Anesthesia Business Consultants (ABC) is pleased to announce its latest partnership with the Louisiana State University Health Science Center Shreveport Department of Anesthesiology (LSUHSC – Shreveport). The Department of Anesthesiology at LSUHSC – Shreveport is a part of a world class university and thriving medical school that is committed to being a center of excellence in educational training in anesthesiology, critical care medicine and interventional pain management along with providing innovative programs to develop management skills and future leaders in the specialty of anesthesiology. ABC is thrilled to support LSUHSC – Shreveport Department of Anesthesiology with their billing operations, as well as other programs, into the future.“The Louisiana State University Health Science Center, Shreveport Department of Anesthesiology is excited about the ability to work with the premier anesthesia billing and consulting company for our specialty. They possess a wealth of experience and expertise which will provide a multitude of benefits for...
 Are the standard measures of health care quality—structure, process and even outcomes—all that good?
A generation ago, many observers doubted that the tools of quality measurement could be applied at all in healthcare. Now we have moved beyond the belief that “we know quality when we see it.” We have acknowledged the limitations of structure (e.g., clinician training) and process (e.g., maintenance of normothermia in anesthetized patients) measures. We have placed the emphasis on outcomes and have created considerable numbers of performance measures to assess clinical outcomes. Yet, when we examine and compare performance scores across providers, the information is not always convincing. Varying definitions of outcomes, and the underdeveloped state of risk adjustment methodologies are just some of the factors that make quality data unreliable in many cases. Quality measurement in healthcare has come a considerable distance, but it still has a long way to go.
That may be the reason for...
Are the standard measures of health care quality—structure, process and even outcomes—all that good?
A generation ago, many observers doubted that the tools of quality measurement could be applied at all in healthcare. Now we have moved beyond the belief that “we know quality when we see it.” We have acknowledged the limitations of structure (e.g., clinician training) and process (e.g., maintenance of normothermia in anesthetized patients) measures. We have placed the emphasis on outcomes and have created considerable numbers of performance measures to assess clinical outcomes. Yet, when we examine and compare performance scores across providers, the information is not always convincing. Varying definitions of outcomes, and the underdeveloped state of risk adjustment methodologies are just some of the factors that make quality data unreliable in many cases. Quality measurement in healthcare has come a considerable distance, but it still has a long way to go.
That may be the reason for... 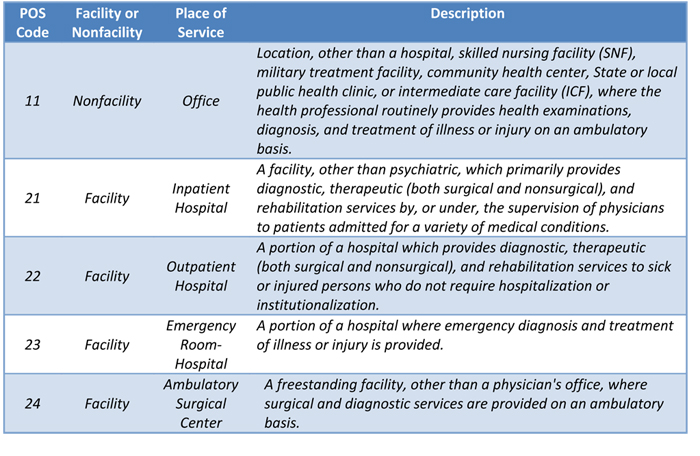 The Office of the Inspector General (OIG) reported in May 2015 that Medicare made up to $33.4 million in overpayments for claims on which the place of service (POS) was coded incorrectly during the period from January 2010 through September 2012. (Incorrect Place-of-Service Claims Resulted in Potential Medicare Overpayment Costing Millions.) Reports finding that Medicare has overpaid usually lead to heightened scrutiny of the conduct at issue. Thus it is important that pain physicians, anesthesiologists and their billing staff understand POS coding.
