 We have known since Congress passed the Medicare Access and CHIP Reauthorization Act (MACRA), just over a year ago, that big changes in the way that CMS pays physicians are coming. MACRA has already repealed the detested Sustainable Growth Rate formula. On Wednesday, April 27, CMS released the proposed regulations (Medicare Program; Merit-Based Incentive Payment System (MIPS) and Alternative Payment Model (APM) Incentive under the Physician Fee Schedule, and Criteria for Physician-Focused Payment Models) that begin to define the new unified framework called the Quality Payment Program going forward.
The 962-page proposed rule is just that: proposed. CMS will be receiving public comments through June 27 and will then consider them for several months before publishing the final rule later this year. We hope that the final will be released sooner rather than later, because anesthesiologists and other physicians will need to know what they must do before January 1, 2017....
We have known since Congress passed the Medicare Access and CHIP Reauthorization Act (MACRA), just over a year ago, that big changes in the way that CMS pays physicians are coming. MACRA has already repealed the detested Sustainable Growth Rate formula. On Wednesday, April 27, CMS released the proposed regulations (Medicare Program; Merit-Based Incentive Payment System (MIPS) and Alternative Payment Model (APM) Incentive under the Physician Fee Schedule, and Criteria for Physician-Focused Payment Models) that begin to define the new unified framework called the Quality Payment Program going forward.
The 962-page proposed rule is just that: proposed. CMS will be receiving public comments through June 27 and will then consider them for several months before publishing the final rule later this year. We hope that the final will be released sooner rather than later, because anesthesiologists and other physicians will need to know what they must do before January 1, 2017....
Anesthesia Business Consultants (ABC), a leading provider in billing and practice management for anesthesia and pain management specialty, is pleased to announce they will be serving as Diamond Sponsor, as well as attending the Medical Group Management Association’s 2016 Anesthesia Conference, being held this weekend, May 5 – 7, 2016, at Gaylord National Resort & Convention Center, National Harbor, MD. Whether you are new to anesthesiology/pain management or an experienced administrator, the MGMA 2016 Anesthesia Conference will provide practical education that will include peer-to-peer interaction, tools and techniques and in-depth learning experiences designed to help you and your practice succeed.ABC will be premiering the availability of its Qualified Clinical Data Registry (QCDR) program. The QCDR is the next stage of the government’s transition to value-based payments. ABC's new QCDR program demonstrates our strong commitment to clients, the industry and compliance with these governmental quality programs.Payment models are getting even more complex...
On July 13, 2015, we informed you of CMS’s Two-Midnight Rule. After much pushback from industry stakeholders and from the judicial system since our alert, CMS proposes to eliminate the notorious payment reduction under the Two-Midnight Rule in its FY 2017 Medicare Inpatient Prospective Payment System (IPPS) Proposed Rule (Proposed Rule). Though not slated to be finalized until the latter part of 2016, hospitals and their partners can be optimistic that the penalty under the Two-Midnight Rule may soon be a memory.
The Two-Midnight Rule, effective beginning October 1, 2013, was enacted with the intent of curbing payment for inpatient hospital admissions (i.e., Part A). The Two-Midnight Rule generally states that payment under Medicare Part A is appropriate if the admitting physician has a reasonable expectation that the patient’s stay would span at least two midnights. For patients expected to stay less than two midnights, payment under Medicare Part B (i.e.,...
Correlation does not equal causation.
One fresh demonstration of the truth of this axiom appears in an article in this month’s issue of Gastroenterology (Wernli KJ, Brenner AT, Rutter CM, Inadomi JM. Risks Associated With Anesthesia Services During Colonoscopy. Gastroenterology 2016; 150: 888-894).
The research team, from the Group Health Research Institute in Seattle, performed a prospective cohort study of nationwide claims data from 3,168,228 colonoscopy procedures in adults aged 40 to 64 in the Truven Health MarketScan Research Databases from 2008 to 2011. Moderate sedation was performed in 65.6 percent of the procedures included in the study; deep sedation (in most cases using propofol) was provided by anesthesiologists or nurse anesthetists in 34.4 percent. The study authors found a correlation between use of anesthesia services and a 13 percent higher risk of any complication within 30 days: specifically, higher risk of perforation, bleeding, abdominal pain, complications due to anesthesia, and...
 How would you like to know exactly what’s going to happen in the future so that you can prepare for and profit from it?
