with a screening colonoscopy in the Final Rule on the Physician Fee Schedule for 2015.
As CMS observed,
A recent study in The Journal of...  I. Background
The medical specialty of anesthesiology is recognized for being in the forefront of adopting technology to enhance patient safety. The rapid dissemination of pulse oximetry and capnonography in anesthetic practice are two classic examples of early adoption of technology by the medical community to make our practice safer. The creation of the Anesthesia Patient Safety Foundation (APSF) further exemplifies our specialty’s commitment to both patient welfare and technological progress.
Over the past few decades, a new factor has prominently inserted itself into the equation, influencing the introduction of new technology. That is cost-effectiveness. In evaluating a new product, whether it provides ideal patient care or cost-effective care may give different answers.
The professional cost of anesthesia services is only a small percentage of total physician services (three percent of Medicare spending in 2010). Yet, the increase in spending on monitored anesthesia care (MAC) for esophagogastroduodenoscopy (EGD) and for colonoscopy...
I. Background
The medical specialty of anesthesiology is recognized for being in the forefront of adopting technology to enhance patient safety. The rapid dissemination of pulse oximetry and capnonography in anesthetic practice are two classic examples of early adoption of technology by the medical community to make our practice safer. The creation of the Anesthesia Patient Safety Foundation (APSF) further exemplifies our specialty’s commitment to both patient welfare and technological progress.
Over the past few decades, a new factor has prominently inserted itself into the equation, influencing the introduction of new technology. That is cost-effectiveness. In evaluating a new product, whether it provides ideal patient care or cost-effective care may give different answers.
The professional cost of anesthesia services is only a small percentage of total physician services (three percent of Medicare spending in 2010). Yet, the increase in spending on monitored anesthesia care (MAC) for esophagogastroduodenoscopy (EGD) and for colonoscopy...
Is your anesthesia or pain medicine practice participating in any bundled payment programs? Bundled payments are single payments to providers or health care facilities (or to a combination of both) for all services furnished during an episode of care or over a certain time period. Distribution of the single payment among the providers often entails a gainsharing and/or pay-for-performance arrangement to incentivize cost reduction and improve quality of care. With many bundled payment packages including orthopedic, spine or cardiovascular service lines, it is almost certain that some anesthesiologists are involved.
More than 243 providers had entered into bundled payment contracts with CMS under Phase II of the Medicare Bundled Payments for Care Improvement (BPCI) Initiative as of July 2014. More than 6,400 providers participated in Phase I. According to CMS, some 6,500 providers are analyzing Medicare spending data to decide whether to apply to enter into BPCI contracts. Although the ability...
 By now, many readers of the ABC Communiqué will have heard about the Qualified Clinical Data Registry (QCDR) and will be wondering (or dreading) what this means for them and their practice. This article will lay out the basic definitions and requirements.
The QCDR is a new mechanism for eligible professionals (EPs) to report data on their performance to the Centers for Medicare and Medicaid Services (CMS). CMS currently reimburses about one-third of anesthesia care in the United States, and almost every practice derives a portion of its income from CMS. As a federal agency, CMS has been at the forefront of responding to public demand for transparent reporting of healthcare quality from both hospitals and providers. This has led to a steadily escalating requirement for performance reporting.
Under the QCDR, EPs contributing data to a clinical registry can get credit for meeting the requirements of the Physician Quality Reporting System...
By now, many readers of the ABC Communiqué will have heard about the Qualified Clinical Data Registry (QCDR) and will be wondering (or dreading) what this means for them and their practice. This article will lay out the basic definitions and requirements.
The QCDR is a new mechanism for eligible professionals (EPs) to report data on their performance to the Centers for Medicare and Medicaid Services (CMS). CMS currently reimburses about one-third of anesthesia care in the United States, and almost every practice derives a portion of its income from CMS. As a federal agency, CMS has been at the forefront of responding to public demand for transparent reporting of healthcare quality from both hospitals and providers. This has led to a steadily escalating requirement for performance reporting.
Under the QCDR, EPs contributing data to a clinical registry can get credit for meeting the requirements of the Physician Quality Reporting System...  CMS has raised hackles in the physician community by finalizing its proposal to eliminate 10- and 90-day global surgical periods beginning in 2017 (Final Fee Schedule Rule). All procedures would have a zero-day global period by 2018. While the change will not affect anesthesia services or most pain medicine practices, it is of great concern to surgeons—and their anesthesiology colleagues should therefore be conversant with the issues.
