This tag contains 2 private blog which isn't listed here.
Although the editor, bless her heart, steadfastly refused to let me have a sneak, pre-publication peek at the other articles that appear alongside this one, my educated guess is that each of them purports to give you answers.I know that's why you usually read Communiqué. In fact, nearly every one of the hundreds of other articles that I've written ...
1633 Hits
• The 2018 CPT edition includes 170 new CPT codes, 60 revised codes and 82 deleted codes along with two new modifiers. It is important to understand the changes and what should be documented to support the utilization of these codes.• The majority of the changes for 2018 were new CPT codes added to the Surgery section, Pathology/Laboratory section ...
15241 Hits
Press releases following a recent publication in the British Medical Journal (BMJ) hysterically echoed the article's headline: "Medical error—the third leading cause of death in the U.S."1 The authors used a variety of published sources on the incidence, lethality and preventability of medical errors to produce an estimate of 251,000 deaths per yea...
2233 Hits
Will Latham, MBA President, Latham Consulting Group, Inc., Chattanooga, TNIn despair at the way its programs were organized, the business school at one university recruited as the director of programs a successful businessman, who had made a modest fortune in his own business and wanted to move on to a new career. "I will soon put some order in thi...
1813 Hits
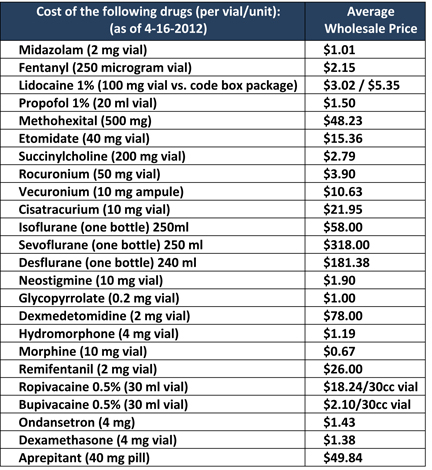 One way in which anesthesiologists can add value to their hospitals’ bottom line is by assuming responsibility for the cost of the drugs they order and administer.
The U.S. general anesthesia market size was approximately $2 billion in 2011 and is expected to grow at a moderate rate of 4% annually from 2011 to 2015, according to a Markets and Markets report. In addition, intravenous anesthetic drugs accounted for the largest share—65%—of the U.S. general anesthetics drugs market in 2011. Individual anesthesiology practitioners and groups have little control over total spending on drugs, just as they have little control over annual national spending on anesthesia services, but they can involve themselves in cost management locally, within their own institutions. As with most activities, success starts with knowledge.
First, anesthesiologists should be aware of the large variation in the cost of anesthetic agents and other medications used during the perioperative process. One...
One way in which anesthesiologists can add value to their hospitals’ bottom line is by assuming responsibility for the cost of the drugs they order and administer.
The U.S. general anesthesia market size was approximately $2 billion in 2011 and is expected to grow at a moderate rate of 4% annually from 2011 to 2015, according to a Markets and Markets report. In addition, intravenous anesthetic drugs accounted for the largest share—65%—of the U.S. general anesthetics drugs market in 2011. Individual anesthesiology practitioners and groups have little control over total spending on drugs, just as they have little control over annual national spending on anesthesia services, but they can involve themselves in cost management locally, within their own institutions. As with most activities, success starts with knowledge.
First, anesthesiologists should be aware of the large variation in the cost of anesthetic agents and other medications used during the perioperative process. One...
22978 Hits
 CMS defines surgical anesthesia time as “the continuous, actual presence of a qualified anesthesia provider. This time begins when the anesthesia provider begins preparing the patient for anesthesia in the operating room or equivalent area. Anesthesia time ends when the anesthesia provider is no longer in personal attendance.” The ASA Relative Value Guide has a similar definition: “anesthesia time begins when the anesthesiologist begins to prepare the patient for anesthesia care in the operating room or in an equivalent area and ends when the patient is safely placed under post-anesthesia supervision.” This is a typical “clear as mud” definition when it comes to anesthesia and CMS. Exactly what is an equivalent area? Is this “equivalent area” ambiguity something we can use to our advantage or is it a disadvantage? Could it be both? It all depends on how or who does the interpretation of the anesthesia record; nevertheless, as long as...
