Although the editor, bless her heart, steadfastly refused to let me have a sneak, pre-publication peek at the other articles that appear alongside this one, my educated guess is that each of them purports to give you answers.I know that's why you usually read Communiqué. In fact, nearly every one of the hundreds of other articles that I've written ...
1637 Hits
Will Latham, MBA President, Latham Consulting Group, Inc., Chattanooga, TNIn despair at the way its programs were organized, the business school at one university recruited as the director of programs a successful businessman, who had made a modest fortune in his own business and wanted to move on to a new career. "I will soon put some order in thi...
1817 Hits
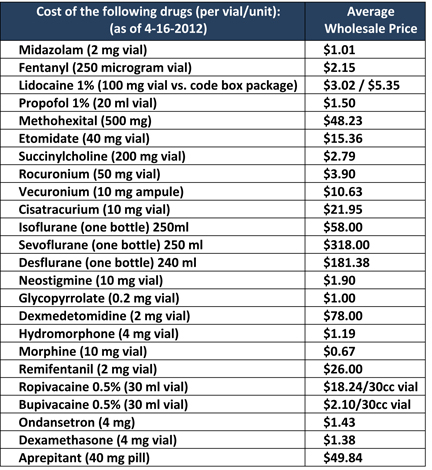 One way in which anesthesiologists can add value to their hospitals’ bottom line is by assuming responsibility for the cost of the drugs they order and administer.
The U.S. general anesthesia market size was approximately $2 billion in 2011 and is expected to grow at a moderate rate of 4% annually from 2011 to 2015, according to a Markets and Markets report. In addition, intravenous anesthetic drugs accounted for the largest share—65%—of the U.S. general anesthetics drugs market in 2011. Individual anesthesiology practitioners and groups have little control over total spending on drugs, just as they have little control over annual national spending on anesthesia services, but they can involve themselves in cost management locally, within their own institutions. As with most activities, success starts with knowledge.
First, anesthesiologists should be aware of the large variation in the cost of anesthetic agents and other medications used during the perioperative process. One...
One way in which anesthesiologists can add value to their hospitals’ bottom line is by assuming responsibility for the cost of the drugs they order and administer.
The U.S. general anesthesia market size was approximately $2 billion in 2011 and is expected to grow at a moderate rate of 4% annually from 2011 to 2015, according to a Markets and Markets report. In addition, intravenous anesthetic drugs accounted for the largest share—65%—of the U.S. general anesthetics drugs market in 2011. Individual anesthesiology practitioners and groups have little control over total spending on drugs, just as they have little control over annual national spending on anesthesia services, but they can involve themselves in cost management locally, within their own institutions. As with most activities, success starts with knowledge.
First, anesthesiologists should be aware of the large variation in the cost of anesthetic agents and other medications used during the perioperative process. One...
23005 Hits
 The specialty of anesthesiology is experiencing an unprecedented level of merger activity and practice acquisitions. The idea of two or more practices joining forces to secure their market position or enhance their strategic options is hardly a new phenomenon. The past few decades has seen the emergence of some very large anesthesia organizations that have dramatically changed the landscape in their respective markets. Once a pioneer in large group practice management, the Anesthesia Service Management Group (ASMG) and its 150 plus physicians in San Diego has become a model to emulate and refine. By some accounts, we have already reached a point where fewer than 100 organizations employ more than 15 percent of all anesthesia providers, but this is only a rough calculation, made especially challenging by the recent infusion of venture capital money that is inspiring an impressive list of practice acquisitions across the country. This dramatic rethinking of...
The specialty of anesthesiology is experiencing an unprecedented level of merger activity and practice acquisitions. The idea of two or more practices joining forces to secure their market position or enhance their strategic options is hardly a new phenomenon. The past few decades has seen the emergence of some very large anesthesia organizations that have dramatically changed the landscape in their respective markets. Once a pioneer in large group practice management, the Anesthesia Service Management Group (ASMG) and its 150 plus physicians in San Diego has become a model to emulate and refine. By some accounts, we have already reached a point where fewer than 100 organizations employ more than 15 percent of all anesthesia providers, but this is only a rough calculation, made especially challenging by the recent infusion of venture capital money that is inspiring an impressive list of practice acquisitions across the country. This dramatic rethinking of...