I have a crystal ball. Here, let me share it with you.
We’re going to review some of the trends currently impacting, and soon to impact, hospitals that will, I predict, lead to their destruction, at least as we know them.
There is absolutely no question that these trends are going to have an impact on your anesthesia practice. Start preparing now.
Trend 1: Hospitals Are Getting Bigger and That is a Weakness
Government induces physician labor
Obamacare favors the growth of hospitals with its incentives for aligning physicians. Think Accountable Care Organizations (ACOs) and other incentives to coordinate care, meaning coordination via hospitals.
Although reports lag by several years, at least 20 percent to 30 percent of all practicing physicians are currently employed by hospitals. There...
How would you like to know exactly what’s going to happen in the future so that you can prepare for and profit from it?
I have a crystal ball. Here, let me share it with you.
We’re going to review some of the trends currently impacting, and soon to impact, hospitals that will, I predict, lead to their destruction, at least as we know them.
There is absolutely no question that these trends are going to have an impact on your anesthesia practice. Start preparing now.
Trend 1: Hospitals Are Getting Bigger and That is a Weakness
Government induces physician labor
Obamacare favors the growth of hospitals with its incentives for aligning physicians. Think Accountable Care Organizations (ACOs) and other incentives to coordinate care, meaning coordination via hospitals.
Although reports lag by several years, at least 20 percent to 30 percent of all practicing physicians are currently employed by hospitals. There...
Many pain medicine procedures, and, increasingly, perioperative and critical care procedures such as central venous access are performed using ultrasound guidance (U/S). Indeed, U/S is an integral part of many CPT® codes, e.g., 20604 [Arthrocentesis, aspiration and/or injection, small joint or bursa, (e.g., fingers, toes), with ultrasound guidance, with permanent recording and reporting]. When and where, and by whom, must those permanent images be stored? What if another entity, such as a hospital, is responsible for storing them? According to Sonosite,
All diagnostic ultrasound examinations, including those when ultrasound is used to guide a procedure, require that permanently recorded images be maintained in the patient record. The images can be kept in the patient record or some other archive--they do not need to be submitted with the claim. Images can be stored as printed images, on a tape or electronic medium. Documentation of the study must be available to the insurer...
 One important voice sounding a warning or at least a heads-up about what is coming is that of Mark Weiss, Esq. The title of Mr. Weiss’s article— Impending Death of Hospitals: Will Your Anesthesia Practice Survive?—which is also the title of his forthcoming book—is intentionally provocative. He lays out several of the major threats confronting hospitals, starting with health system growth, through mergers and acquisitions, acquisition of physician practices and investments in integrated delivery networks. Others have predicted that the Federal Trade Commission will place a damper on hospital merger activity in 2016, but the quest for greater scale and scope is going to continue. Anesthesiologists may want to consider the wisdom of relying on the ongoing health of just one or two hospitals. This is especially true in light of the ability of physician-owned facilities, notably ambulatory surgery centers, and new technologies (think telemedicine) to disrupt hospitals’ traditional business. Mr....
One important voice sounding a warning or at least a heads-up about what is coming is that of Mark Weiss, Esq. The title of Mr. Weiss’s article— Impending Death of Hospitals: Will Your Anesthesia Practice Survive?—which is also the title of his forthcoming book—is intentionally provocative. He lays out several of the major threats confronting hospitals, starting with health system growth, through mergers and acquisitions, acquisition of physician practices and investments in integrated delivery networks. Others have predicted that the Federal Trade Commission will place a damper on hospital merger activity in 2016, but the quest for greater scale and scope is going to continue. Anesthesiologists may want to consider the wisdom of relying on the ongoing health of just one or two hospitals. This is especially true in light of the ability of physician-owned facilities, notably ambulatory surgery centers, and new technologies (think telemedicine) to disrupt hospitals’ traditional business. Mr....  If you receive a letter by email that begins like this:
You should respond within the 14 days mentioned in the letter. Congratulations; you are participating in Phase 2 of the HIPAA Audit Program.
With this letter, OCR is seeking just to identify contacts to create a pool of HIPAA-covered entities (CEs) and their business associates (BAs) for possible audits. In the next step, OCR will transmit a pre-audit questionnaire to gather data about the size, type, and operations of CEs and their BAs. These data will then be used with other information to create potential audit subject pools. Eventually more than 200 entities will face audits in Phase 2 of the HIPAA Audit Program, which will primarily be desk audits, although some on-site audits will also be conducted.