CMS defines surgical anesthesia time as “the continuous, actual presence of a qualified anesthesia provider. This time begins when the anesthesia provider begins preparing the patient for anesthesia in the operating room or equivalent area. Anesthesia time ends when the anesthesia provider is no longer in personal attendance.” The ASA Relative Value Guide has a similar definition: “anesthesia time begins when the anesthesiologist begins to prepare the patient for anesthesia care in the operating room or in an equivalent area and ends when the patient is safely placed under post-anesthesia supervision.” This is a typical “clear as mud” definition when it comes to anesthesia and CMS. Exactly what is an equivalent area? Is this “equivalent area” ambiguity something we can use to our advantage or is it a disadvantage? Could it be both? It all depends on how or who does the interpretation of the anesthesia record; nevertheless, as long as...
3485 Hits
 This post was written by:
Aman Mahajan, MD Chair, Department of Anesthesiology, University of California, Los Angeles, CA
Jody Locke, CPC Vice President of Anesthesia and Pain Management Services, ABC
Background
It is often suggested that an anesthesiology department should have more complete and readily accessible data about the clinical care provided in the operating rooms and the delivery suite than any other department of the facility; but how often is this actually the case? Anesthesia providers review and document enormous amounts of clinical detail and critical events for every patient they see, but little of this information is actually captured in a way that allows for its logical indexing and retrieval. Most anesthesia groups and their billing services have been so focused on the data necessary to calculate a charge and generate a claim that they have virtually ignored what is potentially the most valuable of information of all. The...
This post was written by:
Aman Mahajan, MD Chair, Department of Anesthesiology, University of California, Los Angeles, CA
Jody Locke, CPC Vice President of Anesthesia and Pain Management Services, ABC
Background
It is often suggested that an anesthesiology department should have more complete and readily accessible data about the clinical care provided in the operating rooms and the delivery suite than any other department of the facility; but how often is this actually the case? Anesthesia providers review and document enormous amounts of clinical detail and critical events for every patient they see, but little of this information is actually captured in a way that allows for its logical indexing and retrieval. Most anesthesia groups and their billing services have been so focused on the data necessary to calculate a charge and generate a claim that they have virtually ignored what is potentially the most valuable of information of all. The...
3954 Hits
The decisions that anesthesiologists and pain medicine specialists
must make are more fundamental and consequential than ever as we enter
the final months before implementation of Obamacare in January 2014.
Adding staff, adding locations or even altering income distribution
systems are easy decisions in comparison, especially since they lend
themselves to well-defined quantitative analysis. Creating and selecting
options that involve the very nature and identity of groups is much
more challenging. Three of the articles in this issue of the Communiqué
explore different aspects of the answer to the question, “How do we
secure our future?”
The broadest view and the most basic recommendations are to be found in Will Latham’s article Strengthening Your Anesthesiology Group.
Mr. Latham proposes two steps groups can take to reduce the pervasive
environmental uncertainty: strengthen group governance and, with a more
predictable decision-making process in place, develop a group-endorsed
strategic plan. From defining the group’s...
5006 Hits
Health insurance exchanges
(HIEs) will open in every state by October 1, 2013, as mandated by the
Affordable Care Act (ACA). Their basic role will be to permit consumers
to compare and purchase qualified insurance plans online. Estimates of
the numbers of individuals who will enroll in HIE plans during the
six-month enrollment period that starts on October 1st vary from seven
million (Congressional Budget Office) to four million (Citigroup
investor survey released last Monday). Many of these enrollees will be
eligible for federal subsidies to help pay for the coverage.
The issue for
anesthesiologists and other physicians is whether to participate in the
HIE health plans that are seeking to sign them up. The clock is
running; coverage under the HIE plans will begin as early as January 1,
2014. This Alert will discuss the questions and considerations that
will help groups decide how to proceed.
Bear in mind that some...
3310 Hits
The anesthesia community is rich in practice management educational resources.Since 1995, the American Society of Anesthesiologists has presented an annual conference on practice management in late January. The conference is now a three-day meeting with multiple tracks, including an all-day program for residents. According to the ASA, “This comprehensive educational event provides up-to-date information about the state of practice management including business and technology trends, changes in regulations and laws, and best practices to manage an anesthesiology practice in today’s environment.” Next year’s meeting will be held in Dallas on January 24-26, and is beneficial for anesthesiologists, practice administrators, allied health professionals, consultants and others. For further information, go to www.ASAhq.org.The Anesthesia Administration Assembly of the Medical Group Management Association hosts an annual national practice management meeting in the spring. Several hundred administrators and a growing number of anesthesiologists attend this three-day event. Like the ASA Practice Management Conference, the AAA meeting offers...
2235 Hits
 “Most people choose unhappiness over uncertainty.” — Timothy Ferris
Anesthesiology groups are facing unprecedented challenges. How will the Affordable Care Act affect them? What will happen when ACOs get up and running? Should our group sell to an investment group? Should we pursue hospital employment?
These are truly uncertain times.