3394 Hits
 Anesthesiologists
increasingly point to their role in driving down the rate of surgical
site and other hospital-acquired infections (HAIs). Not only does
anesthesiologists’ and nurse anesthetists’ compliance with the relevant
quality measures help the hospitals’ quality scores and satisfy PQRS
requirements, preventing HAIs is good for patients and saves on health
care system costs.
Compliance with quality
standards and improvement upon current scores are often elements in
negotiations with hospitals, ambulatory surgical centers and, more and
more, third-party payers. When it comes to including performance
bonuses in contracts, the principle is sound, but the dollar value has
been elusive. A new study published in the online edition of JAMA
Internal Medicine on September 2, 2013, Health Care-Associated Infections: A Meta-analysis of Costs and Financial Impact on the US Health Care System
by Zimlichman et al. at the Brigham & Women’s Hospital in Boston,
analyzed the literature and available databases to determine...
Anesthesiologists
increasingly point to their role in driving down the rate of surgical
site and other hospital-acquired infections (HAIs). Not only does
anesthesiologists’ and nurse anesthetists’ compliance with the relevant
quality measures help the hospitals’ quality scores and satisfy PQRS
requirements, preventing HAIs is good for patients and saves on health
care system costs.
Compliance with quality
standards and improvement upon current scores are often elements in
negotiations with hospitals, ambulatory surgical centers and, more and
more, third-party payers. When it comes to including performance
bonuses in contracts, the principle is sound, but the dollar value has
been elusive. A new study published in the online edition of JAMA
Internal Medicine on September 2, 2013, Health Care-Associated Infections: A Meta-analysis of Costs and Financial Impact on the US Health Care System
by Zimlichman et al. at the Brigham & Women’s Hospital in Boston,
analyzed the literature and available databases to determine...
4331 Hits
 On October 1, 2014, the United States health care system will undergo a major transformation. We will transition from the decades-old Ninth Edition of the International Classification of Diseases (ICD-9) set of diagnosis and inpatient procedure codes to the Tenth Edition of those code sets—or ICD-10. The Tenth Edition is the version currently used by most developed countries throughout the world. ICD-10 allows for greater specificity and detail in describing a patient’s diagnosis and in classifying inpatient procedures, so reimbursement can better reflect the intensity of the patient’s condition and diagnostic needs.
This transition will have a major impact on anyone who uses health care information that contains a diagnosis and/or inpatient procedure code, including hospitals, physicians, other providers, payers, clearinghouses, billing companies, etc.
The change will affect all covered entities as defined by the Health Insurance Portability and Accountability Act of 1996 (HIPAA). Covered entities are required to adopt...
On October 1, 2014, the United States health care system will undergo a major transformation. We will transition from the decades-old Ninth Edition of the International Classification of Diseases (ICD-9) set of diagnosis and inpatient procedure codes to the Tenth Edition of those code sets—or ICD-10. The Tenth Edition is the version currently used by most developed countries throughout the world. ICD-10 allows for greater specificity and detail in describing a patient’s diagnosis and in classifying inpatient procedures, so reimbursement can better reflect the intensity of the patient’s condition and diagnostic needs.
This transition will have a major impact on anyone who uses health care information that contains a diagnosis and/or inpatient procedure code, including hospitals, physicians, other providers, payers, clearinghouses, billing companies, etc.
The change will affect all covered entities as defined by the Health Insurance Portability and Accountability Act of 1996 (HIPAA). Covered entities are required to adopt...
3706 Hits
 There has been substantial growth in the number of ambulatory surgery centers across the United States. With the advancement in technology for non-invasive procedures, and shorter-acting anesthetics, more patients are being seen in the freestanding surgery facility (FSF). However, the trend in patient co-morbidities, i.e., obesity, diabetes, cardiac, and respiratory diseases has also risen, increasing the anesthetic risk even though low risk procedures are performed. The most common malpractice claims have been associated with diagnostic procedures performed in ambulatory surgery centers under monitored anesthesia care (MAC) with patient co-morbidities as contributing factors. The morbidity and mortality of ambulatory surgery patients has led to an increased concern for patient safety in freestanding facilities. Of particular concern is sedation, specifically in gastroenterology (GI) centers. Yet, the Journal of the American Medical Association (JAMA) recently reported that two-thirds of the anesthesia procedures provided during colonoscopies and endoscopies (EGDs) were on “low-risk patients;” suggesting...