Phase 1 of the HIPAA Audits
HIPAA established national standards for the privacy and security of protected...
If you receive a letter by email that begins like this:
You should respond within the 14 days mentioned in the letter. Congratulations; you are participating in Phase 2 of the HIPAA Audit Program.
With this letter, OCR is seeking just to identify contacts to create a pool of HIPAA-covered entities (CEs) and their business associates (BAs) for possible audits. In the next step, OCR will transmit a pre-audit questionnaire to gather data about the size, type, and operations of CEs and their BAs. These data will then be used with other information to create potential audit subject pools. Eventually more than 200 entities will face audits in Phase 2 of the HIPAA Audit Program, which will primarily be desk audits, although some on-site audits will also be conducted.
Phase 1 of the HIPAA Audits
HIPAA established national standards for the privacy and security of protected...
The anesthesia record, like medical records in general, should be complete and accurate at the time when the physician signs it—ideally. In practice, it occasionally requires amendment. Given the huge role that accurate documentation plays in our medical payment system, compliance with the rules and regulations governing medical record amendments is important. Altered medical records have great potential for fraud, especially if the added information helps to raise the level of a billable service, and no one should be surprised if auditors look at any changes closely.
One basic principle was added to the first paragraph of the provision that regulates amendments in Chapter 3 of the Medicare Program Integrity Manual, Section 3.3.2.5, when that provision was updated effective October 2, 2015. The intent of the new paragraph is to make it clear that amendment should be the exception.
All services provided to beneficiaries are expected to be documented in the...
 “CMS’ pay-for-performance reimbursement changes are looming. As members of the Huntington Accountable Care Organization (ACO), anesthesia recognizes the need to improve surgical outcomes. Our collective financial future is tied to solid quality improvements that only increasingly coordinated care can deliver. We will double down on our cooperative effort with our hospital in order to improve medical outcomes, to lower costs and to improve the patient experience.” – Pacific Valley Medical Group, Pasadena, CA.
Summary of Recent Events
The Centers for Medicare & Medicaid Services (CMS) is pushing quality, the American Society of Anesthesiologists (ASA) is pushing the perioperative surgical home (PSH) and our 30-partner Pacific Valley Medical (anesthesiology) Group (PVMG) in Pasadena, CA is picking up both causes. In our commitment to a PSH clinic staffed and managed by anesthesiologists, we are fully embracing the concept of transitional care & perioperative medicine. This is our contribution to our patients and to...
“CMS’ pay-for-performance reimbursement changes are looming. As members of the Huntington Accountable Care Organization (ACO), anesthesia recognizes the need to improve surgical outcomes. Our collective financial future is tied to solid quality improvements that only increasingly coordinated care can deliver. We will double down on our cooperative effort with our hospital in order to improve medical outcomes, to lower costs and to improve the patient experience.” – Pacific Valley Medical Group, Pasadena, CA.
Summary of Recent Events
The Centers for Medicare & Medicaid Services (CMS) is pushing quality, the American Society of Anesthesiologists (ASA) is pushing the perioperative surgical home (PSH) and our 30-partner Pacific Valley Medical (anesthesiology) Group (PVMG) in Pasadena, CA is picking up both causes. In our commitment to a PSH clinic staffed and managed by anesthesiologists, we are fully embracing the concept of transitional care & perioperative medicine. This is our contribution to our patients and to...
Recent media coverage of surgeons operating in two concurrent cases raises three issues: (1) patient safety, (2) compliance with the Medicare teaching physician billing rules and (3) transparency vis-à-vis patients.
The Safety Controversy
The question whether it is right or safe for surgeons to run two operations at once erupted publicly last year when the Boston Globe published a detailed report (Clash in the Name of Care) focusing on events that had occurred at Massachusetts General Hospital (MGH) in August 2012. A 41-year old patient had undergone complicated spinal surgery from which he emerged a quadriplegic, and it revealed itself that his surgeon had been in and out of the operating room, attending to a patient undergoing spinal fusion in another OR for seven of the eleven hours that the first case took to complete.
A controversy among MGH surgeons and anesthesiologists over concurrent surgeries had been years in the making. ...