Unfortunately many groups are in a reactive mode, struggling with how to deal with threats and opportunities in the marketplace. This is often because their governance and management processes were formed at a time when there were fewer stressors and challenges. Some group are sprinting towards relationships that appear to offer financial reward and some level of security, but at the same time have the potential to severely limit the group’s and the physician’s autonomy.
While there are situations where employment may be appropriate, many groups that pursue this course are “choosing unhappiness over uncertainty.”
If your group intends to remain...
“Most people choose unhappiness over uncertainty.” — Timothy Ferris
Anesthesiology groups are facing unprecedented challenges. How will the Affordable Care Act affect them? What will happen when ACOs get up and running? Should our group sell to an investment group? Should we pursue hospital employment?
These are truly uncertain times.
Unfortunately many groups are in a reactive mode, struggling with how to deal with threats and opportunities in the marketplace. This is often because their governance and management processes were formed at a time when there were fewer stressors and challenges. Some group are sprinting towards relationships that appear to offer financial reward and some level of security, but at the same time have the potential to severely limit the group’s and the physician’s autonomy.
While there are situations where employment may be appropriate, many groups that pursue this course are “choosing unhappiness over uncertainty.”
If your group intends to remain...
6586 Hits
If you are an
anesthesiologist practicing in a group of 100 or more eligible
professionals (EPs) and submitting claims to Medicare under a single
taxpayer number, you may be subject to the Value Based Payment Modifier
(VBPM) in 2015. By 2017, all physicians participating in
Fee-for-Service Medicare will be affected by the VBPM. This Alert is
intended to help anesthesiologists familiarize themselves with the VBPM.
The VBPM program,
as provided for in the Affordable Care Act, is designed to connect the
cost and quality of medical services in order to pay for “value” rather
than the quantity of care. It combines quality measures under the
Physician Quality Reporting System (PQRS) with cost measures and a
payment adjustment.
The VBPM and PQRS are
related but independent. Readers are reminded that EPs who do not
participate in PQRS in 2013 are subject to a -1.5% payment adjustment in 2015. Non-participation in 2014 and...
3833 Hits
 The specialty of anesthesiology is experiencing an unprecedented level of merger activity and practice acquisitions. The idea of two or more practices joining forces to secure their market position or enhance their strategic options is hardly a new phenomenon. The past few decades has seen the emergence of some very large anesthesia organizations that have dramatically changed the landscape in their respective markets. Once a pioneer in large group practice management, the Anesthesia Service Management Group (ASMG) and its 150 plus physicians in San Diego has become a model to emulate and refine. By some accounts, we have already reached a point where fewer than 100 organizations employ more than 15 percent of all anesthesia providers, but this is only a rough calculation, made especially challenging by the recent infusion of venture capital money that is inspiring an impressive list of practice acquisitions across the country. This dramatic rethinking of...
The specialty of anesthesiology is experiencing an unprecedented level of merger activity and practice acquisitions. The idea of two or more practices joining forces to secure their market position or enhance their strategic options is hardly a new phenomenon. The past few decades has seen the emergence of some very large anesthesia organizations that have dramatically changed the landscape in their respective markets. Once a pioneer in large group practice management, the Anesthesia Service Management Group (ASMG) and its 150 plus physicians in San Diego has become a model to emulate and refine. By some accounts, we have already reached a point where fewer than 100 organizations employ more than 15 percent of all anesthesia providers, but this is only a rough calculation, made especially challenging by the recent infusion of venture capital money that is inspiring an impressive list of practice acquisitions across the country. This dramatic rethinking of...
3389 Hits
 Anesthesiologists
increasingly point to their role in driving down the rate of surgical
site and other hospital-acquired infections (HAIs). Not only does
anesthesiologists’ and nurse anesthetists’ compliance with the relevant
quality measures help the hospitals’ quality scores and satisfy PQRS
requirements, preventing HAIs is good for patients and saves on health
care system costs.
Compliance with quality
standards and improvement upon current scores are often elements in
negotiations with hospitals, ambulatory surgical centers and, more and
more, third-party payers. When it comes to including performance
bonuses in contracts, the principle is sound, but the dollar value has
been elusive. A new study published in the online edition of JAMA
Internal Medicine on September 2, 2013, Health Care-Associated Infections: A Meta-analysis of Costs and Financial Impact on the US Health Care System
by Zimlichman et al. at the Brigham & Women’s Hospital in Boston,
analyzed the literature and available databases to determine...
Anesthesiologists
increasingly point to their role in driving down the rate of surgical
site and other hospital-acquired infections (HAIs). Not only does
anesthesiologists’ and nurse anesthetists’ compliance with the relevant
quality measures help the hospitals’ quality scores and satisfy PQRS
requirements, preventing HAIs is good for patients and saves on health
care system costs.
