This tag contains 2 private blog which isn't listed here.
 Every year, the time comes to begin looking at one or a set of payor contracts. A multitude of questions abound regarding appropriate rates, term length, and whether or not to participate or stay on panel. These are all good questions to raise. But are these the only questions to ask? This article seeks to explore the value of planning for payor negotiations.As a backdrop to the planning, it is important to remember the value of strategic planning as described by Sun Tzu:The general who wins a battle makes many calculations in his temple where the battle is fought. The general who loses a battle makes but few calculations beforehand. Thus do many calculations lead to victory, and few calculations to defeat: how much more no calculation at all! It is by attention to this point that I can foresee who is likely to win or lose.1The point is primarily to...
Every year, the time comes to begin looking at one or a set of payor contracts. A multitude of questions abound regarding appropriate rates, term length, and whether or not to participate or stay on panel. These are all good questions to raise. But are these the only questions to ask? This article seeks to explore the value of planning for payor negotiations.As a backdrop to the planning, it is important to remember the value of strategic planning as described by Sun Tzu:The general who wins a battle makes many calculations in his temple where the battle is fought. The general who loses a battle makes but few calculations beforehand. Thus do many calculations lead to victory, and few calculations to defeat: how much more no calculation at all! It is by attention to this point that I can foresee who is likely to win or lose.1The point is primarily to...
1718 Hits
 Abby Pendleton, Esq., The Health Law Partners, P.C., Southfield, MIStephanie P. Ottenwess, Esq., The Health Law Partners, P.C., Los Angeles, CAOn March 7, 2012, the Centers for Medicare and Medicaid Services (CMS) published its Notice of Proposed Rule Making (NPRM, or proposed rule) for Stage 2 user requirements for the Medicare/Medicaid Electronic Health Record (EHR) Incentive Program (“meaningful use,” or MU) in the Federal Register. 77 FR 13698.1 There is a three pronged focus to the Stage 2 criteria: standardizing data formats to dramatically simplify how information is both captured and shared across disparate IT systems in order to be better able to coordinate care with other physicians; ensuring that patients be able to access and easily download their healthcare records and images for their own use; and expanding the scope of tracked quality metrics to include specialists and to reflect and improve specific patient outcomes as well as care coordination.Although subsequent to...
Abby Pendleton, Esq., The Health Law Partners, P.C., Southfield, MIStephanie P. Ottenwess, Esq., The Health Law Partners, P.C., Los Angeles, CAOn March 7, 2012, the Centers for Medicare and Medicaid Services (CMS) published its Notice of Proposed Rule Making (NPRM, or proposed rule) for Stage 2 user requirements for the Medicare/Medicaid Electronic Health Record (EHR) Incentive Program (“meaningful use,” or MU) in the Federal Register. 77 FR 13698.1 There is a three pronged focus to the Stage 2 criteria: standardizing data formats to dramatically simplify how information is both captured and shared across disparate IT systems in order to be better able to coordinate care with other physicians; ensuring that patients be able to access and easily download their healthcare records and images for their own use; and expanding the scope of tracked quality metrics to include specialists and to reflect and improve specific patient outcomes as well as care coordination.Although subsequent to...
2110 Hits
 The Anesthesia Quality Institute was chartered in 2009, and it began collecting case data in the National Anesthesia Clinical Outcome Registry (NACOR) on January 1, 2010. NACOR was designed to harness the power of the Information Age by aggregating and analyzing large quantities of data. Unlike traditional registries that depend on a trained abstractor to examine medical records and pull out the facts of interest, NACOR accumulates data by direct reporting from the electronic health records (EHR) that are in use every day, including administrative systems such as the ABC billing software and clinical support systems such as ePreop. As anesthesia practices become increasingly digital — driven by the “meaningful use” requirements of the federal government discussed elsewhere in this issue of the Communiqué — even larger quantities and types of data will be available. The barrier is no longer the creation of digital records; it is now the enormous challenge...
The Anesthesia Quality Institute was chartered in 2009, and it began collecting case data in the National Anesthesia Clinical Outcome Registry (NACOR) on January 1, 2010. NACOR was designed to harness the power of the Information Age by aggregating and analyzing large quantities of data. Unlike traditional registries that depend on a trained abstractor to examine medical records and pull out the facts of interest, NACOR accumulates data by direct reporting from the electronic health records (EHR) that are in use every day, including administrative systems such as the ABC billing software and clinical support systems such as ePreop. As anesthesia practices become increasingly digital — driven by the “meaningful use” requirements of the federal government discussed elsewhere in this issue of the Communiqué — even larger quantities and types of data will be available. The barrier is no longer the creation of digital records; it is now the enormous challenge...