There has been substantial growth in the number of ambulatory surgery centers across the United States. With the advancement in technology for non-invasive procedures, and shorter-acting anesthetics, more patients are being seen in the freestanding surgery facility (FSF). However, the trend in patient co-morbidities, i.e., obesity, diabetes, cardiac, and respiratory diseases has also risen, increasing the anesthetic risk even though low risk procedures are performed. The most common malpractice claims have been associated with diagnostic procedures performed in ambulatory surgery centers under monitored anesthesia care (MAC) with patient co-morbidities as contributing factors. The morbidity and mortality of ambulatory surgery patients has led to an increased concern for patient safety in freestanding facilities. Of particular concern is sedation, specifically in gastroenterology (GI) centers. Yet, the Journal of the American Medical Association (JAMA) recently reported that two-thirds of the anesthesia procedures provided during colonoscopies and endoscopies (EGDs) were on “low-risk patients;” suggesting...
3898 Hits
In order to be their hospitals’ valued partners, anesthesiologists should understand the needs and forces driving the institutions’ leadership. Some of the strongest of those forces today are creating a wave of merger and acquisition (M&A) activity. In 2012 there were more than 100 deals in the U.S., twice as many as three years earlier. If the relationship dynamics do not encourage partnership between the group and the C-suite, it is nevertheless important to be able to gauge whether one’s hospital is going in the right direction (or staying in the right place).
A recent report from the management consulting firm Strategy&, Succeeding in Hospital and Health Systems M&A: Why So Many Deals Have Failed, and How to Succeed in the Future, is instructive.
In the first of a pair of studies, the authors found that the majority of hospital and health system mergers in the period 1998-2008 had failed to...
3571 Hits
 “The Competition”
These days I hear that term from more and more anesthesia group leaders, and I’m sure that you’re thinking about it more than you’d like.
From the Latin root competitionem, its meaning originated in the sense of rivalry, of a contest for something. Since at least the 1790s, it’s been used to describe rivalry in the marketplace.
Ask yourself what “the competition” means to you. What comes to mind?
In working with anesthesia group leaders across the country, my regular experience is that they envision the competition as another anesthesia group, whether from across the county or across the country. These days, the image that often first comes to mind is that of the predatory staffing-service model.
I certainly can’t fault these group leaders because, especially these days, there is tremendous competitive pressure from outside entities coveting your facility contracts.
So, for most group leaders protecting their practice from...
“The Competition”
These days I hear that term from more and more anesthesia group leaders, and I’m sure that you’re thinking about it more than you’d like.
From the Latin root competitionem, its meaning originated in the sense of rivalry, of a contest for something. Since at least the 1790s, it’s been used to describe rivalry in the marketplace.
Ask yourself what “the competition” means to you. What comes to mind?
In working with anesthesia group leaders across the country, my regular experience is that they envision the competition as another anesthesia group, whether from across the county or across the country. These days, the image that often first comes to mind is that of the predatory staffing-service model.
I certainly can’t fault these group leaders because, especially these days, there is tremendous competitive pressure from outside entities coveting your facility contracts.
So, for most group leaders protecting their practice from...
3761 Hits
 On January 25, 2013, the US Department of Health and Human Services (HHS) Office of Civil Rights (OCR) issued its long-awaited Health Insurance Portability and Accountability Act of 1996 (HIPAA) final omnibus regulations (Final Rule). The Final Rule modified the HIPAA Privacy, Security, Enforcement and Breach Notification Rules (HIPAA Rules) and is comprised of four sub-rules:
Final modifications to the HIPAA Privacy, Security, and Enforcement Rules mandated by the Health Information Technology for Economic and Clinical Health (HITECH) Act;
A final rule adopting changes to the HIPAA Enforcement Rule to incorporate the increased and tiered civil money penalty structure as set forth by HITECH;
A final Breach Notification rule; and
A final rule modifying the Privacy Rule as required by the Genetic Information Nondiscrimination Act (GINA).
While the Final Rule is effective March 26, 2013, compliance with the provisions of the Final Rule is not required until September 23, 2013....
