Is it Time to Add TAP Blocks to Your Anesthesia Practice?
First described in 2001, the transverse abdominis plane (TAP) block is a peripheral nerve block designed to anesthetize the nerves supplying the anterior abdominal wall (T6 to L1). In a 2011 meta-analysis, the TAP block was shown to reduce the need for postoperative opioid use, increase the time to first request for further analgesia and provide more effective pain relief, while decreasing opioid-related side effects such as sedation and postoperative nausea and vomiting. Studies included a combination of both general abdominal and gynecologic procedures. The introduction of ultrasound has allowed providers to identify the appropriate tissue plane and perform this block with greater accuracy under direct visualization.
While not all ABC clients use these blocks, a number of practices use them extensively. Prior to 2015, billers typically used the code for peripheral nerve block, 64450, to bill these services. The CPT coding options now include four codes: 64486, 64487, 64488 and 64489. The procedure must be defined as unilateral or bilateral and single shot or continuous. Ultrasonic guidance must be used and is not separately billable.
The introduction of a new code typically represents a careful process of review by AMA CPT editors. It is not uncommon for the process to take years, and many services never receive code designations. The introduction of these new codes raises a number of questions. Since their implementation, how often are they used? What is their clinical efficacy? Is this a modality anesthesia practices should consider implementing? How can you determine the value proposition for the practice and your patients?
A review of a sample of 10 ABC clients indicates that these blocks are not a commonly used procedure. Conversations with clients across the country indicate that many practices have not considered extensive use of these blocks. Invariably, it is the younger physicians fresh from training programs who have the most experience and the best technique.
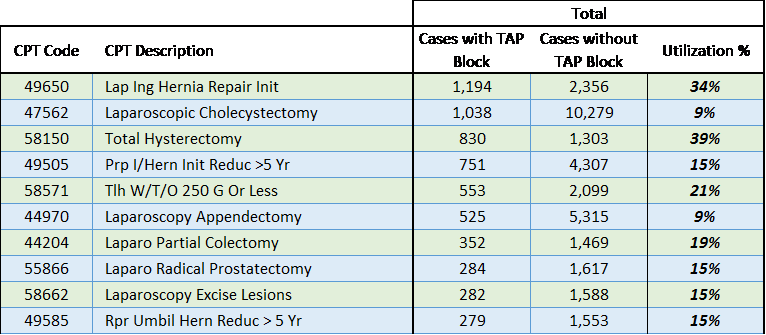
Our analysis of utilization included all blocks billed since the implementation of the new codes in 2015. The first step was to determine what surgical procedures most commonly involved these blocks. Although 450 surgical procedures have been billed with a TAP block, the top 10 are more representative.
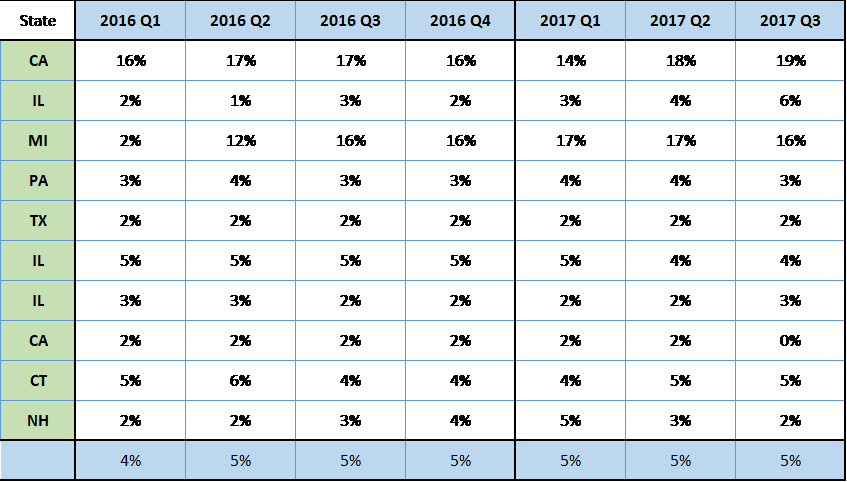
We were also interested in utilization over time. In previous studies looking at the use of interscalene, femoral and sciatic blocks, we have found that once practices analyzed the blocks' clinical efficacy of an enhanced acute pain practice, utilization increased dramatically across the entire ABC client base. This does not appear to be the case for TAP blocks. The table below indicates the percentage of surgical procedures that might include a TAP block that have actually been done with one, by client and quarter since January 2016.
The introduction of a new acute pain management technique involves three considerations: 1) Is this a service that surgeons will find useful? 2) Does the group have sufficiently skilled providers who can provide the blocks regularly? 3) Given the need for skilled providers and the time involved in their administration, would the service represent a value-added opportunity for the practice?
Proponents argue TAP blocks are a very effective adjunct technique for a variety of abdominal procedures and greatly enhance the patient's comfort during recovery. As noted above, a study indicates their use minimizes the need for postoperative opioid management. This modality may not be appropriate for all practices, but the data indicate it may be one that more practices should consider.
It appears that most of today's anesthesiologists did not receive extensive training in these blocks or the opportunity to see the benefits of their utilization. As is true of many new techniques, there are pockets of utilization. The good news is that today's graduates are bringing a variety of new techniques into the field. As has been true of the expansion of acute pain practices, anesthesia groups have a great opportunity to leverage these new graduates' skills and train other group members in these techniques.
The benefit of TAP blocks will vary greatly from practice to practice. Technical experience, clinical demographics and utilization are just a few of the determining factors. If you have questions or would like ABC to provide a comprehensive analysis specific to your practice, please contact your account executive.
We want to hear from you. Do you have a topic you would like to see covered in an ABC eAlert? Send your suggestions to info@anesthesiallc.com.