The Medicare Physician Fee Schedule provides for payment at a higher rate for services performed in doctors’ private offices (the “nonfacility” rate) than for the same services performed in a “facility” such as a hospital or ambulatory surgical center (ASC). The difference accounts for the increased practice expense that physicians generally incur by providing care in their offices and other nonfacility locations, including private clinics. When a physician provides...
The Office of the Inspector General (OIG) reported in May 2015 that Medicare made up to $33.4 million in overpayments for claims on which the place of service (POS) was coded incorrectly during the period from January 2010 through September 2012. (Incorrect Place-of-Service Claims Resulted in Potential Medicare Overpayment Costing Millions.) Reports finding that Medicare has overpaid usually lead to heightened scrutiny of the conduct at issue. Thus it is important that pain physicians, anesthesiologists and their billing staff understand POS coding.
The Medicare Physician Fee Schedule provides for payment at a higher rate for services performed in doctors’ private offices (the “nonfacility” rate) than for the same services performed in a “facility” such as a hospital or ambulatory surgical center (ASC). The difference accounts for the increased practice expense that physicians generally incur by providing care in their offices and other nonfacility locations, including private clinics. When a physician provides...  The Comprehensive Error Rate Testing (CERT) Program is designed to measure improper payments in the Medicare Fee for Service Program (FFS), as required by the Improper Payments Information Act of 2002. The Program was initiated by Health and Human Services (HHS) Centers for Medicare and Medicaid Services (CMS) to achieve the agency’s mission to emphasize accountability and to pay claims appropriately. The Program produces national, contractor-specific and service-specific paid claim error rates, as well as a provider compliance error rate. The improper paid claim error rate is a measure of the extent to which the Medicare program is paying claims correctly. The provider compliance improper error rate is a measure of the extent to which providers are submitting claims correctly.
The fiscal year (FY) 2014 Medicare FFS program improper payment rate is 12.7 percent, representing $45.8 billion in improper payments, compared to the FY 2013 improper payment rate of 10.1 percent...
The Comprehensive Error Rate Testing (CERT) Program is designed to measure improper payments in the Medicare Fee for Service Program (FFS), as required by the Improper Payments Information Act of 2002. The Program was initiated by Health and Human Services (HHS) Centers for Medicare and Medicaid Services (CMS) to achieve the agency’s mission to emphasize accountability and to pay claims appropriately. The Program produces national, contractor-specific and service-specific paid claim error rates, as well as a provider compliance error rate. The improper paid claim error rate is a measure of the extent to which the Medicare program is paying claims correctly. The provider compliance improper error rate is a measure of the extent to which providers are submitting claims correctly.
The fiscal year (FY) 2014 Medicare FFS program improper payment rate is 12.7 percent, representing $45.8 billion in improper payments, compared to the FY 2013 improper payment rate of 10.1 percent...
On June 30, CMS is going to release information on payments made to physicians during 2014 by pharmaceutical, device and other manufacturers. This will be an update to the information made public for the first time in September, 2014. The current database is available at https://openpaymentsdata.cms.gov/.
Open Payments is a national program that promotes transparency by publishing data on the financial relationships between the health care industry (applicable manufacturers and group purchasing organizations, or GPOs) and health care providers (physicians and teaching hospitals). In 2014, CMS published 4.45 million payment records, transfers of value, or instances of ownership/investment interest that occurred over the last five months of 2013. These financial transactions totaled nearly $3.7 billion. (CMS, Annual Report to Congress on the Open Payments Program for Fiscal Year 2014.)
The program requires “applicable” manufacturers and GPOs to report payments of $10 or more, or of $100 or more per year in...
 When one reviews the Current Procedural Terminology (CPT®) changes for 2015, a recurrent theme throughout is the consolidation of code combinations. The American Medical Association/ Specialty Society Relative Value Update Committee (RUC) identifies codes that are regularly reported together more than 75 percent of the time. The identified codes are then considered by the CPT Editorial Panel for bundling. The CPT Editorial Panel consists of physicians representing all specialties and other stakeholders who are all users of the CPT code set and thus have a practical perspective on the changes presented. It is the intention of the RUC, when presenting these code combinations, to provide the logic, rationale and function of these CPT changes. The following paragraphs will explore the rationale behind the bundled codes that are related to anesthesia and pain management.
