The MACRA Quality Payment Program Is Here. Are You Ready?
You have heard of the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) and, most likely, its Quality Payment Program (QPP). But do you really know what it is? Do you know what it means to your practice? Do you know what your practice will need to do to thrive under the QPP? If you haven't already, you'll need to develop a firm understanding of the reimbursement landscape under MACRA. The time is now. Ready. Set. Go.
Background and ContextIn October 2016, the Centers for Medicare and Medicaid Services (CMS) issued the MACRA final rule with comment period titled "Medicare Program; Merit-Based Incentive Payment System (MIPS) and Alternative Payment Model (APM) Incentive under the Physician Fee Schedule, and Criteria for Physician-Focused Payment Models" (the Final Rule).1
Although it is more than 800 pages long, the MACRA final rule is designed to simplify participation by eligible clinicians. MACRA essentially replaces the old methodology used to determine the Medicare Physician Fee Schedule. This methodology, the Sustainable Growth Rate formula, threatened to impose payment cutbacks for physicians for more than a decade. The QPP aims to reward the provision of high quality and efficient services through a single cohesive system that unifies and replaces several different Medicare payment programs.
In 2015, CMS announced its goal of tying 90 percent of traditional Medicare payments to quality or value by 2018.2
The QPP advances these goals and related objectives. More specifically, CMS has clarified that the QPP aims to achieve the following:
- To improve beneficiary outcomes and engage patients through patient-centered policies.
- To enhance clinician experience through flexible and transparent program design and interactions with easy-to-use program tools.
- To increase the availability and adoption of robust Advanced APMs.
- To promote program understanding and maximize participation through customized communication, education, outreach and support that meets the needs of the diversity of physician practices and patients, especially the unique needs of small practices.
- To improve data and information sharing to provide accurate, timely and actionable feedback to clinicians and other stakeholders.
- To ensure operational excellence in program implementation and ongoing development.3
The QPP, which commenced on January 1, 2017 and is anticipated to continue through 2022 and beyond, will result in negative, neutral and positive adjustments to physician compensation. CMS refers to 2017 as a transitional year for the final rule and anticipates a ramp-up period as clinicians adjust to the QPP. Note, however, that, although the reporting periods commence during 2017, physicians will not receive increased reimbursement under the QPP until 2019. For this reason, participation in the QPP should be viewed as a long-term investment.
The QPP provides physicians with the ability to choose from one of two options: (1) the Advanced APMs and (2) the MIPS. It's important for physicians to understand their options and find the best QPP track for their particular practice.
Advanced Alternative Payment ModelsCMS anticipates that up to 120,000 clinicians will participate in the Advanced APM track during the 2017 performance year. Advanced APMs must satisfy certain criteria.
They must:
- Be CMS Innovation Center models, Shared Savings Program tracks or certain federal demonstration programs
- Use certified electronic health record (EHR) technology
- Base payments for services on quality measures comparable to those in MIPS
- Be a Medical Home Model expanded under CMS Innovation Center authority or require participants to bear more than nominal financial risk for losses
As this article is being written, CMS anticipates that the following models will be Advanced APMs for the 2017 performance year:
- Comprehensive End-Stage Renal Disease Care Model (two-sided risk arrangements)
- Comprehensive Primary Care Plus (CPC+)
- Medicare Shared Savings Program, Track 2
- Medicare Shared Savings Program, Track 3
- Next Generation Accountable Care Organization (ACO)
The list of participating Advanced APMs will change over time and updates will be posted on the CMS website.
Note that the QPP does not change the Advanced APMs, but rather, offers additional incentives for sufficiently participating in them. In the event that a practice receives 25 percent of Medicare covered professional services or sees 20 percent of its Medicare patients through an Advanced APM during 2017, then such practice will earn a five percent Medicare incentive payment during 2019.
Merit-Based Incentive Payment SystemCMS anticipates that most clinicians will participate in MIPS instead of the Advanced APM track, at least initially. The agency expects up to 500,000 clinicians to participate in MIPS during the 2017 performance year and that 90 percent of eligible clinicians will receive a neutral or positive payment adjustment.
The MIPS track is available not only to physicians but also to physician assistants, nurse practitioners, clinical nurse specialists and certified registered nurse anesthetists who bill more than $30,000 per year to Medicare and provide care to more than 100 Medicare patients per year.
The MIPS track replaces three Medicare programs: (1) the Medicare EHR Incentive Program (Meaningful Use); (2) the Physician Quality Reporting System (PQRS); and (3) the Value-Based Payment Modifier. Accordingly, the requirements for participating in MIPS are familiar to many physicians.