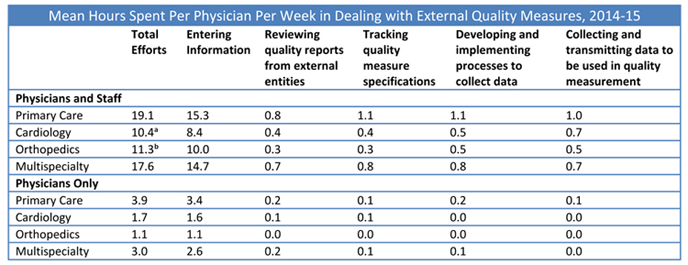 Donald Berwick, MD, senior fellow at the Institute for Healthcare Improvement (IHI) (and a former CMS administrator) described nine steps to advance healthcare into “the moral era” at an IHI forum in December, 2015. One of those steps was to “stop excessive measurement.” Dr. Berwick said:
I don’t mean that we should stop measuring. Indeed, I celebrate transparency in every form. How else can you learn? But we need to tame measurement. It has gone crazy. Far from showing us our way, these searchlights training on us, they blind us. ... I vote for a 50 percent reduction in all metrics currently being used.
Many anesthesiologists and pain physicians will agree that quality measurement has gone over the edge. The ASA’s Anesthesia Quality Institute (AQI) has adopted 22 measures and has identified 26 official Physician Quality Reporting System (PQRS) measures that can be reported by anesthesiologists and/or pain physicians. In proposing 48...
Donald Berwick, MD, senior fellow at the Institute for Healthcare Improvement (IHI) (and a former CMS administrator) described nine steps to advance healthcare into “the moral era” at an IHI forum in December, 2015. One of those steps was to “stop excessive measurement.” Dr. Berwick said:
I don’t mean that we should stop measuring. Indeed, I celebrate transparency in every form. How else can you learn? But we need to tame measurement. It has gone crazy. Far from showing us our way, these searchlights training on us, they blind us. ... I vote for a 50 percent reduction in all metrics currently being used.
Many anesthesiologists and pain physicians will agree that quality measurement has gone over the edge. The ASA’s Anesthesia Quality Institute (AQI) has adopted 22 measures and has identified 26 official Physician Quality Reporting System (PQRS) measures that can be reported by anesthesiologists and/or pain physicians. In proposing 48...  When you received your 2016 Current Procedural Terminology (CPT) and American Society of Anesthesiologists (ASA) Relative Value Guide (RVG) books or discs, you probably noticed there were no new anesthesia code additions or deletions listed for this year. Since the CPT book usually arrives before the RVG, you may not have taken a good look through your RVG or may not have ordered a 2016 RVG as there were no coding changes. However, there are a number of important updates in the RVG New/ Revised RVG Coding Comments section which are not included in the Anesthesia section of the CPT. These comments may affect the way anesthesia coders assign procedure codes in the upcoming year. As this article will not include all updated comments, be sure to order your 2016 RVG. I’ve chosen a few that are certain to have an impact on 2016 coding for anesthesia services.
Let’s start with...
When you received your 2016 Current Procedural Terminology (CPT) and American Society of Anesthesiologists (ASA) Relative Value Guide (RVG) books or discs, you probably noticed there were no new anesthesia code additions or deletions listed for this year. Since the CPT book usually arrives before the RVG, you may not have taken a good look through your RVG or may not have ordered a 2016 RVG as there were no coding changes. However, there are a number of important updates in the RVG New/ Revised RVG Coding Comments section which are not included in the Anesthesia section of the CPT. These comments may affect the way anesthesia coders assign procedure codes in the upcoming year. As this article will not include all updated comments, be sure to order your 2016 RVG. I’ve chosen a few that are certain to have an impact on 2016 coding for anesthesia services.
Let’s start with...
The American Pain Society (APS) last month released its first-ever Clinical Practice Guidelines on the Management of Postoperative Pain. The American Society of Anesthesiologists, which published its own Practice Guidelines for Acute Pain Management in the Perioperative Setting in Anesthesiology in 2012, provided input, and the American Society for Regional Anesthesia endorsed the APS Guidelines.