Ultrasound is often utilized to improve the accuracy of intra-articular placement of the needle for safety and better...
When one reviews the Current Procedural Terminology (CPT®) changes for 2015, a recurrent theme throughout is the consolidation of code combinations. The American Medical Association/ Specialty Society Relative Value Update Committee (RUC) identifies codes that are regularly reported together more than 75 percent of the time. The identified codes are then considered by the CPT Editorial Panel for bundling. The CPT Editorial Panel consists of physicians representing all specialties and other stakeholders who are all users of the CPT code set and thus have a practical perspective on the changes presented. It is the intention of the RUC, when presenting these code combinations, to provide the logic, rationale and function of these CPT changes. The following paragraphs will explore the rationale behind the bundled codes that are related to anesthesia and pain management.
Ultrasound is often utilized to improve the accuracy of intra-articular placement of the needle for safety and better...  Post-acute care services are a major driver of spending, particularly for the Medicare population. Nationwide, one in seven surgical patients is readmitted within 30 days, stated Michael Schweitzer, MD, MBA, who chairs ASA’s Future Models of Anesthesia Practice task force and who gave a very thought-provoking talk on “The Future of Anesthesia Practice” at the MGMA Anesthesia Conference in Chicago on May 1, 2015.
Such readmissions are difficult for patients—and they are costly. In 2009, the average cost of a total hip replacement readmission was $12,300, with an 8.2 percent readmission rate. (Rizzo E. 6 Stats of the Cost of Readmission for CMS-Tracked Conditions. Becker’s Hospital Review, December 12, 2013.) Dr. Schweitzer cited a study published in Health Affairs in 2012 showing that surgical complications could increase the costs of care up to $58,000 per case.
One out of every six Medicare fee-for-service program dollars goes to care provided in rehabilitation...
Post-acute care services are a major driver of spending, particularly for the Medicare population. Nationwide, one in seven surgical patients is readmitted within 30 days, stated Michael Schweitzer, MD, MBA, who chairs ASA’s Future Models of Anesthesia Practice task force and who gave a very thought-provoking talk on “The Future of Anesthesia Practice” at the MGMA Anesthesia Conference in Chicago on May 1, 2015.
Such readmissions are difficult for patients—and they are costly. In 2009, the average cost of a total hip replacement readmission was $12,300, with an 8.2 percent readmission rate. (Rizzo E. 6 Stats of the Cost of Readmission for CMS-Tracked Conditions. Becker’s Hospital Review, December 12, 2013.) Dr. Schweitzer cited a study published in Health Affairs in 2012 showing that surgical complications could increase the costs of care up to $58,000 per case.
One out of every six Medicare fee-for-service program dollars goes to care provided in rehabilitation...  Medscape is one of the very few organizations that surveys physicians on compensation and practice patterns, breaks out the specialty of anesthesiology and publishes the results for free. The Medscape Anesthesiologist Compensation Report also has one of the larger absolute response rates; in the most recent survey, reported in March 2015, 1179 responses were received from anesthesiologists during the period December 30, 2014 – March 11, 2015. For those reasons alone, it behooves anesthesiology practices to be familiar with the Medscape data. The sample is small. It is probably not representative. As science, the survey does not pass muster. But since there is so little information of any better quality available, the Medscape compensation surveys are being used, usually in conjunction with other surveys such as those published (and sold) by the Medical Group Management Association (MGMA) and American Medical Group Association.
The weakness of the information is slightly mitigated by...