4038 Hits
October 1, 2012, as we noted in last week’s Alert, is the deadline for ambulatory surgical centers to begin reporting quality measures to CMS or face payment penalties. October 1st is also a momentous date for hospitals, with the start of the Medicare Hospital Inpatient Value-Based Purchasing (VBP) Program.Value-Based Purchasing for HospitalsThe VBP Program is scheduled to launch a week from now, as required by the Affordable Care Act. This program marks the beginning of an historic change in how Medicare pays health care providers and facilities—for the first time, hospitals across the country will be paid for inpatient acute care services based on care quality, not on the quantity of the services they provide.In fiscal year 2013, which starts on October 1st, the VBP Program will pay out an estimated $850 million to more than 3,500 participating hospitals based on their overall performance on a set of twenty quality measures....
3768 Hits
New Technology Enables Anesthesiologists and Pain Management Specialists to Attest to Meaningful UseWith the deadline fast approaching, more and more anesthesiologists are wondering if there is a quick and easy way to qualify for the Medicare Meaningful Use Incentive.The Medicare and Medicaid EHR Incentive Program provides a financial incentive of up to $44,000 per provider for achieving "meaningful use," which is the use of certified electronic health record(EHR) technology to achieve health and efficiency goals. Stage 1 EHR meaningful use is based on core and menu objectives for eligible professionals as outlined by CMS—which are intended to set a baseline for electronic data capture and information sharing.ABC Can Help You Reap the Benefits of Meaningful Use Through Full EHR with F1RSTUseAnesthesia Business Consultants, LLC (ABC) is pleased to offer the anesthesia community a first—a viable way for anesthesiology and pain management practices to attest to Stage 1 Meaningful Use. Introducing F1RSTUse,...
1968 Hits
We are in the fifth year of Medicare’s Physician Quality Reporting System (PQRS) and most anesthesiologists and nurse anesthetists are at least aware of the program, even if they are not participating. Now it is the turn of the ambulatory surgery centers (ASCs) to start reporting quality measures to CMS or face payment penalties.Not only are anesthesiologists generally involved in the quality and safety protocols that ASCs must report, many are in leadership or management positions in their ASCs and have a particular interest in compliance with reporting requirements. Whether or not they are directly responsible for the completeness and accuracy of the reporting—the new ASC requirements do not in any way require anesthesiologists to report any measures, but some may voluntarily assume the role within and for their facility—ASC anesthesiologists will benefit from understanding what procedural changes the facility is making, and why. Beginning October 1, 2012, the ASC Quality Reporting...
3477 Hits
Many “Covered Entities” within the meaning of the privacy and security provisions of the Health Insurance and Portability Act of 1996 (HIPAA) are managing more and more of their patient information electronically. Indeed, not moving to electronic health records (EHRs) may cost physicians a percentage of their Medicare remittances—or at least the loss of a potential bonus of up to $44,000—under the EHR Incentive Program, as discussed in our last several Alerts.Collecting, analyzing, reporting and storing electronic patient information present perhaps even greater HIPAA challenges than does the use of paper records, however. Data entered on a computer can be copied more easily, more cheaply, more prolifically and even passively. Once unsecured data are moved from the computer on which they are created to other media, manually or wirelessly, controlling the information becomes nearly impossible. The key word in the preceding sentence is “unsecured.” The recently finalized HIPAA regulations on Breach Notification impose...
4560 Hits
Last week, we announced the availability of a new web-based electronic health record (EHR) that will permit anesthesiologists to satisfy the Meaningful Use requirements for the Medicare EHR Incentive Program. Although this technology, F1RSTUse, is relatively simple, requires little additional data entry and is an option for ABC clients and non-clients alike, it will not be the best solution for every reader. Those of you who are not in a position to implement F1RSTUse or any EHR will be interested in a new hardship exception created by CMS when it released the final regulation on the Stage 2 Meaningful Use requirements on August 23, 2012.Anesthesiologists not participating in the EHR Incentive Program are the targets of the new exception based on “scope of practice,” along with radiologists and pathologists. In the final rule, CMS added a new section, §495.102(d)(4)(iv), to the regulations which provides that “eligible professionals” (EPs) who designate their...