The Global Surgical Package
The global surgical package includes all necessary services normally furnished by a surgeon before, during and after a procedure. Medicare payment for the surgical procedure includes the preoperative, intra-operative and postoperative services routinely performed by the surgeon or by members of the same group with the same specialty, whether provided in the inpatient, outpatient, ambulatory surgery center (ASC) or office setting. There are no global periods for anesthesia services, but most pain medicine procedures are subject to the policy.
There...
CMS has raised hackles in the physician community by finalizing its proposal to eliminate 10- and 90-day global surgical periods beginning in 2017 (Final Fee Schedule Rule). All procedures would have a zero-day global period by 2018. While the change will not affect anesthesia services or most pain medicine practices, it is of great concern to surgeons—and their anesthesiology colleagues should therefore be conversant with the issues.
The Global Surgical Package
The global surgical package includes all necessary services normally furnished by a surgeon before, during and after a procedure. Medicare payment for the surgical procedure includes the preoperative, intra-operative and postoperative services routinely performed by the surgeon or by members of the same group with the same specialty, whether provided in the inpatient, outpatient, ambulatory surgery center (ASC) or office setting. There are no global periods for anesthesia services, but most pain medicine procedures are subject to the policy.
There...  Healthcare is always changing and ambulatory surgery centers (ASCs) are in a great position to take advantage of the new care philosophy: providing the best quality for the lowest cost. However, that’s only if they can overcome some of the bigger market challenges facing ASCs today:
1. Transitioning to value-based care. ASCs traditionally depended on volume to drive their bottom line, but healthcare is moving more toward pay-for-performance instead of fee-for-service. Bundled payments, accountable care organizations (ACOs) and shared savings programs all promote outcomes over volume and require healthcare providers to take on risk.
“As payers increasingly sell health plans tied to ACOs, ASCs will progressively feel compelled to participate in ACOs as well,” says Adam C. Powell, PhD, president of Payer+Provider Syndicate. “This is likely to be particularly pronounced in high-density areas in which ACOs have a strong presence. Many ASCs will have to take a serious look at how...
Healthcare is always changing and ambulatory surgery centers (ASCs) are in a great position to take advantage of the new care philosophy: providing the best quality for the lowest cost. However, that’s only if they can overcome some of the bigger market challenges facing ASCs today:
1. Transitioning to value-based care. ASCs traditionally depended on volume to drive their bottom line, but healthcare is moving more toward pay-for-performance instead of fee-for-service. Bundled payments, accountable care organizations (ACOs) and shared savings programs all promote outcomes over volume and require healthcare providers to take on risk.
“As payers increasingly sell health plans tied to ACOs, ASCs will progressively feel compelled to participate in ACOs as well,” says Adam C. Powell, PhD, president of Payer+Provider Syndicate. “This is likely to be particularly pronounced in high-density areas in which ACOs have a strong presence. Many ASCs will have to take a serious look at how...  The last two issues of the Alert reviewed changes to the Physician Quality Reporting System (PQRS) and to the Value-Based Payment Modifier (VM) announced in the Final Fee Schedule Rule for 2015. This week we will note for the record some of the most meaningful numbers in the Final Rule—the conversion factors—and explore developments regarding two of CMS’ transparency ventures, the Physician Compare website and the Open Payments program.
Conversion Factors for 2015
The Final Rule announced two different conversion factors (CFs) for each of two different periods: January 1 through March 31, 2015 and April 1st onward. On April 1st, unless Congress enacts yet another fix to the Sustainable Growth Rate (SGR) formula, the delayed 21.2-percent cut will go into effect. The CFs for the two periods are:
The figures for the first three-month period are slightly different from the CFs for 2014 because of required budget neutrality adjustments and...
The last two issues of the Alert reviewed changes to the Physician Quality Reporting System (PQRS) and to the Value-Based Payment Modifier (VM) announced in the Final Fee Schedule Rule for 2015. This week we will note for the record some of the most meaningful numbers in the Final Rule—the conversion factors—and explore developments regarding two of CMS’ transparency ventures, the Physician Compare website and the Open Payments program.