Medscape is one of the very few organizations that surveys physicians on compensation and practice patterns, breaks out the specialty of anesthesiology and publishes the results for free. The Medscape Anesthesiologist Compensation Report also has one of the larger absolute response rates; in the most recent survey, reported in March 2015, 1179 responses were received from anesthesiologists during the period December 30, 2014 – March 11, 2015. For those reasons alone, it behooves anesthesiology practices to be familiar with the Medscape data. The sample is small. It is probably not representative. As science, the survey does not pass muster. But since there is so little information of any better quality available, the Medscape compensation surveys are being used, usually in conjunction with other surveys such as those published (and sold) by the Medical Group Management Association (MGMA) and American Medical Group Association.
The weakness of the information is slightly mitigated by... 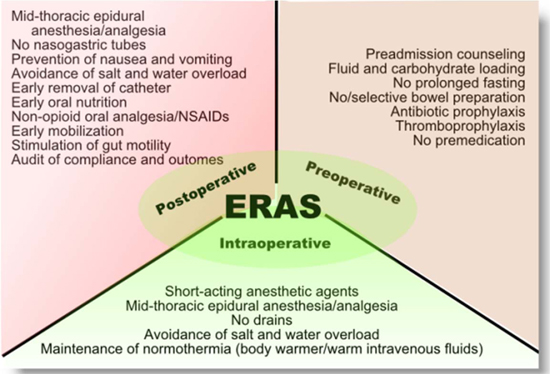 The term “Enhanced Recovery After Surgery” and the acronym ERAS are familiar to most anesthesiologists and to other clinicians. Anesthesia administrators and non-physician advisors may not have encountered the ERAS concept yet. Because of burgeoning interest in better evidence-based perioperative care protocols leading to improved patient outcomes in this era of value-based payment, administrators and practice management staff should acquire a basic understanding of the ERAS concept.
“Enhanced recovery after surgery (ERAS) protocols are multimodal perioperative care pathways designed to achieve early recovery after surgical procedures by maintaining pre-operative organ function and reducing the profound stress response following surgery. The key elements of ERAS protocols include preoperative counselling, optimization of nutrition, standardized analgesic and anesthetic regimens and early mobilization.” (M. Melnyk, RG Casey, P. Black, A.J. Koupparis. Enhanced recovery after surgery (ERAS) protocols: Time to change practice? Can Urol Assoc J. 2011 Oct; 5(5): 342–348). Also referred to as “optimized patient...
The term “Enhanced Recovery After Surgery” and the acronym ERAS are familiar to most anesthesiologists and to other clinicians. Anesthesia administrators and non-physician advisors may not have encountered the ERAS concept yet. Because of burgeoning interest in better evidence-based perioperative care protocols leading to improved patient outcomes in this era of value-based payment, administrators and practice management staff should acquire a basic understanding of the ERAS concept.
“Enhanced recovery after surgery (ERAS) protocols are multimodal perioperative care pathways designed to achieve early recovery after surgical procedures by maintaining pre-operative organ function and reducing the profound stress response following surgery. The key elements of ERAS protocols include preoperative counselling, optimization of nutrition, standardized analgesic and anesthetic regimens and early mobilization.” (M. Melnyk, RG Casey, P. Black, A.J. Koupparis. Enhanced recovery after surgery (ERAS) protocols: Time to change practice? Can Urol Assoc J. 2011 Oct; 5(5): 342–348). Also referred to as “optimized patient...
Anesthesia Business Consultants (ABC) is pleased to announce its latest partnership with the University of California at Irvine (UC Irvine). The anesthesia department at UC Irvine has long been a leader in various projects designed to promote the alignment of Anesthesiologists with their perioperative colleagues; to further the goal of supporting the entire perioperative process. ABC is thrilled to support UC Irvine with their billing operations as well as other programs into the future.“The anesthesia department at University of California, Irvine looks forward to working with Anesthesia Business Consultants. Their approach to comprehensive billing and technology platforms matches our organization's needs and strategic initiatives,” said Dr. Zeev Kain, Chancellor's Professor & Chair of the UC Irvine Department of Anesthesiology and Perioperative Care. “UC Irvine is at the forefront of improving hospital-based care with projects such as the Perioperative Surgical Home (PSH) and quality initiatives and ABC’s commitment to this specialty will...