3423 Hits
New Technology Enables Anesthesiologists and Pain Management Specialists to Attest to Meaningful Use
On Thursday, August 23, 2012 the Centers for Medicare and Medicaid Services (CMS) released the final rule on Stage 2 of the federal electronic health record (EHR) system incentive program.ABC is very pleased to announce F1RSTUse, the first complete EHR platform built exclusively for anesthesiologists and pain management specialists to satisfy easily Stage 1 of Meaningful Use as required to earn the Medicare EHR incentive payment. Stage 1 requirements remain in effect for the next several years; one of the major changes of the August 23rd final rule was to extend the deadline to meet Stage 2 criteria until 2014. Other changes contained in the 672-page rule (PDF) will be reviewed in future Alerts.The industry has been discussing the impracticality of attesting to Meaningful Use with current technologies and relationships that are in place for anesthesia. We at ABC also noted the lack of ease implementing this requirement for the specialty. Attestation was...
3749 Hits
Advanced Integration Streamlines Data Collection to Speed Billing, Improve Efficiency and Enhance AnalysisAnesthesia Business Consultants (ABC) announces that it has partnered with Surgical Information Systems (SIS), a leading anesthesia information management system (AIMS) provider, to streamline revenue cycle workflow. The alliance provides integration that enables data captured in SIS’ AIMS to flow into ABC’s anesthesia billing tools to improve billing accuracy and timeliness. It also offers analytics capabilities that enable ABC clients to collect and analyze anesthesia-specific perioperative data.With over 300 successful perioperative implementations, SIS solutions deliver proven benefits to anesthesia providers and hospitals across the United States and Canada. SIS is recognized by top industry associations for its commitment to advance anesthesia solutions. SIS was the first AIMS provider to achieve Anesthesia Quality Institute (AQI) Preferred Vendor status, and SIS Anesthesia is exclusively endorsed by the American Hospital Association (AHA) indicating the solution has met AHA requirements for quality, integrity,...
5923 Hits
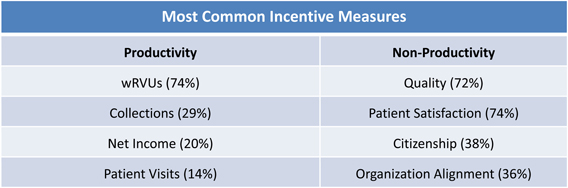 Preparing for negotiations requires an appreciation of the other side’s needs, wants, values and constraints. Anesthesiologists who have contracts with their hospitals or surgery centers are in a continuous cycle of negotiations—as soon as one contract is signed, it is time to start working toward the next agreement. One good place to start in understanding the facility’s position is to look at the advice hospitals are receiving from their consultants. Below is an article recently written for that audience by ABC Vice President for Regulatory Affairs & Research Joette Derricks, CPC, CHC, CMPE, CSSGB. This article addresses hospital employment of physicians who bill using RBRVS Relative Value Units, and of course anesthesiologists use the Relative Value Guide’s Base and Time Unit methodology and typically have group exclusive contracts to provide services to the hospital’s patients, but the discussion below can be read with the differences in mind. It is important to...
Preparing for negotiations requires an appreciation of the other side’s needs, wants, values and constraints. Anesthesiologists who have contracts with their hospitals or surgery centers are in a continuous cycle of negotiations—as soon as one contract is signed, it is time to start working toward the next agreement. One good place to start in understanding the facility’s position is to look at the advice hospitals are receiving from their consultants. Below is an article recently written for that audience by ABC Vice President for Regulatory Affairs & Research Joette Derricks, CPC, CHC, CMPE, CSSGB. This article addresses hospital employment of physicians who bill using RBRVS Relative Value Units, and of course anesthesiologists use the Relative Value Guide’s Base and Time Unit methodology and typically have group exclusive contracts to provide services to the hospital’s patients, but the discussion below can be read with the differences in mind. It is important to...