Conversion Factors for 2015
The Final Rule announced two different conversion factors (CFs) for each of two different periods: January 1 through March 31, 2015 and April 1st onward. On April 1st, unless Congress enacts yet another fix to the Sustainable Growth Rate (SGR) formula, the delayed 21.2-percent cut will go into effect. The CFs for the two periods are:
The figures for the first three-month period are slightly different from the CFs for 2014 because of required budget neutrality adjustments and...  Compensation packages for senior practice administrators in large, private anesthesia groups can be well into six figures. That’s a lot of money, but are they really worth it? During this time of turmoil in the healthcare market where there is tremendous pressure on all healthcare providers, including doctors, to do more for less, does it make sense to pay one individual so much money? Each anesthesia practice must decide who they want to help run their business and how much they should be paid. However, the following issues should be a part of the equation.
The business side of anesthesia is very complicated. Anesthesiologist, CRNA and AA recruiting and retention. Scheduling. Retirement plans and health insurance benefits. Employee policies and enforcement. Managed care and hospital contracting. Revenue cycle management (billing and collections). Coding. Compliance. Accounting. Payroll. Risk management (lawsuits) and insurance. Continuous quality improvement. Computer and communication systems. Strategic planning...
Compensation packages for senior practice administrators in large, private anesthesia groups can be well into six figures. That’s a lot of money, but are they really worth it? During this time of turmoil in the healthcare market where there is tremendous pressure on all healthcare providers, including doctors, to do more for less, does it make sense to pay one individual so much money? Each anesthesia practice must decide who they want to help run their business and how much they should be paid. However, the following issues should be a part of the equation.
The business side of anesthesia is very complicated. Anesthesiologist, CRNA and AA recruiting and retention. Scheduling. Retirement plans and health insurance benefits. Employee policies and enforcement. Managed care and hospital contracting. Revenue cycle management (billing and collections). Coding. Compliance. Accounting. Payroll. Risk management (lawsuits) and insurance. Continuous quality improvement. Computer and communication systems. Strategic planning...  CMS released the Final Rule on the Physician Fee Schedule containing next year’s Physician Quality Reporting System (PQRS) requirements on October 31, 2014. As expected, Measure #30, Timing of Antibiotic Prophylaxis-Administering Physician, has been deleted from the list of measures available for either claims-based or registry reporting. So has the Back Pain Measures Group (Measures ##148-151) and Measure #142, Assessment for Use of Anti-Inflammatory or Analgesic Over-the-Counter (OTC) Medications, but CMS did not ultimately remove Measure #109, Osteoarthritis: Function and Pain Assessment, from the list.
For 2015, the following are the basic PQRS measures applicable to anesthesiology:
And the following is a sample of PQRS measures that may be applicable to your pain medicine practice:
Please note that neither of these lists necessarily represents the complete universe of measures that you may be able to report. There may be others that also apply to your practice, and there may be measures groups that you would choose...
CMS released the Final Rule on the Physician Fee Schedule containing next year’s Physician Quality Reporting System (PQRS) requirements on October 31, 2014. As expected, Measure #30, Timing of Antibiotic Prophylaxis-Administering Physician, has been deleted from the list of measures available for either claims-based or registry reporting. So has the Back Pain Measures Group (Measures ##148-151) and Measure #142, Assessment for Use of Anti-Inflammatory or Analgesic Over-the-Counter (OTC) Medications, but CMS did not ultimately remove Measure #109, Osteoarthritis: Function and Pain Assessment, from the list.
For 2015, the following are the basic PQRS measures applicable to anesthesiology:
And the following is a sample of PQRS measures that may be applicable to your pain medicine practice:
Please note that neither of these lists necessarily represents the complete universe of measures that you may be able to report. There may be others that also apply to your practice, and there may be measures groups that you would choose...  No fewer than four experts in anesthesia practice management have contributed articles to the Communiqué for the first time in this issue. We are struck—not for the first time—at both the vast knowledge reservoir in our community and the generosity of so many professionals who go the extra mile to share their expertise. Let us take this opportunity to thank our regular authors and especially newcomers Danielle Reicher, MD; Steve Boggs, MD; Pat Everett, CPA, CMPE and Ron Booker, JD, CPA.
