 By:
Serene K. Zeni, Esq. Clark Hill, PLC, Birmingham, MI
Greg Moore, Esq. Clark Hill, PLC, Birmingham, MI
Alexandra A. Hall, Esq. Clark Hill, PLC, Birmingham, MI
It is not by chance that the discussions leading to the SGR “fix,” the Medicare Access and CHIP Reauthorization Act of 2015 (H.R.2), signed into law on April 16, 2015, began with an anesthesiologist, Republican Congressman Andy Harris, MD. The manner in which the Sustainable Growth Rate (SGR) would be fixed was particularly relevant to anesthesiologists who get roughly 31 percent of commercial payment when they bill Medicare, according to Jane Fitch, MD, chair of anesthesiology at the University of Oklahoma Health Sciences Center in Oklahoma City, in an interview with Anesthesiology News. Understanding H.R.2, therefore, is necessary to understand how anesthesia practices will be reimbursed in the future.
To understand the rationale underlying H.R.2, it is necessary to start with the basic assumption...
By:
Serene K. Zeni, Esq. Clark Hill, PLC, Birmingham, MI
Greg Moore, Esq. Clark Hill, PLC, Birmingham, MI
Alexandra A. Hall, Esq. Clark Hill, PLC, Birmingham, MI
It is not by chance that the discussions leading to the SGR “fix,” the Medicare Access and CHIP Reauthorization Act of 2015 (H.R.2), signed into law on April 16, 2015, began with an anesthesiologist, Republican Congressman Andy Harris, MD. The manner in which the Sustainable Growth Rate (SGR) would be fixed was particularly relevant to anesthesiologists who get roughly 31 percent of commercial payment when they bill Medicare, according to Jane Fitch, MD, chair of anesthesiology at the University of Oklahoma Health Sciences Center in Oklahoma City, in an interview with Anesthesiology News. Understanding H.R.2, therefore, is necessary to understand how anesthesia practices will be reimbursed in the future.
To understand the rationale underlying H.R.2, it is necessary to start with the basic assumption...
One of the largest anesthesia groups in the Midwest has won an important victory in US ex rel Donegan v. Anesthesia Associates of Kansas City, 2015 WL 3616640 (W.D. Mo., June 9, 2015), a False Claims Act (FCA) lawsuit initiated by a whistleblower several years ago. On June 9, 2015, a federal district court in Missouri granted the defendant’s motion for summary judgment, effectively ending the case unless the plaintiff or “relator” files and wins an appeal.Donegan should be helpful to anyone defending against allegations that they billed the federal government improperly for medical services, in violation of the FCA, based on someone else’s interpretation of an ambiguous rule. In the court’s own words, “A relator ‘must show that there is no reasonable interpretation of the law that would make the allegedly false statement true.’”This the relator, John Donegan, a CRNA formerly employed by the defendant, Anesthesia Associates of Kansas City...
 Neda M. Ryan, Esq. Corporate Compliance Attorney, Anesthesia Business Consultants, Jackson, MI
Christopher J. Ryan, Esq. Giarmarco, Mullins & Horton, PC, Troy, MI
The number of self-pay patients continues to rise. The term “self-pay” used to apply primarily to the population of individuals who are uninsured; now, the term continues to expand to also represent the insured population with high deductible plans. Some in the community call self-pay “no pay” because collecting payment from these individuals can be extremely difficult. Unfortunately for healthcare providers, medical debts do not rise to the top of many consumers’ priority lists, especially if money is tight. They often fall behind items like mortgages, car payments and credit card bills. To address this situation there are two options: either eliminate self-pay patients from a practice altogether (which is not feasible for most anesthesiologists), or take the right steps early on to increase a practice’s likelihood of...
Neda M. Ryan, Esq. Corporate Compliance Attorney, Anesthesia Business Consultants, Jackson, MI
Christopher J. Ryan, Esq. Giarmarco, Mullins & Horton, PC, Troy, MI
The number of self-pay patients continues to rise. The term “self-pay” used to apply primarily to the population of individuals who are uninsured; now, the term continues to expand to also represent the insured population with high deductible plans. Some in the community call self-pay “no pay” because collecting payment from these individuals can be extremely difficult. Unfortunately for healthcare providers, medical debts do not rise to the top of many consumers’ priority lists, especially if money is tight. They often fall behind items like mortgages, car payments and credit card bills. To address this situation there are two options: either eliminate self-pay patients from a practice altogether (which is not feasible for most anesthesiologists), or take the right steps early on to increase a practice’s likelihood of...