3699 Hits
 Does the title of this article seem boring – or “timeless,” for readers in a more generous mood? If the answer to either question is yes, that is not altogether a bad thing. The United States Supreme Court decision upholding the Patient Protection and Affordable Care Act alleviated much uncertainty about healthcare reform and all of its ramifications, at least until after the November elections. Trends in the delivery of healthcare that began some time ago will continue. “The coming years will bring continued dealmaking and greater scrutiny of hospital and physician performance on quality and cost control,” as speakers said at the June 2012 Healthcare Financial Management Association Annual National Institute. Quality, safety and practice management are as important as ever to the future of anesthesia practice.
Richard P. Dutton, MD, MBA, Executive Director of the Anesthesia Quality Institute, bridges the small valley between traditional mortality and morbidity (M&M) conferences...
Does the title of this article seem boring – or “timeless,” for readers in a more generous mood? If the answer to either question is yes, that is not altogether a bad thing. The United States Supreme Court decision upholding the Patient Protection and Affordable Care Act alleviated much uncertainty about healthcare reform and all of its ramifications, at least until after the November elections. Trends in the delivery of healthcare that began some time ago will continue. “The coming years will bring continued dealmaking and greater scrutiny of hospital and physician performance on quality and cost control,” as speakers said at the June 2012 Healthcare Financial Management Association Annual National Institute. Quality, safety and practice management are as important as ever to the future of anesthesia practice.
Richard P. Dutton, MD, MBA, Executive Director of the Anesthesia Quality Institute, bridges the small valley between traditional mortality and morbidity (M&M) conferences...
3653 Hits
 The Anesthesia Quality Institute was founded to create and maintain the National Anesthesia Clinical Outcomes Registry (NACOR). This project is now two and a half years old and more than 135 practices, including nine ABC clients, have contributed more than 5 million records to this “every case, every day” registry. Participants have online access to the NACOR Reporting Server, where they can see continually updated summaries of their practice performance and aggregated national benchmarks. This information, and the ability to slice and dice it to examine subsets of interest, is an important business and quality management tool. After all, what can’t be measured can’t be improved.
Or can it? Although we pride ourselves on our data-driven, scientific, high-tech practice, anesthesiology remains as much art as science. As the popularity of morbidity and mortality conferences attests, there is a lot to be learned from the unfortunate experience of others. Schadenfreude aside,...
The Anesthesia Quality Institute was founded to create and maintain the National Anesthesia Clinical Outcomes Registry (NACOR). This project is now two and a half years old and more than 135 practices, including nine ABC clients, have contributed more than 5 million records to this “every case, every day” registry. Participants have online access to the NACOR Reporting Server, where they can see continually updated summaries of their practice performance and aggregated national benchmarks. This information, and the ability to slice and dice it to examine subsets of interest, is an important business and quality management tool. After all, what can’t be measured can’t be improved.
Or can it? Although we pride ourselves on our data-driven, scientific, high-tech practice, anesthesiology remains as much art as science. As the popularity of morbidity and mortality conferences attests, there is a lot to be learned from the unfortunate experience of others. Schadenfreude aside,...
4283 Hits
This issue of the Communiqué is a keeper. On pages 6 through 10 you will find tables that lay out clearly the Electronic Health Records (EHR) incentive program’s Stage 1 Meaningful Use objectives, the recently proposed changes to Stage 1, and the potential Stage 2 objectives, measures and exclusions as proposed by CMS in March. The objectives, translated into measures, are capabilities that your EHR must have in order for you to qualify for the incentive, which is non-negligible at a maximum of $44,000 per physician, or to avoid the penalty for non-compliance. Even though the proposed changes discussed in the Meaningful Use article by Abby Pendleton, Esq. and Stephanie Ottenweis, Esq. are likely to be different in some respects when CMS issues the final regulation later in the year, it is worth familiarizing yourself with the proposals because understanding the final versions will be that much easier.The Meaningful Use article,...
3429 Hits
A change to some language in the Anesthesia Services chapter of the Medicare National Correct Coding Initiative (NCCI) manual recently created considerable confusion among participants in the on-line discussion maintained by the Medical Group Management Association (MGMA) for the Anesthesia Administration Assembly (AAA).The information that gave rise to the confusion has been clarified. The NCCI has confirmed that there has been no policy change here; epidurals and blocks placed preoperatively for the management of postoperative pain are still separately reportable and not bundled into the anesthesia service unless they are used as the method of administering the anesthesia itself. Because the issue of post-op pain management is a perennial hot topic, we take this opportunity to help ensure that no incorrect interpretations take root.Chapter II of the NCCI manual, “Anesthesia Services,” was revised effective January 1, 2012. It contains a number of statements that are consistent with the established principles of billing...