On January 25, 2013, the US Department of Health and Human Services (HHS) Office of Civil Rights (OCR) issued its long-awaited Health Insurance Portability and Accountability Act of 1996 (HIPAA) final omnibus regulations (Final Rule). The Final Rule modified the HIPAA Privacy, Security, Enforcement and Breach Notification Rules (HIPAA Rules) and is comprised of four sub-rules:
Final modifications to the HIPAA Privacy, Security, and Enforcement Rules mandated by the Health Information Technology for Economic and Clinical Health (HITECH) Act;
A final rule adopting changes to the HIPAA Enforcement Rule to incorporate the increased and tiered civil money penalty structure as set forth by HITECH;
A final Breach Notification rule; and
A final rule modifying the Privacy Rule as required by the Genetic Information Nondiscrimination Act (GINA).
While the Final Rule is effective March 26, 2013, compliance with the provisions of the Final Rule is not required until September 23, 2013....
3366 Hits
 There is no doubt that the emergence of the Electronic Health Record (EHR) program is changing the way providers capture documentation on the front end. According to the 2012 NCHS Data Brief, 55 percent of physician groups have already adopted an EHR. Among the 45 percent that have yet to implement an EHR system, nearly half plan to purchase or use a system already purchased this year.1 Hospitals are also purchasing and installing EHRs at a rapid rate.
EHR templates are rapidly gaining footholds despite some growing pains. CMS has issued advice on the use of checkboxes and drop-down menus accommodating discrete data capture. Despite access to such “documentation tools” via point-and-click templates, most physicians are complaining that it takes longer to document an encounter in an EHR than to previously dictate it. The RAND Corporation released a paper describing the phenomenon that occurs when an industry’s technological capabilities improve at...
There is no doubt that the emergence of the Electronic Health Record (EHR) program is changing the way providers capture documentation on the front end. According to the 2012 NCHS Data Brief, 55 percent of physician groups have already adopted an EHR. Among the 45 percent that have yet to implement an EHR system, nearly half plan to purchase or use a system already purchased this year.1 Hospitals are also purchasing and installing EHRs at a rapid rate.
EHR templates are rapidly gaining footholds despite some growing pains. CMS has issued advice on the use of checkboxes and drop-down menus accommodating discrete data capture. Despite access to such “documentation tools” via point-and-click templates, most physicians are complaining that it takes longer to document an encounter in an EHR than to previously dictate it. The RAND Corporation released a paper describing the phenomenon that occurs when an industry’s technological capabilities improve at...
15334 Hits
 The anesthesia business, regardless of whether one chooses to define it as the practice of medicine, nursing, or some hybrid, is in the midst of upheaval. Increasing market consolidation, mergers, acquisitions and introduction of private equity funding have made the business of managing anesthesia delivery services increasingly complex. Bear in mind that delivering anesthesia and managing the delivery of anesthesia services are two very different things.
Our unparalleled improvements in patient safety, quality, and, ultimately, morbidity and mortality make us justifiably proud of the specialty’s success and the envy of the rest of health care. One would think that this remarkable history of clinical success would provide stability for the business side of anesthesia practice. After all, the clinical product that we provide is orders of magnitude safer than when I entered the specialty 25 years ago. If anything, however, I believe our advances have actually laid the foundation for the...
The anesthesia business, regardless of whether one chooses to define it as the practice of medicine, nursing, or some hybrid, is in the midst of upheaval. Increasing market consolidation, mergers, acquisitions and introduction of private equity funding have made the business of managing anesthesia delivery services increasingly complex. Bear in mind that delivering anesthesia and managing the delivery of anesthesia services are two very different things.
Our unparalleled improvements in patient safety, quality, and, ultimately, morbidity and mortality make us justifiably proud of the specialty’s success and the envy of the rest of health care. One would think that this remarkable history of clinical success would provide stability for the business side of anesthesia practice. After all, the clinical product that we provide is orders of magnitude safer than when I entered the specialty 25 years ago. If anything, however, I believe our advances have actually laid the foundation for the...
4207 Hits
 Over the New Year holiday, Congress finally passed legislation to stop the U.S. economy from going over the fiscal cliff. The new law included a temporary reprieve from the 26.5 percent cut provided for by the Medicare Sustainable Growth Rate (SGR) formula. There will be no SGR reduction throughout 2013—a development that lets us all breathe a deep sigh of relief, even though the formula itself, and its future depredations, are still in the law. Medicare payments to physicians and hospitals are not inviolate for the coming year, it must be noted: automatic two-percent reductions will hit Medicare as part of the “sequestration” process just two months from now if Congress and the White House do not reach another deal.
