 When one reviews the Current Procedural Terminology (CPT®) changes for 2015, a recurrent theme throughout is the consolidation of code combinations. The American Medical Association/ Specialty Society Relative Value Update Committee (RUC) identifies codes that are regularly reported together more than 75 percent of the time. The identified codes are then considered by the CPT Editorial Panel for bundling. The CPT Editorial Panel consists of physicians representing all specialties and other stakeholders who are all users of the CPT code set and thus have a practical perspective on the changes presented. It is the intention of the RUC, when presenting these code combinations, to provide the logic, rationale and function of these CPT changes. The following paragraphs will explore the rationale behind the bundled codes that are related to anesthesia and pain management.
Ultrasound is often utilized to improve the accuracy of intra-articular placement of the needle for safety and better...
When one reviews the Current Procedural Terminology (CPT®) changes for 2015, a recurrent theme throughout is the consolidation of code combinations. The American Medical Association/ Specialty Society Relative Value Update Committee (RUC) identifies codes that are regularly reported together more than 75 percent of the time. The identified codes are then considered by the CPT Editorial Panel for bundling. The CPT Editorial Panel consists of physicians representing all specialties and other stakeholders who are all users of the CPT code set and thus have a practical perspective on the changes presented. It is the intention of the RUC, when presenting these code combinations, to provide the logic, rationale and function of these CPT changes. The following paragraphs will explore the rationale behind the bundled codes that are related to anesthesia and pain management.
Ultrasound is often utilized to improve the accuracy of intra-articular placement of the needle for safety and better...  Medscape is one of the very few organizations that surveys physicians on compensation and practice patterns, breaks out the specialty of anesthesiology and publishes the results for free. The Medscape Anesthesiologist Compensation Report also has one of the larger absolute response rates; in the most recent survey, reported in March 2015, 1179 responses were received from anesthesiologists during the period December 30, 2014 – March 11, 2015. For those reasons alone, it behooves anesthesiology practices to be familiar with the Medscape data. The sample is small. It is probably not representative. As science, the survey does not pass muster. But since there is so little information of any better quality available, the Medscape compensation surveys are being used, usually in conjunction with other surveys such as those published (and sold) by the Medical Group Management Association (MGMA) and American Medical Group Association.
The weakness of the information is slightly mitigated by...
Medscape is one of the very few organizations that surveys physicians on compensation and practice patterns, breaks out the specialty of anesthesiology and publishes the results for free. The Medscape Anesthesiologist Compensation Report also has one of the larger absolute response rates; in the most recent survey, reported in March 2015, 1179 responses were received from anesthesiologists during the period December 30, 2014 – March 11, 2015. For those reasons alone, it behooves anesthesiology practices to be familiar with the Medscape data. The sample is small. It is probably not representative. As science, the survey does not pass muster. But since there is so little information of any better quality available, the Medscape compensation surveys are being used, usually in conjunction with other surveys such as those published (and sold) by the Medical Group Management Association (MGMA) and American Medical Group Association.
The weakness of the information is slightly mitigated by... 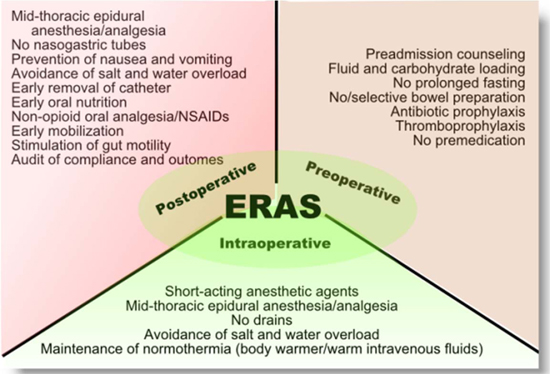 The term “Enhanced Recovery After Surgery” and the acronym ERAS are familiar to most anesthesiologists and to other clinicians. Anesthesia administrators and non-physician advisors may not have encountered the ERAS concept yet. Because of burgeoning interest in better evidence-based perioperative care protocols leading to improved patient outcomes in this era of value-based payment, administrators and practice management staff should acquire a basic understanding of the ERAS concept.