Anesthesia Business Consultants (ABC), a leading provider in billing and practice management for the anesthesia and pain management specialty, is pleased to announce the release of its new client portal and included analytics desktop and mobile access products aimed at anesthesia practices to increase access and visibility of their practice data.ABC’s new portal, F1RSTClient™, is now available and delivers secure, seamless single-sign-on (SSO) access in a fully integrated system utilizing the powerful F1RSTAnesthesia™ and the flexibility of the F1RSTAnalytics™ series of dashboards—now available on desktops as well as mobile access.F1RSTAnesthesia is ABC's proprietary software that gives clients a powerful tool to convert clinical information into claims for reimbursement. The software supports electronic claims editing to ensure consistently high billing acceptance rates, and minimizes manual intervention in payment posting through direct remittance processing. Clients are able to access the details of their practice and to view trends securely online.F1RSTAnalytics is ABC’s Big...
 The Anesthesia Quality Institute’s Qualified Data Clinical Registry (AQI QCDR) became even more valuable with the recent addition of 16 new measures bringing the total number of measures adopted by the AQI for use in its QCDR to 27. With the nine official Medicare Physician Quality Reporting System (PQRS) measures that can also be reported to the QCDR, the combined total of 36 measures will give most anesthesiologists, nurse anesthetists and anesthesiologist assistants ample opportunity to satisfy the PQRS requirements for 2015. The array of available measures should also provide practices with sound choices for their own quality measurement and improvement programs.
PQRS Reporting via the QCDR
Eligible professionals (EPs) must successfully participate in the PQRS in 2015 in order to avoid a two-percent negative payment adjustment in 2017. Successful participation means reporting on a total of nine measures from three different National Quality Strategy (NQS) domains for at least 50...
The Anesthesia Quality Institute’s Qualified Data Clinical Registry (AQI QCDR) became even more valuable with the recent addition of 16 new measures bringing the total number of measures adopted by the AQI for use in its QCDR to 27. With the nine official Medicare Physician Quality Reporting System (PQRS) measures that can also be reported to the QCDR, the combined total of 36 measures will give most anesthesiologists, nurse anesthetists and anesthesiologist assistants ample opportunity to satisfy the PQRS requirements for 2015. The array of available measures should also provide practices with sound choices for their own quality measurement and improvement programs.
PQRS Reporting via the QCDR
Eligible professionals (EPs) must successfully participate in the PQRS in 2015 in order to avoid a two-percent negative payment adjustment in 2017. Successful participation means reporting on a total of nine measures from three different National Quality Strategy (NQS) domains for at least 50...
Anesthesia Business Consultants is pleased to announce the success of the 2nd annual Advanced Institute for Anesthesia Practice Management (AIAPM). The AIAPM was held at the Cosmopolitan Hotel in Las Vegas on April 17-19, 2015 and attracted 340 participants, an increase of nearly 10 percent over the 2014 inaugural AIAPM.During three days of plenary and breakout sessions, attendees heard presentations by 16 speakers including chief executives of national anesthesia practice management companies, private equity firm principals, academic anesthesiologists, compliance and health information technology experts and lawyers and consultants. Roundtable discussions, meals and refreshment breaks sponsored by some of the 35 exhibitors provided ample opportunity for participants to share information.The participants—practicing anesthesiologists and nurse anesthetists, anesthesia group managers and billing professionals—were highly enthusiastic about the program. Comments received on the evaluation forms included the following:Excellent conference. The topics should be mandatory education for every anesthesia provider. Appreciate the expertise of the presenters.Great...
Leadership has never been more important in anesthesiology than it is today. As the specialty demands and takes ownership of increasing levels of responsibility in healthcare reform, the quality of leadership becomes one the fundamental factors that determine success. Developing the Perioperative Surgical Home (PSH), the most exciting organizational concept to emerge within anesthesiology this century, requires outstanding leaders. So does maintaining the highest quality of patient care in each anesthesiology department or practice.