For many anesthesia practices, the runup to negotiations with hospitals and payers is a cliffhanger—indeed, even contemplating future negotiations often feels precarious. Last year, one of the national anesthesia practice management...
Over the New Year holiday, Congress finally passed legislation to stop the U.S. economy from going over the fiscal cliff. The new law included a temporary reprieve from the 26.5 percent cut provided for by the Medicare Sustainable Growth Rate (SGR) formula. There will be no SGR reduction throughout 2013—a development that lets us all breathe a deep sigh of relief, even though the formula itself, and its future depredations, are still in the law. Medicare payments to physicians and hospitals are not inviolate for the coming year, it must be noted: automatic two-percent reductions will hit Medicare as part of the “sequestration” process just two months from now if Congress and the White House do not reach another deal.
For many anesthesia practices, the runup to negotiations with hospitals and payers is a cliffhanger—indeed, even contemplating future negotiations often feels precarious. Last year, one of the national anesthesia practice management...
3233 Hits
 I am an anesthesiologist. The leadership of my small group of 15 physicians has been negotiating a merger with the large group in a nearby city. They have made some compelling arguments for the strategic advantages of an affiliation with a larger entity. But as logical as the rationale for merging is, so are the concerns and the questions raised by detractors. It is just not clear that all the disruption of closing out our current entity and transitioning to employment status with the big group will result in a more favorable situation for us as individuals or even as a division of the new entity. I personally worry about losing control of my practice and the clinical autonomy that attracted me to this practice in the first place. The fact is that I am still unsure how I will vote when we all get together to make a final...
I am an anesthesiologist. The leadership of my small group of 15 physicians has been negotiating a merger with the large group in a nearby city. They have made some compelling arguments for the strategic advantages of an affiliation with a larger entity. But as logical as the rationale for merging is, so are the concerns and the questions raised by detractors. It is just not clear that all the disruption of closing out our current entity and transitioning to employment status with the big group will result in a more favorable situation for us as individuals or even as a division of the new entity. I personally worry about losing control of my practice and the clinical autonomy that attracted me to this practice in the first place. The fact is that I am still unsure how I will vote when we all get together to make a final...
7763 Hits
 Noah Rosenberg, M.D.Resident, Department of Family & Community Medicine, University of Massachusetts Memorial Medical Center, Worcester, MA
Fred E. Shapiro, D.O.Assistant Professor of Anesthesia, Harvard Medical School, Boston, ISOBS Founder
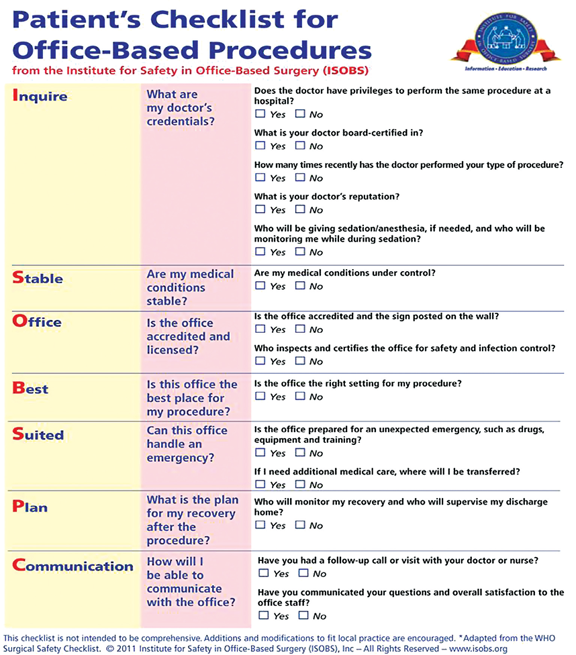
The Institute for Safety in Office-Based Surgery (ISOBS), an independent, non-profit 501(c)(3) organization, has developed a safety checklist for use in the office-based setting. A recent study to be published in the journal ePlastydemonstrated a more than 75% reduction in the number of surgical complications with use of the ISOBS Safety Checklist (see below for citation). While this positive effect on surgical complications validates much of the data already collected in the inpatient setting, it also clearly emphasizes the need for a tailored patient safety approach to the office-based setting. For that reason, ISOBS has developed a second checklist for use by patients to engage them in office-based surgical safety.