4421 Hits
The most significant change for anesthesia and pain medicine practices in the proposed Medicare Fee Schedule rule for 2013 (NPRM), released on July 6, 2012, was the proposal to allow nurse anesthetists to perform chronic pain services without physician supervision in those states that include such services in the scope of practice of nurse anesthesia. As noted in last week’s Alert, the 765-page NPRM contains many other potential changes. Highlights appear below.1. Medicare Payment Rates in 2013It comes as no surprise that the 27 percent cut mandated by the Sustainable Growth Rate (SGR) formula remains in place for now and will take effect on January 1, 2013, if Congress fails to act. Fear of the economic cliff that the entire country faces with mandatory spending reductions and the expiration of tax cuts early next year will undoubtedly affect how Congress deals with the SGR for 2013; what we cannot predict now...
4257 Hits
Anesthesiologists, nurse anesthetists and anesthesiologist assistants who last validated their enrollment in Medicare prior to March 25, 2011 are going to have to revalidate again by March 23, 2013. The revalidation is required under Section 6028 of the Affordable Care Act. According to this statutory provision, all providers and suppliers who were initially enrolled before March 25, 2011 and have not revalidated since then must revalidate their enrollment information within 60 days of receiving notice from their carriers, but no later than March 23, 2013.This is a hassle for physicians and allied health professionals who enrolled or revalidated as Medicare providers in 2009, 2010 or up until March 22nd of this year. Normally, providers have five years to revalidate. It may be of modest consolation that the burden will be considerably greater for institutional providers and especially for suppliers. That is because the revalidation is intended to combat Medicare fraud, by bringing...
3673 Hits
Do you check your professional association’s web site regularly? There is more practice-related information there than you may realize. One recent addition to the resources on the American Society of Anesthesiologists web site (www.asahq.org) is worth your special attention. The ASA Committee on Quality Management and Departmental Administration (QMDA) has produced a comprehensive set of questions for anesthesiologists and others involved in perioperative patient care that can guide the development of a quality program tailored to your own department.The QMDA Anesthesiology Department Quality Checklist is a “compendium of anesthesia safety and quality measures suitable as a reference for anesthesiology departments of any size as they develop a comprehensive set of quality standards.” It consists of separate sets of questions for these individuals and offices:Chair of AnesthesiaStaff AnesthesiologistSurgeonCRNA and/or AA Perioperative Nursing ManagerOperating Room NursePACU Nursing ManagerObstetric Nursing ManagerQuality ManagementAdministrationAnesthesia Technicianas well as for Office Based Anesthesia Facilities. The questions, and the answers received, can...
5397 Hits
State governments are under severe financial pressure. In the last few years, many of them have stepped up their efforts to collect unclaimed property held by private entities such as medical practices. Every state has an “escheat” or unclaimed property statute that places the burden on those holding such property to deliver it to the treasury or commerce department if the owner cannot be found. Escheatment is the general rule that abandoned or unclaimed property (of all kinds) becomes the property of the state.Several questions about our clients’ escheat policies and procedures have come up recently, suggesting that it is time for all to review their compliance with the applicable laws. This subject is governed by state statutes that vary in their requirements regarding attempts to notify the owner of the property, e.g., the patient; time limits for delivering the property to the authorities, and other financial procedures. Forty-two states (including...
4643 Hits
A product of 1989 legislation, the Physician Fee Schedule went into effect on January 1, 1992. (And William Hsiao, PhD, whose study of Resource-Based Relative Value Systems was the foundation for the change from charge-based payment methodology, is still teaching at the Harvard School of Public Health today.)The national anesthesia conversion factor (CF), unadjusted for geographic practice cost differences, was $13.68 in 1992, and the general CF for other services was $31.00. Twenty years later, the national anesthesia CF is $21.49, and the general CF is $34.04 – at least for the period ending on February 29, 2012. In mid-December, Congress passed the “Middle Class Tax Relief and Job Creation Act,” setting a zero percent update and postponing the scheduled 27.4 percent CF reduction mandated by the Sustainable Growth Rate (SGR) for just two months. If Congress cannot agree on a longer-term deal averting the SGR cuts, Medicare payments will drop...
6369 Hits