Compliance with quality
standards and improvement upon current scores are often elements in
negotiations with hospitals, ambulatory surgical centers and, more and
more, third-party payers. When it comes to including performance
bonuses in contracts, the principle is sound, but the dollar value has
been elusive. A new study published in the online edition of JAMA
Internal Medicine on September 2, 2013, Health Care-Associated Infections: A Meta-analysis of Costs and Financial Impact on the US Health Care System
by Zimlichman et al. at the Brigham & Women’s Hospital in Boston,
analyzed the literature and available databases to determine...
4326 Hits
 The American Medical
Association (AMA) and the Medical Group Management Association (MGMA)
offer tools that allow physicians, policy makers and others to evaluate
the performance of a number of third party payers including Medicare.
The AMA and MGMA information may help anesthesia and pain medicine
groups who contract with private payers to identify potential problem
areas and to prepare to negotiate for specific performance standards and
remedies for non-compliance.
The AMA’s National Health Insurer Report Card
contains metrics on the timeliness, transparency and accuracy of claims
processing by the payers analyzed. The information in the latest
annual report is derived from a random sampling of 2.6 million
electronic claims submitted by more than 450 physician practices across
41 states in February and March of this year to Aetna, Anthem Blue Cross
Blue Shield, Cigna, Health Care Service Corporation, Humana, Regence,
United Healthcare and Medicare. Below are some of the key findings...
The American Medical
Association (AMA) and the Medical Group Management Association (MGMA)
offer tools that allow physicians, policy makers and others to evaluate
the performance of a number of third party payers including Medicare.
The AMA and MGMA information may help anesthesia and pain medicine
groups who contract with private payers to identify potential problem
areas and to prepare to negotiate for specific performance standards and
remedies for non-compliance.
The AMA’s National Health Insurer Report Card
contains metrics on the timeliness, transparency and accuracy of claims
processing by the payers analyzed. The information in the latest
annual report is derived from a random sampling of 2.6 million
electronic claims submitted by more than 450 physician practices across
41 states in February and March of this year to Aetna, Anthem Blue Cross
Blue Shield, Cigna, Health Care Service Corporation, Humana, Regence,
United Healthcare and Medicare. Below are some of the key findings...
4289 Hits
The Centers for Medicare
& Medicaid Services (CMS) implemented the Comprehensive Error Rate
Testing (CERT) program to measure improper payments in the Medicare
Fee-for-Service (FFS) program. CERT is designed to comply with the
Improper Payments Information Act (IPIA) of 2002, as amended by the
Improper Payments Elimination and Recovery Improvement Act (IPERIA) of
2012. IPIA and IPERIA require the heads of Federal agencies, including
the Department of Health and Human Services (HHS), to annually review
programs it administers to improve agency efforts to reduce and recover
improper payments.
The Medicare FFS improper
payment rate was first measured in 1996. HHS Office of Inspector General
(OIG) was responsible for estimating the national Medicare FFS improper
payment rate from 1996 through 2002. Based on available resources, OIG
reviewed about 6,000 claims. Currently CERT selects a stratified random
sample of approximately 50,000 claims submitted to Part A/B Medicare
Administrative Contractors (MACs) and Durable Medical...
3879 Hits
 On October 1, 2014, the United States health care system will undergo a major transformation. We will transition from the decades-old Ninth Edition of the International Classification of Diseases (ICD-9) set of diagnosis and inpatient procedure codes to the Tenth Edition of those code sets—or ICD-10. The Tenth Edition is the version currently used by most developed countries throughout the world. ICD-10 allows for greater specificity and detail in describing a patient’s diagnosis and in classifying inpatient procedures, so reimbursement can better reflect the intensity of the patient’s condition and diagnostic needs.
This transition will have a major impact on anyone who uses health care information that contains a diagnosis and/or inpatient procedure code, including hospitals, physicians, other providers, payers, clearinghouses, billing companies, etc.
The change will affect all covered entities as defined by the Health Insurance Portability and Accountability Act of 1996 (HIPAA). Covered entities are required to adopt...
On October 1, 2014, the United States health care system will undergo a major transformation. We will transition from the decades-old Ninth Edition of the International Classification of Diseases (ICD-9) set of diagnosis and inpatient procedure codes to the Tenth Edition of those code sets—or ICD-10. The Tenth Edition is the version currently used by most developed countries throughout the world. ICD-10 allows for greater specificity and detail in describing a patient’s diagnosis and in classifying inpatient procedures, so reimbursement can better reflect the intensity of the patient’s condition and diagnostic needs.