“Enhanced recovery after surgery (ERAS) protocols are multimodal perioperative care pathways designed to achieve early recovery after surgical procedures by maintaining pre-operative organ function and reducing the profound stress response following surgery. The key elements of ERAS protocols include preoperative counselling, optimization of nutrition, standardized analgesic and anesthetic regimens and early mobilization.” (M. Melnyk, RG Casey, P. Black, A.J. Koupparis. Enhanced recovery after surgery (ERAS) protocols: Time to change practice? Can Urol Assoc J. 2011 Oct; 5(5): 342–348). Also referred to as “optimized patient...
The term “Enhanced Recovery After Surgery” and the acronym ERAS are familiar to most anesthesiologists and to other clinicians. Anesthesia administrators and non-physician advisors may not have encountered the ERAS concept yet. Because of burgeoning interest in better evidence-based perioperative care protocols leading to improved patient outcomes in this era of value-based payment, administrators and practice management staff should acquire a basic understanding of the ERAS concept.
“Enhanced recovery after surgery (ERAS) protocols are multimodal perioperative care pathways designed to achieve early recovery after surgical procedures by maintaining pre-operative organ function and reducing the profound stress response following surgery. The key elements of ERAS protocols include preoperative counselling, optimization of nutrition, standardized analgesic and anesthetic regimens and early mobilization.” (M. Melnyk, RG Casey, P. Black, A.J. Koupparis. Enhanced recovery after surgery (ERAS) protocols: Time to change practice? Can Urol Assoc J. 2011 Oct; 5(5): 342–348). Also referred to as “optimized patient...
Anesthesia Business Consultants (ABC) is pleased to announce its latest partnership with the University of California at Irvine (UC Irvine). The anesthesia department at UC Irvine has long been a leader in various projects designed to promote the alignment of Anesthesiologists with their perioperative colleagues; to further the goal of supporting the entire perioperative process. ABC is thrilled to support UC Irvine with their billing operations as well as other programs into the future.“The anesthesia department at University of California, Irvine looks forward to working with Anesthesia Business Consultants. Their approach to comprehensive billing and technology platforms matches our organization's needs and strategic initiatives,” said Dr. Zeev Kain, Chancellor's Professor & Chair of the UC Irvine Department of Anesthesiology and Perioperative Care. “UC Irvine is at the forefront of improving hospital-based care with projects such as the Perioperative Surgical Home (PSH) and quality initiatives and ABC’s commitment to this specialty will...
 The Anesthesia Quality Institute’s Qualified Data Clinical Registry (AQI QCDR) became even more valuable with the recent addition of 16 new measures bringing the total number of measures adopted by the AQI for use in its QCDR to 27. With the nine official Medicare Physician Quality Reporting System (PQRS) measures that can also be reported to the QCDR, the combined total of 36 measures will give most anesthesiologists, nurse anesthetists and anesthesiologist assistants ample opportunity to satisfy the PQRS requirements for 2015. The array of available measures should also provide practices with sound choices for their own quality measurement and improvement programs.
PQRS Reporting via the QCDR
Eligible professionals (EPs) must successfully participate in the PQRS in 2015 in order to avoid a two-percent negative payment adjustment in 2017. Successful participation means reporting on a total of nine measures from three different National Quality Strategy (NQS) domains for at least 50...
The Anesthesia Quality Institute’s Qualified Data Clinical Registry (AQI QCDR) became even more valuable with the recent addition of 16 new measures bringing the total number of measures adopted by the AQI for use in its QCDR to 27. With the nine official Medicare Physician Quality Reporting System (PQRS) measures that can also be reported to the QCDR, the combined total of 36 measures will give most anesthesiologists, nurse anesthetists and anesthesiologist assistants ample opportunity to satisfy the PQRS requirements for 2015. The array of available measures should also provide practices with sound choices for their own quality measurement and improvement programs.
PQRS Reporting via the QCDR
Eligible professionals (EPs) must successfully participate in the PQRS in 2015 in order to avoid a two-percent negative payment adjustment in 2017. Successful participation means reporting on a total of nine measures from three different National Quality Strategy (NQS) domains for at least 50...