The Burden of Measuring Quality in Anesthesiology and Other Physician Practices
Donald Berwick, MD, senior fellow at the Institute for Healthcare Improvement (IHI) (and a former CMS administrator) described nine steps to advance healthcare into “the moral era” at an IHI forum in December, 2015. One of those steps was to “stop excessive measurement.” Dr. Berwick said:
I don’t mean that we should stop measuring. Indeed, I celebrate transparency in every form. How else can you learn? But we need to tame measurement. It has gone crazy. Far from showing us our way, these searchlights training on us, they blind us. ... I vote for a 50 percent reduction in all metrics currently being used.
Many anesthesiologists and pain physicians will agree that quality measurement has gone over the edge. The ASA’s Anesthesia Quality Institute (AQI) has adopted 22 measures and has identified 26 official Physician Quality Reporting System (PQRS) measures that can be reported by anesthesiologists and/or pain physicians. In proposing 48 distinct measures to CMS for use in its Qualified Clinical Data Registry (QCDR) in 2016—CMS’s approval is still pending—the AQI was obviously trying to provide an adequate selection for any of its members to be able to report the PQRS-required minimum of nine measures. But choosing the best measures for an individual practice is itself not easy and takes time. To begin with, there is the question of which type of measures the practice should focus on. Does it choose those that are the least demanding to report, or those that are the most meaningful for potential quality improvement?
The fact that the question of ease of reporting vs. worthiness of measures persists is an indication of the immature yet highly complex state of quality measurement. To put it another way, anesthesiologists and other physicians often ask, “How is all this helping patient care?”
In a study published in the March 2016 issue of Health Affairs, US Physician Practices Spend More Than $15.4 Billion Annually To Report Quality Measures, Casalino et al. published the results of a survey of physicians representing four common specialties: internal medicine, family medicine, orthopedics and multispecialty practice. They found that:
- The average physician spends 2.6 hours per week dealing with quality measures and their clinical and administrative staff spends another 12.5 hours per physician per week.
- The combined total of 15.1 hours per week from paragraph 1 amounts to 785.2 physician and staff hours per physician per week.
- The time spent by physicians and staff translates to an average cost of $40,069 per physician per year, or $19,494 in physician time alone. Annualized, the average cost for both physician and staff comes to $15.4 billion for just the four specialties surveyed.
- Of the 394 practices responding to the survey, 81 percent reported that they spent more or much more effort dealing with external quality measures than three years ago.
- Only 27 percent believed that current measures were moderately or very representative of the quality of care.
- Only 28 percent used quality scores as the basis for quality improvement activities.
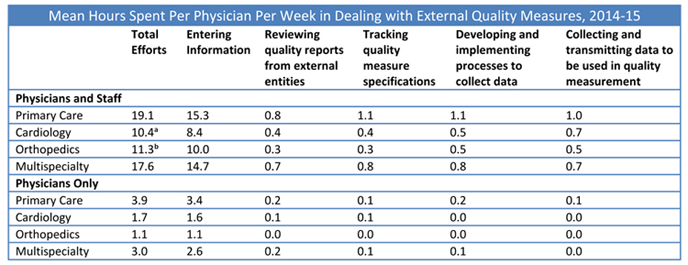
- Data entry is by far the most time-consuming of the five elements surveyed, and the amount of time spent by the physicians in the four specialties varies considerably. The following table appears as Exhibit 6 in the Health Affairs article:
A majority of the respondents wrote comments in the free-text portion of the survey instrument. “Five major themes recurred,” according to the authors: “the burden of current measurement requirements on small practices, recommendations to have measures that are uniform across entities, the need for specialty specific measures, the need for measures that better represent quality, and the need to easily and accurately extract data from electronic health records (EHRs).”
Many anesthesiologists and pain physicians would add a sixth theme: the inability of current quality measures to account for differences among patients, i.e., the lack of adjustment for severity of illness.
The survey conducted by Dr. Casolino and his team was one of the first formal studies of the burden of complying with externally-required quality measurement systems (not that it did not have limitations such as the possible overrepresentation of respondents who were dissatisfied). There has been a good deal of anecdotal criticism of the state of quality measurement in general.
The profusion of measures, questions about their validity and the EHRs that should be facilitating rather than impeding reporting together have contributed perhaps more than any other factors to a 50 percent burnout rate among physicians. (See Wachter RM. How Measurement Fails Doctors and Teachers. New York Times Sunday Review, January 16, 2016.) Casolino noted a “study of twenty-three health insurers [that] found that 546 provider quality measures were used, few of which matched across insurers or with the 1,700 measures used by federal agencies.” Different rules between Medicare, private payers and health systems as to the details required in reporting what is essentially a single measure increase the burden by orders of magnitude.
Fatigue is growing as performance on the various measures becomes increasingly linked to financial rewards and penalties. The PQRS, Value-Based Payment Modifier and the “Meaningful Use” of EHR technology incentive program have become complicated almost beyond comprehension. As we know, they are being phased out—but they will be replaced in 2019, pursuant to the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA), by the Merit-Based Incentive Payment System which will potentially introduce even more measures.
One expert who does not believe that MACRA will introduce a better way of linking measurement of physician performance to the amount of Medicare payments—because the concept of measurement as the best route to improvement is flawed—is Robert Berenson, MD, former chair of the Medicare Payment Advisory Commission (MedPAC) and former acting CMS administrator:
[Dr. Berenson] argues that the Medicare Access and CHIP Reauthorization Act (MACRA), which will steadily increase the amount of Medicare payments to physicians that are based on measures of value, will likely turn out to be “a doomed attempt to measure value.” “Practical challenges aside, pay for performance for health professionals may simply be a bad idea. Behavioral economists find that tangible rewards can undermine motivation for tasks that are intrinsically interesting or rewarding. Furthermore, such rewards have their strongest negative impact when they are perceived as being large, controlling, contingent on very specific task performance, or associated with surveillance, deadlines, or threats …”
(Doherty B. Explaining the Physician Anxiety Behind Performance Measures. KevinMD blog, March 1, 2016.)
Many of our readers would surely agree that pay for performance, the impetus for the explosion of quality measurement systems, “may simply be a bad idea.” Yul Ejnes, MD, a past chair of the American College of Physicians, wrote for the KevinMD blog (Let’s Fix Performance Measurement for Physicians, March 2, 2016):
It was supposed to be that if we provided high-quality care to our patients, the measurements would reflect that. Instead, the mantra is that if we score well on our measures, then that means that we provided high-quality care. In other words, the cart has become the horse. It’s time to fix that.
That is a concise and profound statement of the problem, and it is indeed “time to fix that.”