"The intent of the guideline is to provide evidence-based recommendations for better management of postoperative pain, and the target audience is all clinicians who manage pain resulting from surgery," said principal author Roger Chou, MD of the Departments of Medicine and Medical Informatics and Clinical Epidemiology, Oregon Health and Science University, Pacific Northwest Evidence Based Practice Center. (APS News Release, February 17, 2016.) Studies have shown again and again that the majority of surgical patients receive inadequate pain control, which can increase the risks of persistent postoperative pain and of post-surgical complications, function and functional recovery,...
 We all know that the healthcare industry is experiencing a wave of integration. This trend has been evident for many years. Fewer physicians are willing to assume the legal, financial and other business risks associated with owning their own practices. More and more physicians, including anesthesiologists, are becoming employed by large physician groups, health systems and national providers.
This shift necessarily involves not only entry into new employment arrangements but also the termination of existing relationships. And those terminations are often governed by written employment agreements, state and federal healthcare laws and employer benefit plans and other policies and procedures.
Before pursuing their next opportunity, physicians should pause for a moment and first attend to the arrangement that they are leaving. Departing physicians need to understand their legal rights and obligations when leaving their current employment relationships in order to avoid unintended consequences and detrimental missteps along the way. Here are...
We all know that the healthcare industry is experiencing a wave of integration. This trend has been evident for many years. Fewer physicians are willing to assume the legal, financial and other business risks associated with owning their own practices. More and more physicians, including anesthesiologists, are becoming employed by large physician groups, health systems and national providers.
This shift necessarily involves not only entry into new employment arrangements but also the termination of existing relationships. And those terminations are often governed by written employment agreements, state and federal healthcare laws and employer benefit plans and other policies and procedures.
Before pursuing their next opportunity, physicians should pause for a moment and first attend to the arrangement that they are leaving. Departing physicians need to understand their legal rights and obligations when leaving their current employment relationships in order to avoid unintended consequences and detrimental missteps along the way. Here are...
“Ransomware” attacks are malicious intrusions into information systems that encrypt the victim’s sensitive data and demand payment in exchange for a key to unlock the data. They have become increasingly common in the last few years. Since January 2013, there have been at least 100,000 cases of recorded ransomware attacks.
The installation of such malware on third parties’ computer systems is usually paired with a demand for payment by a certain deadline or the computer data will be deleted. This is a more direct means for criminals to realize profits from hacking into hospital systems than selling medical records. It is also a more immediate, direct threat to patient welfare.
On February 5, 2016, Hollywood Presbyterian Medical Center in Los Angeles became one of the latest and highest-profile victims, demonstrating that “ransomware should be a permanent concern for anyone or any business using the internet, and it’s going to get worse...
 Depending on one’s standpoint and experience, the peer review process can bring about mixed feelings in healthcare providers. Opinions about the effectiveness of the process, those who sit on the panel and the outcome are often debated. However, what is often less debated until long after the process has taken place is whether the information reviewed during the peer review process is subject to discovery in other settings.
Generally, the peer review process is a retrospective review of an event or series of events conducted in an effort to improve quality of care. In order to encourage candid review, many states have enacted laws to limit the discoverability of the proceedings, the records reviewed and the records created during the peer review process. In other words, in a civil proceeding, the contents of the peer review meetings and the records discussed are not discoverable and are not subject to a subpoena...
Depending on one’s standpoint and experience, the peer review process can bring about mixed feelings in healthcare providers. Opinions about the effectiveness of the process, those who sit on the panel and the outcome are often debated. However, what is often less debated until long after the process has taken place is whether the information reviewed during the peer review process is subject to discovery in other settings.
Generally, the peer review process is a retrospective review of an event or series of events conducted in an effort to improve quality of care. In order to encourage candid review, many states have enacted laws to limit the discoverability of the proceedings, the records reviewed and the records created during the peer review process. In other words, in a civil proceeding, the contents of the peer review meetings and the records discussed are not discoverable and are not subject to a subpoena...
The Affordable Care Act requires Medicare physicians and others to report and return overpayments within 60 days after the date when an overpayment is identified. Four years after publishing its proposed rule, CMS issued a Final Rule on February 6, 2016 with the intent of providing “needed clarity and consistency for providers and suppliers on the actions they need to take to comply with requirements for reporting and returning of self-identified overpayments.”
Identification of an overpayment starts the clock for the repayment deadline of 60 days. The most significant point of clarification in the Rule is that “identification” of an overpayment occurs when “the person has, or should have through the exercise of reasonable diligence, determined that the person has received an overpayment and quantified the amount of the overpayment." Applying this principle may seem to require little explanation but CMS managed to spend nine pages discussing it in the Federal...