On July 6, 2015, as we advised readers in our Alert of July 20th, the Centers for Medicare and Medicaid Services (CMS) and the American Medical Association (AMA) jointly announced efforts to help physicians prepare for the October 1st changeover to ICD-10 diagnosis coding. The joint announcement indicated that or a full year from October 1, 2015, Medicare review contractors will not deny physician claims “based solely on the specificity of the ICD-10 diagnosis code as long as the physician/practitioner used a valid code from the right family.” Confronted with many requests for a clarification of what constitutes “a valid code from the right family,” CMS issued a longer set of Frequently Asked Questions (FAQs) on July 27, and then revised those FAQs again on July 31. The short answer is that a “valid” code is one consisting of three to seven characters but “a three-character code is to be used...
 A review of recent activity by the Health and Human Services Office of Inspector General (OIG) indicates that it may be physicians’ turn for a higher level of scrutiny. Over the past few years, the OIG has released three Special Fraud Alerts focusing on physicians’ arrangements. In 2013, the OIG issued a fraud alert about physician-owned device distributorships, and in 2014 it issued a fraud alert about lab payments to physicians. The third alert, issued June 9, 2015, addresses physician compensation arrangements that may result in significant liability under the federal Anti-Kickback Statute (AKS).
One purpose of the AKS is to protect patients from inappropriate medical referrals or recommendations by healthcare professionals who may be unduly influenced by financial incentives. Section 1128B(b) of the Social Security Act (the Act) makes it a criminal offense to knowingly and willfully offer, pay, solicit or receive any remuneration to induce, or in return for,...
A review of recent activity by the Health and Human Services Office of Inspector General (OIG) indicates that it may be physicians’ turn for a higher level of scrutiny. Over the past few years, the OIG has released three Special Fraud Alerts focusing on physicians’ arrangements. In 2013, the OIG issued a fraud alert about physician-owned device distributorships, and in 2014 it issued a fraud alert about lab payments to physicians. The third alert, issued June 9, 2015, addresses physician compensation arrangements that may result in significant liability under the federal Anti-Kickback Statute (AKS).
One purpose of the AKS is to protect patients from inappropriate medical referrals or recommendations by healthcare professionals who may be unduly influenced by financial incentives. Section 1128B(b) of the Social Security Act (the Act) makes it a criminal offense to knowingly and willfully offer, pay, solicit or receive any remuneration to induce, or in return for,...
The value of healthcare acquisitions in the U.S. in the first seven months of 2015 is now more than $356 billion. The final figure for all of 2014 was $326.1 billion, according to the Wall Street Journal. Within anesthesiology alone, 14 different entities acquired 27 anesthesia practices in 2014 at an estimated total cost of nearly $1 billion. Almost as many acquisitions were completed in the first quarter of this year alone. (Anesthesiology Acquisition Rate Still at Fevered Pace, Anesthesiology News, July 2015).Merger and acquisition (M&A) activity in health care has spread far beyond the consolidation of groups and hospitals and health systems. We are now in a phase where health insurance companies are trying to grow by buying others. The potential for a landscape dominated by just a handful of insurance behemoths is raising concerns across the industry.Anthem, Inc. announced on July 24th that it had entered into a definitive...
Anesthesia Business Consultants (ABC), a leading provider in billing and practice management for the anesthesia and pain management specialty, is pleased to announce its latest partnership with Stat-App. Developed and piloted by Anaesthesia Associates of Massachusetts, the largest private anesthesia practice in New England, Stat-App focuses on improving the efficiencies of anesthesia practices to better serve the facilities they work in.The Stat-App infrastructure is designed to allow clinical providers to securely communicate with their colleagues, and to better understand who is available presently within their own facility utilizing GPS technologies. Leveraging devices that are already utilized today, the Stat-App brings a new capability to an anesthesia practice to better manage schedules, utilization and costs."The profitability, and even survival, of an independent multi-facility practice group depends upon correctly aligning valuable clinicians with an appropriate workload. Stat-App exists to optimize multi-facility practices, open lines of communication and to equalize provider workload," said Christopher...