Performance Categories
For 2017, there are four weighted performance categories:
- Quality (which replaces the PQRS and carries a 60 percent weight)
- Improvement Activities (a new category that carries a 15 percent weight)
- Advancing Care Information (which replaces the Medicare EHR Incentive Program and carries a 25 percent weight)
- Cost (which replaces the Value-Based Payment Modifier but is not counted in the composite score until 2018)
CMS encourages clinicians to submit measures and activities in the quality, improvement activities and advancing care information categories in order to achieve the highest possible composite score. (When the cost measure becomes a part of the composite score in 2018, no reporting will be required because it will be calculated based on claims submitted.)
Specific measure-related and reporting requirements, exceptions and nuances will differ based on various circumstances. An abundance of additional information regarding the potential quality and advancing care information measures and the improvement activities can be found on the QPP website. This article covers some basic information.
Quality
For purposes of the quality category, most MIPS participants will need to report up to six quality measures (to the extent such measures are applicable), including an outcome measure, for a minimum of 90 days. Quality measures will be determined on an annual basis. For 2017, the anesthesiology measures are as follows:
- Anesthesiology Smoking Abstinence
- Coronary Artery Bypass Graft (CABG): Preoperative Beta-Blocker in Patients with Isolated CABG Surgery
- Documentation of Current Medications in the Medical Record
- Perioperative Temperature Management
- Post-Anesthetic Transfer of Care Measure: Procedure Room to a Post-Anesthesia Care Unit (PACU)
- Post-Anesthetic Transfer of Care: Use of Checklist or Protocol for Direct Transfer of Care from Procedure Room to Intensive Care Unit (ICU)
- Prevention of Central Venous Catheter (CVC)-Related Bloodstream Infections
- Prevention of Post-Operative Nausea and Vomiting (PONV): Combination Therapy
- Preventive Care and Screening: Screening for High Blood Pressure and Follow-Up Documented
Improvement Activities
The MIPS measure for improvement activities will require most participants to attest that they completed up to four improvement activities for a minimum of 90 days. Groups that are located in a rural or health professional shortage area or with 15 or fewer participants will need to attest that they completed up to two activities for a minimum of 90 days.
Advancing Care Information
For the 2017 transition year, participants may select from one of two sets of measures based on their EHR. Subject to certain exceptions, the MIPS advancing care information category requires that participants report on at least the following required categories for a minimum of 90 days:
- Security Risk Analysis
- Electronic Prescribing
- Patient Electronic Access
- Send Summary of Care
- Request/Accept Summary of Care
Reporting and Adjustments
Participating clinicians may start collecting performance data anytime between January 1, 2017 and October 2, 2017. Note that performance data must be submitted by March 31, 2018 irrespective of the specific starting date. Similar to the Advanced APMs track, the first payment adjustments (which may be increases, decreases or neither) under MIPS will not occur until 2019.