Recognizing the value of leaders and also their role in enhancing each others’ skills as well as those of the broader community, the Anesthesia Quality Institute (AQI) has created an Anesthesia Leadership Registry, a database of more than 250 ASA members who serve in leadership roles. The purposes of this registry are threefold, according to Richard P. Dutton, MD, MBA, Executive Director of the AQI (“Data, Data, and More Data—Where’s the Value?” Presentation given at the ASA...
1. Senate Passes SGR Repeal BillWe are very happy to advise you that late last night, the Senate passed the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) 92-8 and did away with the Sustainable Growth Rate (SGR) formula at long last. Had the Senate not acted, Medicare payments to physicians would have been reduced by 21.2 percent, effective April 1. Instead, Medicare payments will increase by 0.5 percent for the next five years beginning on July 1, 2015.Claims that Medicare held for services provided between April 1 and April 14, pending Senate action, will now be processed and paid at the rates that were in place during the first quarter. Other changes in the legislation include an extension of the Children's Health Insurance Program by two years as well as a consolidation of Medicare’s quality reporting programs into a single merit-based incentive payment system (MIPS). The MIPS and the...
 Let us begin with the basic answer to the question in the title of this Alert: anesthesiologists continue to benefit from a specialty-based exemption from the Electronic Health Record (EHR) Incentive Program’s “meaningful use” (MU) requirements, so only those who are have chosen to earn the incentive will be affected directly by the new Stage 3 rules. Pain physicians may be affected, unless their practice meets the EHR program definition of “hospital-based” or they have been granted a hardship exception (see Alert dated February 16, 2015).
The Stage 3 changes to the MU requirements, as described in a proposed rule issued on March 20, are part of what CMS calls its “broader efforts to increase simplicity and flexibility in the program while driving interoperability and a focus on patient outcomes in the meaningful use program.” The most significant of the changes that would be implemented beginning in 2017, if the Stage...
Let us begin with the basic answer to the question in the title of this Alert: anesthesiologists continue to benefit from a specialty-based exemption from the Electronic Health Record (EHR) Incentive Program’s “meaningful use” (MU) requirements, so only those who are have chosen to earn the incentive will be affected directly by the new Stage 3 rules. Pain physicians may be affected, unless their practice meets the EHR program definition of “hospital-based” or they have been granted a hardship exception (see Alert dated February 16, 2015).
The Stage 3 changes to the MU requirements, as described in a proposed rule issued on March 20, are part of what CMS calls its “broader efforts to increase simplicity and flexibility in the program while driving interoperability and a focus on patient outcomes in the meaningful use program.” The most significant of the changes that would be implemented beginning in 2017, if the Stage...
Cyber attacks on health databases are occurring so frequently that they are only newsworthy when they affect millions of records, as happened with the recently-reported massive Anthem (about 80 million individuals) and Premera Blue Cross (more than 11 million) data breaches. Last year, in fact, was characterized as the “year of the data breach” by some, according to Becker’s Hospital Review, which reports that: “Across industries, the healthcare sector experienced the highest percentage of breaches in 2014, according to Identity Theft Resource. Of the 761 data breaches reported last year, 322 of them came from the healthcare industry.”
These attacks are the source of personal data not just from patients’ insurance records. They are also perpetrated on physicians’ personal and financial information, which is then used to commit tax identity fraud. Physicians are an attractive target for tax fraud because their income levels and potential tax refunds are higher than average. ...