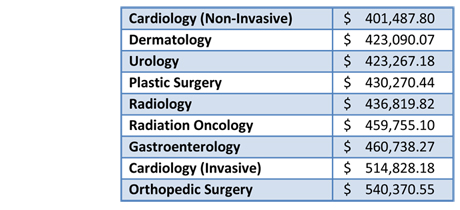 The amount of physician compensation is one of the key issues in every negotiation between anesthesiologists and anesthesiology groups and hospitals or health systems. What is the fair market value for an anesthesiologist? And how much do you have to offer to attract him or her? There is no definitive set of data, just a handful of surveys, some free and some for sale at hefty prices. Practices that are sufficiently large or that have a long history often realize that their own internal information may be the best available. In the interest of covering as many bases as possible and providing the greatest amount of data on which interested readers may perform their meta-analyses, we bring to your attention the latest public physician compensation information, released last week by Modern Healthcare in its Physician Compensation: 2015 report.
For 2015, Modern Healthcare reports an average salary for anesthesiologists of $384,290, which comes from...
The amount of physician compensation is one of the key issues in every negotiation between anesthesiologists and anesthesiology groups and hospitals or health systems. What is the fair market value for an anesthesiologist? And how much do you have to offer to attract him or her? There is no definitive set of data, just a handful of surveys, some free and some for sale at hefty prices. Practices that are sufficiently large or that have a long history often realize that their own internal information may be the best available. In the interest of covering as many bases as possible and providing the greatest amount of data on which interested readers may perform their meta-analyses, we bring to your attention the latest public physician compensation information, released last week by Modern Healthcare in its Physician Compensation: 2015 report.
For 2015, Modern Healthcare reports an average salary for anesthesiologists of $384,290, which comes from...
On July 6, 2015, the Centers for Medicare and Medicaid Services (CMS) and the American Medical Association (AMA) jointly announced efforts to help physicians prepare for the October 1st changeover to ICD-10 diagnosis coding. The AMA and CMS will be offering webinars, on-site training, articles and national conference calls to educate providers and ease the transition throughout the summer.This announcement makes it seem less likely than ever that there will be a delay in CMS’s implementation of ICD-10 coding. CMS’s new set of Frequently Asked Questions (FAQs) entitled “CMS and AMA Announce Efforts to Help Providers Get Ready for ICD-10” stated clearly and in boldface type “a valid ICD-10 code will be required on all claims starting on October 1.” (CMS, of course, does not have the discretion to put off the deadline, for which Congressional action would be required.) The AMA’s participation in the final set of educational programs and...
In order to engage fully with their hospital partners, anesthesiologists need to understand some of their institutions’ concerns. While our readers may not hold the solutions, familiarity with pressures on the hospitals can only help in negotiating the relationships, day-to-day and at contract renewal time. The Two-Midnight rule is a current hospital hassle of which anesthesiologists should have some awareness.Background Whether a patient is admitted as an inpatient or treated as an outpatient has a considerable impact on hospital payment and on patient cost sharing. Medicare covers inpatient admissions under Part A and pays $3,100 more on average for an inpatient stay than for an outpatient observation stay, which is paid under Part B, according to claims data reviewed by the Medicare Payment Advisory Commission (MedPAC).By 2012 the Medicare Recovery Audit Contractors (RACs) had become so aggressive in pursuing medically unnecessary hospital admissions that hospitals started keeping patients for extended outpatient...
Anesthesia Business Consultants (ABC) is pleased to announce Anesthesia Valet™, an exciting, new platform to support the quality reporting programs designed to enable the anesthesia specialty and as mandated by the Centers for Medicare and Medicaid Services (CMS).Anesthesia Valet is an easy, streamlined solution developed exclusively for the anesthesia specialty to document, analyze and submit quality data to the Anesthesia Quality Institute’s (AQI) Qualified Clinical Data Registry (QCDR) database. ABC has been a preferred vendor of the AQI since 2010; the AQI was founded by the American Society of Anesthesiologists (ASA) in 2008. The AQI established the National Anesthesia Clinical Outcomes Registry (NACOR) for the collection and reporting of anesthesia quality metrics.Starting in 2015, Eligible Professionals need to report quality data to a designated QCDR or potentially face reimbursement penalties from CMS. “NACOR not only meets CMS’ reporting requirements as a designated QCDR, but provides the anesthesia speciality a valuable resource...
