More Alphabet Soup for Anesthesiologists, CRNAs and AAs—the Medicare QRURs
Next year, all physicians in groups of ten or more eligible professionals (EPs) will be subject to the Medicare Value-Based Payment Modifier (VM). Larger groups with 100 or more EPs are already seeing VM adjustments based on their 2013 performance.
In 2017, the VM will apply to all physicians, whether they are in solo practice or are in a group with two or more EPs. And in 2018, payments to nurse anesthetists and anesthesiologist assistants will also reflect the impact of the VM.
It is time for us to familiarize ourselves with the Physician Feedback Program and the Quality and Resource Use Reports (QRURs) that will let physicians find out how they are doing, in terms of the quality and cost metrics that will determine the VM payment adjustment, and compare themselves to their peers.
VM Recap
As we stated in our November 3, 2014 Alert (What Anesthesiologists Need to Know about the Value-Based Payment Modifier):
The VM, which was mandated by the Affordable Care Act, adjusts payments to physicians, groups of physicians, and other EPs based on the quality and cost of care they furnish to patients enrolled in the traditional Medicare Fee-for-Service program.
EPs practicing high-quality, low-cost care will earn a positive VM, while those whose scores indicate relatively lower quality and higher cost may have a negative VM. Given that the VM program is budget neutral, the amount of the positive modifier is unknown until all groups are scored. After such scoring, the aggregate adjustments applied to the low quality/high cost groups are used to fund the positive adjustment payment to the high quality/low cost groups.
CMS will calculate the VM for each practice. It is derived from a quality composite score and a cost composite score. The quality composite score summarizes the group’s (determined by Tax Identification Number or TIN) performance on quality care for Medicare beneficiaries for as many as six equally weighted quality domains: (1) Clinical Process/Effectiveness, (2) Patient and Family Engagement, (3) Population/Public Health, (4) Patient Safety, (5) Care Coordination, and (6) Efficient Use of Healthcare Resources. Each domain score is based on performance scores for PQRS measures reported, using its associated domain. The cost composite score summarizes a TIN’s performance regarding resource use for its attributed Medicare beneficiaries, across two equally weighted cost domains: Per Capita Costs for All Attributed Beneficiaries and Per Capita Costs for Beneficiaries with Specific Conditions (diabetes, CAD, COPD, and heart failure).
As of yet, there are no cost measures that can be attributed to single-specialty anesthesia groups. A beneficiary (and the beneficiary’s assigned costs) will only be attributed to an anesthesia group if that group provided the majority of the beneficiary’s primary care visits. For groups without cost measure scores, CMS will consider the group’s cost "average" for purposes of the VM adjustments.
CMS is currently applying the VM to groups with 100 or more EPs and will apply the VM to groups of ten or more EPs in 2016, based in part on 2014 PQRS participation in the Physician Quality Reporting System (PQRS). Groups of ten or more EPs that do not avoid the -2.0 percent PQRS penalty in 2014 will automatically also be subject, cumulatively, to the -2.0 percent VM penalty in 2016, applied at the claim level.
Groups that successfully report PQRS measures and thus avoid the 2014 PQRS penalty may receive an upward, neutral, or downward VM payment adjustment based on their quality and cost performance scores, as follows:
Groups of 10-99 EPs will only be subject to an upward or neutral payment adjustment in 2016 based on 2014 performance scores.
Groups of 100 or more EPs will receive an upward, neutral or downward adjustment based on performance scores. Those groups whose performance scores place them in lower quality/higher cost categories will have payment at risk under the VM of up to 2.0 percent.
Further details on the timeline for the phase-in of the VM, which began in 2013 and will be complete in 2018, are available at Timeline to Phase In the Value-Based Payment Modifier.
What Are QRURs?
The QRURs are the other primary component of the Physician Feedback Program, the VM being the first. They contain performance information on the quality and cost measures used to calculate the quality and cost composites of the VM—both individual and comparative. According to CMS, “they help physicians understand their current performance levels and how to use the information provided in the QRURs to improve their performance on quality and cost measures.”
In April 2015, CMS released the 2014 Mid-Year QRURs covering the period July 1, 2013 – June 30, 2014. The Mid-Year QRURs were made available, for informational purposes only, to every group and solo practitioner nationwide who reported at least one quality or cost measure with at least one eligible case during the performance period from January 1, 2014 to December 30, 2014. They contain information on a subset of the measures that will be used to calculate the 2016 Value Modifier.