The ISOBS Patient Checklist (ISOBS PC) contains a number of questions...
Noah Rosenberg, M.D.Resident, Department of Family & Community Medicine, University of Massachusetts Memorial Medical Center, Worcester, MA
Fred E. Shapiro, D.O.Assistant Professor of Anesthesia, Harvard Medical School, Boston, ISOBS Founder
The Institute for Safety in Office-Based Surgery (ISOBS), an independent, non-profit 501(c)(3) organization, has developed a safety checklist for use in the office-based setting. A recent study to be published in the journal ePlastydemonstrated a more than 75% reduction in the number of surgical complications with use of the ISOBS Safety Checklist (see below for citation). While this positive effect on surgical complications validates much of the data already collected in the inpatient setting, it also clearly emphasizes the need for a tailored patient safety approach to the office-based setting. For that reason, ISOBS has developed a second checklist for use by patients to engage them in office-based surgical safety.
The ISOBS Patient Checklist (ISOBS PC) contains a number of questions...
4215 Hits
“Much has changed in health
care since HIPAA was enacted over fifteen years ago,” said HHS Secretary
Kathleen Sebelius in the Department of Health and Human Services’
January 17th press release announcing the publication of the
long-awaited final omnibus rule with Modifications to the HIPAA Privacy,
Security, Enforcement and Breach Notification Rules under the Health
Information Technology for Economic and Clinical Health Act and the
Genetic Information Nondiscrimination Act. “The new rule will help
protect patient privacy and safeguard patients’ health information in an
ever expanding digital age.”
The final omnibus rule will
go into effect on March 26, 2013. Covered entities such as anesthesia
and pain medicine practices and billing companies including ABC—and
their business associates—must be in compliance by September 23, 2013.
The final rule changes HIPAA in several important ways:
It toughens the definition and consequences of failure to notify affected parties of security and privacy breaches;It strengthens...
4285 Hits
The 2013 CPT®
Changes and Codebook are now available to health care providers.
Overall, the 2013 changes include 186 new codes, 119 deleted codes, and
263 revised codes. In addition CPT revised 18 modifiers and updated 150
guidelines. The very good news for anesthesia and pain management
providers is only a small handful of these changes directly impact the
services they routinely provide. Following are general comments
regarding the 2013 changes:
No Anesthesia codes were deleted, revised, or added for 2013.Pain management providers should take note of the four revised codes
and one new code in the nervous system section of CPT 2013. The
majority of changes occur in the denervation subsection, where CPT
revised codes 64612 and 64614 and added 64615 for bilateral
chemodenervation of muscles innervated by the facial, trigeminal,
cervical spinal and accessory nerves.CPT also changed the parenthetical note for code 76942, ultrasound
guidance for needle placement (eg,...
14567 Hits
 MEDICARE PAYMENTS AFTER DECEMBER 31st
If we go into the New Year without
legislation to stop the economy from going over the fiscal cliff—as
appears almost certain—there will be no just-in-time SGR fix either.
The Medicare conversion factor applicable to services provided from
January 1st onwards will be 26.5% lower, unless and until Congress
corrects the problem. Since the earliest that Medicare will pay claims
will be January 14th, however, there is time for Congress to take the
necessary action and prevent any remittances from going out at the lower
rate, subject to later adjustment. It is instructive to look at a
six-year history of the dates on which Congress passed legislation each
year avoiding the impact of the SGR (American Medical News, December 24,
2012):
2006-4.4%0.2%Feb. 8, 2006*
2007-5%0%Dec. 20, 2006
2008 (Jan.–June)-10.1%0.5%Dec. 29, 2007
2008 (July–Dec.)-10.6%0%July 15, 2008*
2009N/A1.1%N/A
2010 (Jan.–Feb.)-21.3%0%Dec. 19, 2009
2010 March-21.3%0%March 2, 2010*
2010...