 The past several years have, once again, brought major changes to the anesthesia community and have greatly impacted private practice anesthesia. Whereas the early nineties were a time of “anesthesia surplus” when anesthesiologists struggled to find opportunities paying as little as $100,000, those days were followed by a shortage of anesthesia providers. Supply and demand economics dictated that during the days of anesthesia staffing shortage, prices and compensation for anesthesia staff increased to the highest levels in history. Now, a new day is on the horizon where hospitals have many choices for anesthesia coverage. Smaller, private practice anesthesia groups struggle to sustain financial viability. Many groups are exploring mergers to achieve economies of scale and hoped-for negotiation leverage with private payers. Larger and mega-groups continue to liquidate their value and sell to publicly traded companies such as EmCare or MedNax. A growing number of large anesthesia staffing companies continue to enter...
The past several years have, once again, brought major changes to the anesthesia community and have greatly impacted private practice anesthesia. Whereas the early nineties were a time of “anesthesia surplus” when anesthesiologists struggled to find opportunities paying as little as $100,000, those days were followed by a shortage of anesthesia providers. Supply and demand economics dictated that during the days of anesthesia staffing shortage, prices and compensation for anesthesia staff increased to the highest levels in history. Now, a new day is on the horizon where hospitals have many choices for anesthesia coverage. Smaller, private practice anesthesia groups struggle to sustain financial viability. Many groups are exploring mergers to achieve economies of scale and hoped-for negotiation leverage with private payers. Larger and mega-groups continue to liquidate their value and sell to publicly traded companies such as EmCare or MedNax. A growing number of large anesthesia staffing companies continue to enter... 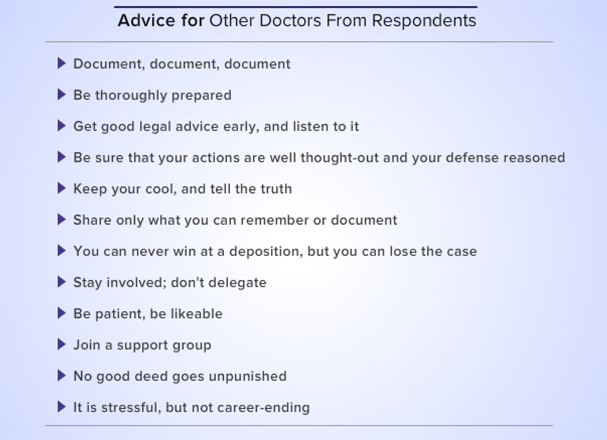 Being sued by a patient who had a poor outcome is one of the more unpleasant experiences most doctors can contemplate. The impact of a malpractice lawsuit can be potentially devastating to one’s financial, professional and personal well-being. But it is not often that bad. In a survey conducted by Medscape among 4,000 physicians (Peckham C. Medscape Malpractice Report 2015: Top Reasons Doctors Get Sued—Anesthesiologists. January 22, 2016), the responding anesthesiologists reported that trial resulted in a verdict for the plaintiff in only two percent of cases. Another 33 percent were dismissed either by the court or by the plaintiff. Twenty-four percent were dismissed from the suit either before any depositions were taken or within the first few months. Forty-one percent settled before reaching the verdict stage, and 10 percent resulted in a verdict in the anesthesiologist’s favor.
Malpractice litigation usually ends in the anesthesiologist’s favor or with a settlement that is...
Being sued by a patient who had a poor outcome is one of the more unpleasant experiences most doctors can contemplate. The impact of a malpractice lawsuit can be potentially devastating to one’s financial, professional and personal well-being. But it is not often that bad. In a survey conducted by Medscape among 4,000 physicians (Peckham C. Medscape Malpractice Report 2015: Top Reasons Doctors Get Sued—Anesthesiologists. January 22, 2016), the responding anesthesiologists reported that trial resulted in a verdict for the plaintiff in only two percent of cases. Another 33 percent were dismissed either by the court or by the plaintiff. Twenty-four percent were dismissed from the suit either before any depositions were taken or within the first few months. Forty-one percent settled before reaching the verdict stage, and 10 percent resulted in a verdict in the anesthesiologist’s favor.
Malpractice litigation usually ends in the anesthesiologist’s favor or with a settlement that is...