The 2014 Annual QRURs, for the entire 2014 calendar year, are expected to be released any day. For the first time, CMS will make the Annual QRURs available for everyone, including EPs who will not be subject to the MV in 2016—groups and solo practitioners with non-physician eligible professionals only, as well as groups and solo practitioners that participated in the Shared Savings Program, the Pioneer ACO Model, or the Comprehensive Primary Care initiative in 2014.
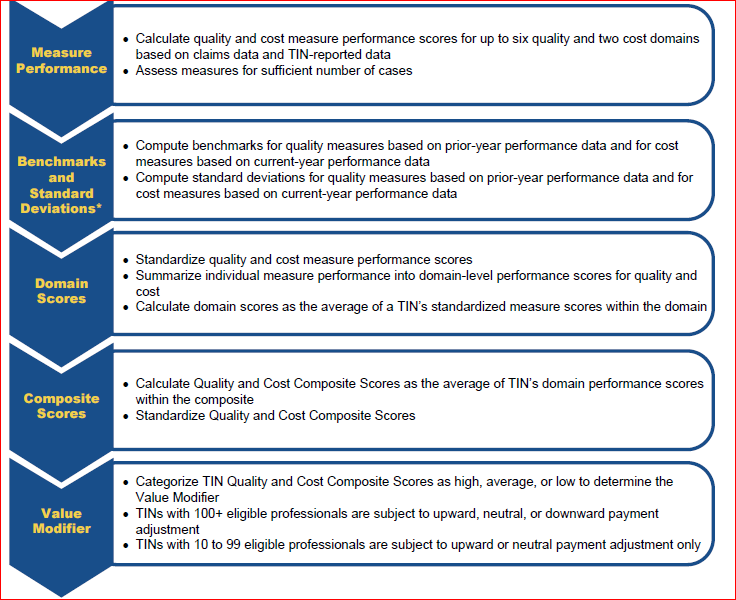
For information on the methodology behind the Annual QRURs, consult the chart below and the 81-page CMS publication in which it appears (https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PhysicianFeedbackProgram/Downloads/2014QRUR-2016VM-DetailedMethodology.pdf)
Methodology for Computing the VM Based on the QRURs
How to Access Your QRUR
You must obtain an Enterprise Identity Management System (EIDM) account in order to access a QRUR. Some readers may remember that they have seen references to “Individuals Authorized Access to CMS Computer Services (IACS)” accounts in connection with checking VM or PQRS reports. CMS discontinued the use of IACS accounts in mid-July and replaced them with EIDM accounts. (If you have an IACS account that you previously used to access QRURs, then follow the instructions for migrating to sign up for an EIDM account.)
You can access QRURs and PQRS Feedback Reports on behalf of a group or solo practitioner at https://portal.cms.gov. QRURs are provided for each Medicare-enrolled Taxpayer Identification Number (TIN). At least one person from your group will need to obtain an EIDM account. Preliminarily, that person must select the correct role:
- On behalf of a group practice (two or more EPs)
- Security Official role, or
- Group Representative role (the difference between the two roles is simply that the Security Official can approve requests for the Group Representative role)
- On behalf of a solo practitioner
- Individual Practitioner role, or
- Individual Practitioner Representative role (again, the Individual Practitioner has the ability to approve requests for the representative role but not vice versa).
Then, once you have an EIDM account with the correct role (for which process more detailed information can be found in CMS’s Guide for Obtaining a New EIDM Account with a ‘Physician Quality and Value Programs’ Role), follow the step-by-step instructions provided in the latest CMS Reference Guide for Accessing the QRURs. At press time, only the Quick Reference Guide for Accessing the 2014 Mid-Year QRURs and Supplementary Exhibits was available. Although the information in the guide for the Annual QRURs will probably be quite similar, certain key information such as the “Calculations related to the VM, including, cost and quality composite scores, quality and cost performance categories (High, Average, Low), and the quality tiering categories” will only appear in the Guide for the Annual QRURs—which CMS is expected to publish shortly. We will notify you once that Guide is available.
Until now, the VM and the QRURs have only affected Medicare payments to large groups of 100 or more EPs. Beginning on January 1, 2016, however, the VM will apply to Fee-For-Service payments for physicians in groups of 10 or more EPs based on performance in 2014.
In the Fall of 2016, for all groups and solo practitioners nationwide, CMS will release QRURs based on quality and cost data from CY 2015. The reports will show the 2017 Value Modifier payment adjustment under the PFS for all physician solo practitioners and physicians in groups with 2 or more EPs. In 2017, all physicians will be subject to the VM, and in 2018, all EPs—including by definition CRNAs and AAs—may also see their Medicare payments adjusted through the VM.
Because of this timeline, we encourage all anesthesia personnel to obtain and understand their QRURs as soon as the 2014 Annual reports are available.