MEDICARE PAYMENTS AFTER DECEMBER 31st
If we go into the New Year without
legislation to stop the economy from going over the fiscal cliff—as
appears almost certain—there will be no just-in-time SGR fix either.
The Medicare conversion factor applicable to services provided from
January 1st onwards will be 26.5% lower, unless and until Congress
corrects the problem. Since the earliest that Medicare will pay claims
will be January 14th, however, there is time for Congress to take the
necessary action and prevent any remittances from going out at the lower
rate, subject to later adjustment. It is instructive to look at a
six-year history of the dates on which Congress passed legislation each
year avoiding the impact of the SGR (American Medical News, December 24,
2012):
2006-4.4%0.2%Feb. 8, 2006*
2007-5%0%Dec. 20, 2006
2008 (Jan.–June)-10.1%0.5%Dec. 29, 2007
2008 (July–Dec.)-10.6%0%July 15, 2008*
2009N/A1.1%N/A
2010 (Jan.–Feb.)-21.3%0%Dec. 19, 2009
2010 March-21.3%0%March 2, 2010*
2010...
4353 Hits
 [Author’s Note: A version of this article originally appeared in the August 2012 issue of Anesthesiology News.]
In a much awaited pronouncement, on June 1, 2012, the U.S. Department of Health and Human Service’s Office of Inspector General issued Advisory Opinion 12-06 addressing the propriety of two popular schemes to extract money from anesthesiologists, the so-called “company model” and the purported “management fee.”
The advisory opinion could not be more welcome: Just as Willie Sutton, the bank robber, targeted banks “because that’s where the money is,” owners of ambulatory surgery centers continue seek a share of anesthesia fees.
According to a survey conducted by the American Society of Anesthesiologists, 41% of the responding anesthesia practices (125 out of 308) reported being requested by an ASC or its referring physician practice to adopt a company model. Not surprisingly, those 125 practices reported that out of the total 332 requests to participate in...
[Author’s Note: A version of this article originally appeared in the August 2012 issue of Anesthesiology News.]
In a much awaited pronouncement, on June 1, 2012, the U.S. Department of Health and Human Service’s Office of Inspector General issued Advisory Opinion 12-06 addressing the propriety of two popular schemes to extract money from anesthesiologists, the so-called “company model” and the purported “management fee.”
The advisory opinion could not be more welcome: Just as Willie Sutton, the bank robber, targeted banks “because that’s where the money is,” owners of ambulatory surgery centers continue seek a share of anesthesia fees.
According to a survey conducted by the American Society of Anesthesiologists, 41% of the responding anesthesia practices (125 out of 308) reported being requested by an ASC or its referring physician practice to adopt a company model. Not surprisingly, those 125 practices reported that out of the total 332 requests to participate in...
4998 Hits
 The acronym “HIPAA” has become a household name since the enactment of the Health Information Portability and Accountability Act of 1996, which, among other things, established rules for protecting and securing patients’ health information. In fact, it is not uncommon to hear about breaches of patient information costing healthcare providers and suppliers six and seven figure civil monetary penalties or settlements. Typically, such settlements and penalties have arisen out of patient complaints that the privacy of their protected health information (PHI) has been compromised. However, beginning November 2011, patient complaints will not be the only way in which the Department of Health and Human Services (HHS) Office of Civil Rights (OCR) will learn about non-compliant entities.Section 13411 of the American Recovery and Reinvestment Act of 2009, which established the Health Information Technology for Economic and Clinical Health (HITECH) Act, requires the Secretary of HHS to “provide for periodic audits to ensure...
The acronym “HIPAA” has become a household name since the enactment of the Health Information Portability and Accountability Act of 1996, which, among other things, established rules for protecting and securing patients’ health information. In fact, it is not uncommon to hear about breaches of patient information costing healthcare providers and suppliers six and seven figure civil monetary penalties or settlements. Typically, such settlements and penalties have arisen out of patient complaints that the privacy of their protected health information (PHI) has been compromised. However, beginning November 2011, patient complaints will not be the only way in which the Department of Health and Human Services (HHS) Office of Civil Rights (OCR) will learn about non-compliant entities.Section 13411 of the American Recovery and Reinvestment Act of 2009, which established the Health Information Technology for Economic and Clinical Health (HITECH) Act, requires the Secretary of HHS to “provide for periodic audits to ensure...
2005 Hits