Anesthesia Practice Management conferences rarely focus on billing, coding and compliance. The AIAPM focuses on all three because we believe how important these topics are to all attendees including Anesthesiologists, CRNAs, Practice Administrators and Billing Staff. Our goal is to help all anesthesia practices maximize their reimbursements and reduce their compliance risk.The Advanced Institute for Anesthesia Practice Management will be held at the Cosmopolitan of Las Vegas from April 17-19, 2015. Please join us along with the following experts in anesthesia billing, coding and compliance:Devona Slater, CHA, CHC, CMCPPresidentAuditing for Compliance & EducationMarvel J Hammer, RN, CPC, CCS-P, ACS-PM, CHCOMJH ConsultingKelly Dennis, MBA, ACS-AN, CAN-PC, CHCA, CPC, CPC-IPerfect Office Solutions, Inc.Vicki Myckowiak, Esq.Myckowiak Associates, PCJudy Blaszczyk, RN, CPC, ACS-PMAuditing for Compliance & EducationWe also have enlisted experts to enlighten us on the following valuable topics:The Latest in the Anesthesia Merger and Acquisition MarketOne Group's Journey Through the Acquisition ProcessThe Anesthesiologist's Role...
Once more, the law preventing the Sustainable Growth Rate (SGR) formula from wreaking havoc on Medicare payments to physicians is about to expire. Payments are scheduled to decrease by 21.2 percent on April 1.
On Thursday, March 26, the House of Representatives voted overwhelmingly 392-37 in favor of the bipartisan Medicare Access and CHIP Reauthorization Act (H.R. 2), which had already received an enthusiastic response from physician organizations, as well as strong support from President Obama. On Friday, disappointingly, the Senate recessed without taking action on the bill. The pressure is on for the Senate to bring the legislation to a vote soon after it reconvenes on April 13, and many observers expect passage. We at ABC encourage all our readers to contact their Senators during this recess and urge them to support the legislation so that the SGR goes to its grave at long last.
In the short term, CMS...
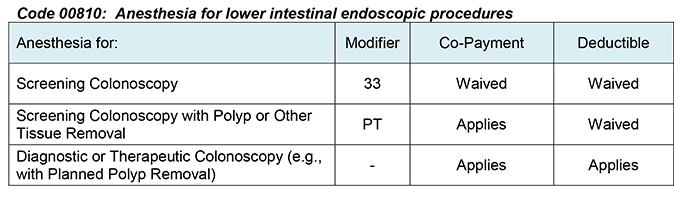 The New York Attorney General announced, on March 11, 2015, that his office had entered into a settlement agreement with EmblemHealth, Inc., requiring the health plan to cover anesthesiology services provided in connection with an in-network preventive colonoscopy, without any cost-sharing by the patient. The agreement includes a $25,000 penalty and applies not just prospectively but also requires Emblem to send nearly $400,000 of reimbursements to 255 patients who were inappropriately charged co-payments.
The Affordable Care Act (ACA) requires health plans to provide first-dollar coverage for colorectal cancer screening tests and certain other preventive care services, waiving any patient co-insurance, co-payments or deductible amounts. The Emblem agreement expressly extends the requirement to anesthesia for screening colonoscopies: “Because colonoscopies necessitate the administration of anesthesia, anesthesia services provided in connection with preventive colonoscopies should likewise be covered without member cost-sharing.”
In the final Physician Fee Schedule rule for 2015, the Centers for Medicare...
The New York Attorney General announced, on March 11, 2015, that his office had entered into a settlement agreement with EmblemHealth, Inc., requiring the health plan to cover anesthesiology services provided in connection with an in-network preventive colonoscopy, without any cost-sharing by the patient. The agreement includes a $25,000 penalty and applies not just prospectively but also requires Emblem to send nearly $400,000 of reimbursements to 255 patients who were inappropriately charged co-payments.
The Affordable Care Act (ACA) requires health plans to provide first-dollar coverage for colorectal cancer screening tests and certain other preventive care services, waiving any patient co-insurance, co-payments or deductible amounts. The Emblem agreement expressly extends the requirement to anesthesia for screening colonoscopies: “Because colonoscopies necessitate the administration of anesthesia, anesthesia services provided in connection with preventive colonoscopies should likewise be covered without member cost-sharing.”
In the final Physician Fee Schedule rule for 2015, the Centers for Medicare...