“Don’t put anything in an e-mail message or on Facebook that you wouldn’t want to see on the front page of the New York Times.” We have all heard that warning many times. In the wake of a widely-reported malpractice and defamation judgment awarded by a Virginia jury to a patient whose anesthesiologist made unpleasant statements to colleagues during the patient’s colonoscopy, one wonders whether the warning should be updated to read: “Don’t say or write anything negative about anyone, anywhere, or you may be sued.”This case was noteworthy not merely for the contempt with which the doctor talked about her patient, but also for the fact that the conversation in the procedure room was recorded by the patient’s smartphone, which neither he nor the medical team realized had been left on. The patient claimed he had inadvertently left his phone in the room, set to record, having neglected to turn...
“Don’t put anything in an e-mail message or on Facebook that you wouldn’t want to see on the front page of the New York Times.” We have all heard that warning many times. In the wake of a widely-reported malpractice and defamation judgment awarded by a Virginia jury to a patient whose anesthesiologist made unpleasant statements to colleagues during the patient’s colonoscopy, one wonders whether the warning should be updated to read: “Don’t say or write anything negative about anyone, anywhere, or you may be sued.”This case was noteworthy not merely for the contempt with which the doctor talked about her patient, but also for the fact that the conversation in the procedure room was recorded by the patient’s smartphone, which neither he nor the medical team realized had been left on. The patient claimed he had inadvertently left his phone in the room, set to record, having neglected to turn...
 The specialty of anesthesiology, and indeed all of health care, is somewhere in the middle of its long transition away from a volume-driven cottage industry. Details of the destination are not yet clear, but one change of which we can be confident is the shift away from in-hospital care toward outpatient settings. Nearly two-thirds of procedures are now performed on an ambulatory basis. With the advent of more and more minimally invasive techniques— not to mention ever-safer anesthesia—that proportion will continue to grow.
Stanford Plavin, MD gives us a window into the mindset necessary for anesthesiologists to succeed in the ambulatory surgical center (ASC) environment, where “the microscope is powerful and the lights are bright” and where even the identity of our customers is changing. “What do the ASC’s customers want?” he asks in Anesthesiologists and the World of ASCs: A Different Value Proposition. Dr. Plavin recommends surveys to identify their...
The specialty of anesthesiology, and indeed all of health care, is somewhere in the middle of its long transition away from a volume-driven cottage industry. Details of the destination are not yet clear, but one change of which we can be confident is the shift away from in-hospital care toward outpatient settings. Nearly two-thirds of procedures are now performed on an ambulatory basis. With the advent of more and more minimally invasive techniques— not to mention ever-safer anesthesia—that proportion will continue to grow.
Stanford Plavin, MD gives us a window into the mindset necessary for anesthesiologists to succeed in the ambulatory surgical center (ASC) environment, where “the microscope is powerful and the lights are bright” and where even the identity of our customers is changing. “What do the ASC’s customers want?” he asks in Anesthesiologists and the World of ASCs: A Different Value Proposition. Dr. Plavin recommends surveys to identify their...
The United States Supreme Court has again upheld the Affordable Care Act (ACA). The Court announced its decision in a 6-3 ruling in King v. Burwell on Thursday, June 25, 2015.Some 6.4 million Americans were at risk of losing their “Obamacare” health insurance coverage had the Court invalidated the ACA and eliminated the subsidies that made the insurance affordable. The cost of insurance was predicted to rise dramatically for millions of others as the pool of participants in the individual markets shrank.Six words provided the basis for the challenge brought by four individual plaintiffs in Virginia: “an Exchange established by the State.” The statute provides for a premium tax credit (i.e., a subsidy) for “health plans offered in the individual market within a State which cover the taxpayer, the taxpayer’s spouse, or any dependent (as defined in section 152) of the taxpayer and which were enrolled in through an Exchange established...
Anesthesia Business Consultants (ABC), is pleased to announce its latest partnership with Virginia Commonwealth University, (VCU) Department of Anesthesiology to provide integrated practice management billing services.ABC entered into discussions with VCU to explore options to integrate VCU’s billing information into ABC’s proprietary practice management software, F1RSTAnesthesia. Effective September 1, 2015, ABC will begin receiving charge information from VCU. This data will be processed via F1RSTAnesthesia with its very sophisticated concurrency and reporting modules and returned to VCU’s GE-IDX system through a secure HL7 interface. The data will then be finalized via VCU’s GE-IDX system, allowing VCU to bill claims out of their historical system, maintaining the look and feel of an internal process.ABC is very excited to be working with VCU on this exciting, new project. We see the integration of F1RSTAnesthesia into VCU's billing process as an excellent way to allow them to provide the level of service they are...