This transition will have a major impact on anyone who uses health care information that contains a diagnosis and/or inpatient procedure code, including hospitals, physicians, other providers, payers, clearinghouses, billing companies, etc.
The change will affect all covered entities as defined by the Health Insurance Portability and Accountability Act of 1996 (HIPAA). Covered entities are required to adopt...
3703 Hits
 There has been substantial growth in the number of ambulatory surgery centers across the United States. With the advancement in technology for non-invasive procedures, and shorter-acting anesthetics, more patients are being seen in the freestanding surgery facility (FSF). However, the trend in patient co-morbidities, i.e., obesity, diabetes, cardiac, and respiratory diseases has also risen, increasing the anesthetic risk even though low risk procedures are performed. The most common malpractice claims have been associated with diagnostic procedures performed in ambulatory surgery centers under monitored anesthesia care (MAC) with patient co-morbidities as contributing factors. The morbidity and mortality of ambulatory surgery patients has led to an increased concern for patient safety in freestanding facilities. Of particular concern is sedation, specifically in gastroenterology (GI) centers. Yet, the Journal of the American Medical Association (JAMA) recently reported that two-thirds of the anesthesia procedures provided during colonoscopies and endoscopies (EGDs) were on “low-risk patients;” suggesting...
There has been substantial growth in the number of ambulatory surgery centers across the United States. With the advancement in technology for non-invasive procedures, and shorter-acting anesthetics, more patients are being seen in the freestanding surgery facility (FSF). However, the trend in patient co-morbidities, i.e., obesity, diabetes, cardiac, and respiratory diseases has also risen, increasing the anesthetic risk even though low risk procedures are performed. The most common malpractice claims have been associated with diagnostic procedures performed in ambulatory surgery centers under monitored anesthesia care (MAC) with patient co-morbidities as contributing factors. The morbidity and mortality of ambulatory surgery patients has led to an increased concern for patient safety in freestanding facilities. Of particular concern is sedation, specifically in gastroenterology (GI) centers. Yet, the Journal of the American Medical Association (JAMA) recently reported that two-thirds of the anesthesia procedures provided during colonoscopies and endoscopies (EGDs) were on “low-risk patients;” suggesting...
3893 Hits
Legislation to repeal the Sustainable Growth Rate (SGR) formula is emerging in the House of Representatives. On July 31st, the Energy and Commerce Committee voted unanimously to pass H.R. 2810, the Medicare Patient Access and Quality Improvement Act of 2013. This is the culmination of more than two years of work involving members of both the Energy and Commerce Committee and the House Ways and Means Committee, with feedback from healthcare providers. The bill now advances to the full Ways and Means Committee; the Senate Finance Committee is expected to produce its version in the fall.Summary of H.R. 2810In Phase I, “Stabilizing Fee Updates,” the bill would permanently repeal the SGR formula at the end of 2013 and replace it with fixed 0.5 percent updates to the Medicare Fee Schedule for each of the years 2014-2018. The positive and negative adjustments or incentives available through the PQRS and EHR programs would...
3197 Hits
 As of August 1st,
certain manufacturers of drugs, medical devices and biologicals are
tracking their payments to physicians, as required by the Physician
Payments Sunshine Act (Sunshine Act), which is part of the Affordable
Care Act. They will report payments and other items of value worth more
than $10, as well as certain ownership interests held by physicians and
immediate family members, to CMS annually. Reporting may begin
immediately, on a voluntary basis, and must begin by next January. CMS
will post the information, by physician, on a public, searchable
website.
CMS published the final regulations implementing the Act on February 1, 2013, and we summarized the rule in an Alert dated February 18th.
We refer readers to that Alert for information on the “applicable
manufacturers,” the definition of “covered products,” the form and
nature of payments and other “transfers of value” that must be reported
and reportable ownership and investment...
As of August 1st,
certain manufacturers of drugs, medical devices and biologicals are
tracking their payments to physicians, as required by the Physician
Payments Sunshine Act (Sunshine Act), which is part of the Affordable
Care Act. They will report payments and other items of value worth more
than $10, as well as certain ownership interests held by physicians and
immediate family members, to CMS annually. Reporting may begin
immediately, on a voluntary basis, and must begin by next January. CMS
will post the information, by physician, on a public, searchable
website.
CMS published the final regulations implementing the Act on February 1, 2013, and we summarized the rule in an Alert dated February 18th.
We refer readers to that Alert for information on the “applicable
manufacturers,” the definition of “covered products,” the form and
nature of payments and other “transfers of value” that must be reported
and reportable ownership and investment...
4054 Hits