Figure 1 briefly summarizes how practices will receive increases and decreases in Medicare payments during 2019 based on their 2017 participation.
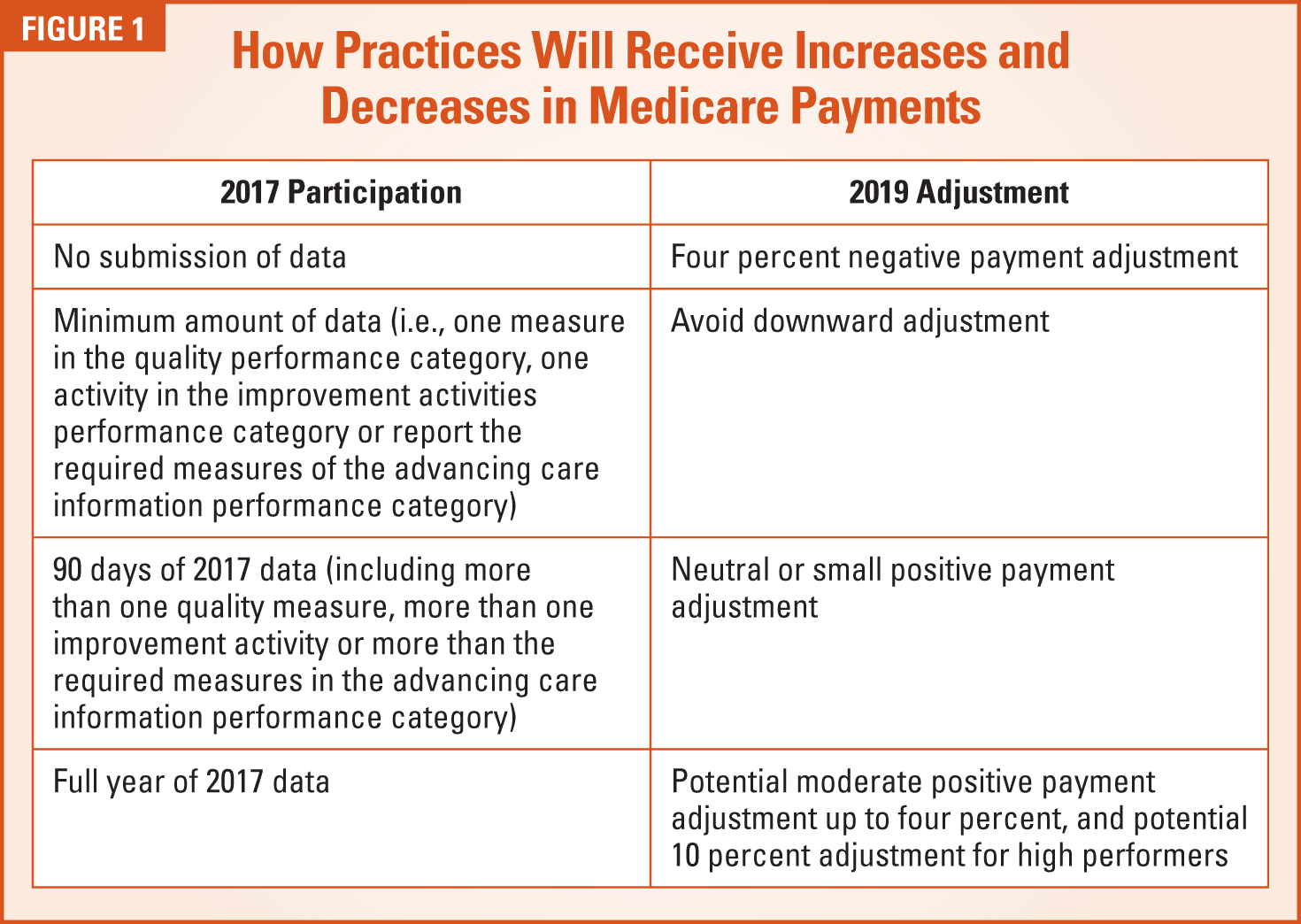
In summary, for clinicians who select MIPS, three levels of reporting will avoid a negative MIPS payment adjustment. Clinicians can avoid a downward adjustment though the submission of a minimal amount of 2017 data (e.g., even one quality measure or improvement activity). Positive adjustments will be based on the actual performance data within the reported information and not on the amount of information submitted or the length of time for which such information is submitted.
For clinicians who submit MIPS data as an individual, the payment adjustment will be based on individual performance. Such individual data for the MIPS categories described above may be submitted through an EHR, registry or Qualified Clinical Data Registry (QCDR). Quality data may also be submitted through the Medicare claims process.
For clinicians who submit MIPS data through a group, the group will receive a single payment adjustment based on the group's performance as a whole. Group-level data may be submitted through the CMS web interface (if the group registers by June 30, 2017) or third-party data submission services (e.g., a certified EHR, registry or QCDR). In future years, the federal government intends to permit clinicians to participate in MIPS through virtual groups and will propose further policies in such regard after soliciting additional input.
Practical Guidance and Next StepsPhysicians and their groups should promptly and proactively develop a strategy to thrive under MACRA and the QPP. If you participate, you need to determine which track is best (i.e., APMs or MIPS) based on your individual circumstances. Such determination should take into account whether your practice already participates in an Advanced APM or whether such participation in the future is desirable. If you select the MIPS track, you will need to decide whether to participate as an individual or a group, the level and timing of participation, and the type of reporting that is practicable.
CMS recommends that physicians take the following steps to prepare for MIPS in 2017:
- Check that your EHR is certified by the Office of the National Coordinator for Health Information Technology. If it is, it should be ready to capture information for the MIPS advancing care information category and certain measures for the quality category.
- Consider using a QCDR or a registry to extract and submit your quality data.
- Use the QPP website to explore the MIPS data your practice can choose to send in. Check to see which measures and activities best fit your practice.

The federal government offers resources to assist small practices through the Transforming Clinical Practice Initiative and through certain small, rural and health professional shortage area exceptions. Additional resources are available through governmental guidance, professional associations, consultants, software, technology and practice management companies, attorneys and others.
Additional QPP resources are available at the following sites:
- https://qpp.cms.gov/
- https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/Value-Based-Programs/MACRA-MIPS-and-APMs/MACRA-MIPS-and-APMs.html.
- www.ama-assn.org/MACRA
- http://www.asahq.org/quality-and-practice-management/macra
- https://innovation.cms.gov/initiatives/Transforming-Clinical-Practices/
Good luck. You can do this.