Last week’s Alert brought a new Fraud Alert from the Office of the Inspector General (OIG) to readers’ attention. The OIG is on the lookout for arrangements in which physicians receive compensation for medical director services that are intended to induce referrals of patients. We wish the OIG were equally interested in the anti-kickback statute ramifications of the “company model,” in which anesthesiologists are asked to share their clinical revenues and thus compensate other physicians and/or facilities for referrals.
We last wrote about company model-like behavior in our Alert dated November 18, 2013 (The OIG Rejects Another Attempt to Take a Franchise Fee from Anesthesiologists), and some of our readers have asked us to address the issue again.
Third parties have continued to seek to enter into company model arrangements. In February 2014, the American Society of Anesthesiologists (ASA) renewed its request that the OIG amend several of the anti-kickback statute safe...
 In today’s anesthesiology environment, all groups are trying to size up their best option to survive and thrive into the future. Some try to go it alone and others sell out to practice management firms, while others seek or are forced into hospital employment.
Another option that many groups are considering is merging with other anesthesiology groups.
Why are anesthesiology groups considering mergers? Mergers:
Allow them to maintain a higher level of autonomy than any other option,
Prevent the groups from being played off against each other by hospitals or managed care companies,
Build clout,
Create the ability to hire needed management expertise, and
Allow them to move towards economies of scale.
In addition, today’s healthcare environment is influencing many hospitals to merge or join systems. When hospitals integrate they often want to work with a single anesthesiology group to cover all their facilities. When this happens, many anesthesiology groups consider...
In today’s anesthesiology environment, all groups are trying to size up their best option to survive and thrive into the future. Some try to go it alone and others sell out to practice management firms, while others seek or are forced into hospital employment.
Another option that many groups are considering is merging with other anesthesiology groups.
Why are anesthesiology groups considering mergers? Mergers:
Allow them to maintain a higher level of autonomy than any other option,
Prevent the groups from being played off against each other by hospitals or managed care companies,
Build clout,
Create the ability to hire needed management expertise, and
Allow them to move towards economies of scale.
In addition, today’s healthcare environment is influencing many hospitals to merge or join systems. When hospitals integrate they often want to work with a single anesthesiology group to cover all their facilities. When this happens, many anesthesiology groups consider...
Note: ABC encourages all anesthesiology groups to participate in ASA’s 13th survey of commercial payment rates, launched on June 9th. The results will be published in the ASA Newsletter later this year and obviously they will be more meaningful if there are many responses. For further information go to http://www.asahq.org/advocacy/fda-and-washington-alerts/washington-alerts/2015/06/please-participate-in-2015-survey-of-commercial-payment-rates.
Many anesthesiologists serve as the paid medical director of their operating room suite or ambulatory surgical center (ASC). Many others would like to receive compensation for medical director services. The Health and Human Services Office of the Inspector General (OIG) has just issued a Fraud Alert entitled Physician Compensation Arrangements May Result in Significant Liability, of which they should all be aware.
The Anti-Kickback Statute
As the OIG has stated in numerous Advisory Opinions,
The anti-kickback statute makes it a criminal offense knowingly and willfully to offer, pay, solicit, or receive any remuneration to induce or reward referrals of items or...
 What is your succession plan? Oh, you don’t have one! Why not? Maybe you don’t think you need one. Or maybe you figure you will manage a change in leadership the way you manage anesthesia in the Operating Room; when the need arises you will figure it out. If this describes your practice you are not alone. If so, it may be time to think about what this says about your practice.
The Significance of a Strong Leader
The reality of most private practice anesthesia groups is that the strength of the contract with the hospital or facility depends heavily on the relationship between a key member of the practice and the administration. This can be a good thing when the leader speaks for the interests of the membership but what happens when he or she steps down? It is an unknown, but this is an inevitable development for every practice....
What is your succession plan? Oh, you don’t have one! Why not? Maybe you don’t think you need one. Or maybe you figure you will manage a change in leadership the way you manage anesthesia in the Operating Room; when the need arises you will figure it out. If this describes your practice you are not alone. If so, it may be time to think about what this says about your practice.
The Significance of a Strong Leader
The reality of most private practice anesthesia groups is that the strength of the contract with the hospital or facility depends heavily on the relationship between a key member of the practice and the administration. This can be a good thing when the leader speaks for the interests of the membership but what happens when he or she steps down? It is an unknown, but this is an inevitable development for every practice....