Anesthesiologists have been seeking out the best electronic health record systems (EHRs) to improve data collection for both clinical and administrative purposes, not to mention for purposes of qualifying for the Medicare Meaningful Use payment incentives. Dr. Reicher describes a specific and very important application of EHR technology in Making Meaningful Use More Meaningful: communicating with patients. Have you thought about the value to the patient of documenting the medications and doses given...
No fewer than four experts in anesthesia practice management have contributed articles to the Communiqué for the first time in this issue. We are struck—not for the first time—at both the vast knowledge reservoir in our community and the generosity of so many professionals who go the extra mile to share their expertise. Let us take this opportunity to thank our regular authors and especially newcomers Danielle Reicher, MD; Steve Boggs, MD; Pat Everett, CPA, CMPE and Ron Booker, JD, CPA.
Anesthesiologists have been seeking out the best electronic health record systems (EHRs) to improve data collection for both clinical and administrative purposes, not to mention for purposes of qualifying for the Medicare Meaningful Use payment incentives. Dr. Reicher describes a specific and very important application of EHR technology in Making Meaningful Use More Meaningful: communicating with patients. Have you thought about the value to the patient of documenting the medications and doses given...  On Friday, October 31, CMS released the Final Rule with Revisions to Payment Policies under the Physician Fee Schedule for 2015. Among numerous changes in the Final Rule are important modifications to the Value-Based Payment Modifier (VM).
Beginning on January 1, 2015, consistent with the Affordable Care Act and CMS’ proposals, the VM will affect all eligible professionals (EPs)— anesthesiologists, nurse anesthetists and anesthesiologist assistants among them.
For the great majority of anesthesia practices, the VM matters for one principal reason, that it will apply an additional payment cut to EPs who do not satisfactorily participate in the Physician Quality Reporting System (PQRS). This cut would be four percent for groups of ten or more EPs and two percent for groups with two to nine EPs and solo practitioners. Thus failure to report under the PQRS in 2015 could cost an EP (in a practice with ten or more EPs) a total of six...
On Friday, October 31, CMS released the Final Rule with Revisions to Payment Policies under the Physician Fee Schedule for 2015. Among numerous changes in the Final Rule are important modifications to the Value-Based Payment Modifier (VM).
Beginning on January 1, 2015, consistent with the Affordable Care Act and CMS’ proposals, the VM will affect all eligible professionals (EPs)— anesthesiologists, nurse anesthetists and anesthesiologist assistants among them.
For the great majority of anesthesia practices, the VM matters for one principal reason, that it will apply an additional payment cut to EPs who do not satisfactorily participate in the Physician Quality Reporting System (PQRS). This cut would be four percent for groups of ten or more EPs and two percent for groups with two to nine EPs and solo practitioners. Thus failure to report under the PQRS in 2015 could cost an EP (in a practice with ten or more EPs) a total of six...  The Centers for Medicare & Medicaid Services (CMS) began the National Correct Coding Initiative (CCI) edits as an initiative to promote correct coding by providers and to prevent Medicare payment for improperly reported services. The CCI program consists of automated edits that are part of the claims processing systems deployed by the Medicare Administrative Contractors (MACs). Specifically, the CCI edits contain pairs of Healthcare Common Procedure Coding System (HCPCS) codes (i.e., code pairs) that generally should not be billed together by a provider for a patient on the same date of service. All code pairs are arranged in two columns. Column 1 contains the primary code and column 2 the secondary code or service format. The column 2 code is generally not payable with the column 1 code.
Under certain circumstances, a provider may bill the column 2 service in a CCI code pair by including a modifier on the...
The Centers for Medicare & Medicaid Services (CMS) began the National Correct Coding Initiative (CCI) edits as an initiative to promote correct coding by providers and to prevent Medicare payment for improperly reported services. The CCI program consists of automated edits that are part of the claims processing systems deployed by the Medicare Administrative Contractors (MACs). Specifically, the CCI edits contain pairs of Healthcare Common Procedure Coding System (HCPCS) codes (i.e., code pairs) that generally should not be billed together by a provider for a patient on the same date of service. All code pairs are arranged in two columns. Column 1 contains the primary code and column 2 the secondary code or service format. The column 2 code is generally not payable with the column 1 code.
Under certain circumstances, a provider may bill the column 2 service in a CCI code pair by including a modifier on the...
Numerous anesthesiologists have expressed confusion about the requirements for reporting Physician Quality Reporting System (PQRS) measures next year. It is very important that every eligible professional (EP) successfully participate in the PQRS program in 2015; failure to do so will mean a two-percent reduction in their Medicare payments in 2017.
There are five methods for submitting PQRS data to CMS:
Claims-based reporting (on Medicare Part B claims)
Registry-based reporting
Electronic health record (EHR) reporting using certified EHR technology (CEHRT) or a data submission vendor
Qualified clinical data registry (QCDR) reporting
Group practice reporting
While these methods have all been established previously, and none of them are new for 2015, CMS has proposed significant changes to the numbers and types of measures that must be reported to avoid the penalties. We will not know for certain whether it will suffice to report one measure, three measures or nine measures as proposed until...
 The Affordable Care Act (ACA) was passed four years ago and there have been plenty of ups and downs regarding its rollout. Now that it appears to be here to stay, healthcare providers need to change their focus on the impact the new health insurance exchanges may have on their financial bottom line.
Individuals who buy coverage on the Marketplace and fall below certain income levels can qualify for advance payments of a premium tax credit (APTC) to help pay their premiums. As long as these individuals pay their share of the first month of premium, insurers cannot later terminate their coverage without first giving a three-month (90-day) grace period to pay. The Obama Administration saw this rule as a means to further the continuity of care for those who cannot afford premiums for certain months due to job loss or other financial constraints. Many healthcare experts see the grace...
The Affordable Care Act (ACA) was passed four years ago and there have been plenty of ups and downs regarding its rollout. Now that it appears to be here to stay, healthcare providers need to change their focus on the impact the new health insurance exchanges may have on their financial bottom line.
Individuals who buy coverage on the Marketplace and fall below certain income levels can qualify for advance payments of a premium tax credit (APTC) to help pay their premiums. As long as these individuals pay their share of the first month of premium, insurers cannot later terminate their coverage without first giving a three-month (90-day) grace period to pay. The Obama Administration saw this rule as a means to further the continuity of care for those who cannot afford premiums for certain months due to job loss or other financial constraints. Many healthcare experts see the grace...
Anesthesia time “starts when the anesthesia practitioner begins to prepare the patient for anesthesia services in the operating room or an equivalent area,” according to the Medicare regulations and the ASA Relative Value Guide®, or “begins to prepare the patient for the induction of anesthesia” as stated in the CPT® Anesthesia Guidelines. What do those words mean—and can there be any remaining controversies after all these years?
To “begin to prepare the patient” involves “doing something to the patient” or placing “hands on,” in the memorable words of a former chair of the ASA Committee on Economics. Thus anesthesia time starts with an intervention performed after completion of the preoperative assessment, whether that assessment is done in the holding area or in the operating room itself. The start of anesthesia time occurs before anesthesia is induced. Our concern is with the period of time from the first act of physical preparation, such as the placement of...
 Date night with my husband usually involves going out to one of our favorite restaurants where we get to enjoy each other’s company in a relaxed atmosphere without worrying about who’s doing the dishes. So how can a night out at a restaurant have anything in common with having a total joint replacement?
My husband and I feel that every waiter or waitress generally deserves a 20 percent tip. From the time we get seated at the table to the time we pay the tab, my husband and I are unconsciously measuring both the restaurant’s and the servers’ performance and quality. We are not concerned about the fact that our waitress has to go to the bar for our glasses of wine or that the bartender may be busy serving happy hour drinks; we just want our drinks timely and exactly as we ordered. Same goes for the food we order....
Date night with my husband usually involves going out to one of our favorite restaurants where we get to enjoy each other’s company in a relaxed atmosphere without worrying about who’s doing the dishes. So how can a night out at a restaurant have anything in common with having a total joint replacement?
My husband and I feel that every waiter or waitress generally deserves a 20 percent tip. From the time we get seated at the table to the time we pay the tab, my husband and I are unconsciously measuring both the restaurant’s and the servers’ performance and quality. We are not concerned about the fact that our waitress has to go to the bar for our glasses of wine or that the bartender may be busy serving happy hour drinks; we just want our drinks timely and exactly as we ordered. Same goes for the food we order....