March 23, 2015
The Medicare Administrative Contractors are denying claims for anesthesia for colonoscopies submitted with modifier -PT although CMS directed providers to report screening colonoscopies that become diagnostic or therapeutic with that modifier. Pending further clarification from CMS, anesthesia practices can either follow their own MACs’ guidance or hold the affected claims. They should also verify their private payers’ policies as these vary as well.
The New York Attorney General announced, on March 11, 2015, that his office had entered into a settlement agreement with EmblemHealth, Inc., requiring the health plan to cover anesthesiology services provided in connection with an in-network preventive colonoscopy, without any cost-sharing by the patient. The agreement includes a $25,000 penalty and applies not just prospectively but also requires Emblem to send nearly $400,000 of reimbursements to 255 patients who were inappropriately charged co-payments.
The Affordable Care Act (ACA) requires health plans to provide first-dollar coverage for colorectal cancer screening tests and certain other preventive care services, waiving any patient co-insurance, co-payments or deductible amounts. The Emblem agreement expressly extends the requirement to anesthesia for screening colonoscopies: “Because colonoscopies necessitate the administration of anesthesia, anesthesia services provided in connection with preventive colonoscopies should likewise be covered without member cost-sharing.”
In the final Physician Fee Schedule rule for 2015, the Centers for Medicare and Medicaid Services (CMS) explicitly applied the cost-sharing waiver to anesthesia for screening colonoscopies. (See our Alert Medicare Eliminates Patient Cost-Sharing for Anesthesia for Screening Colonoscopies, December 8, 2014.) Pursuant to this decision, Medicare has covered 100 percent of the allowable amount for screening colonoscopies since January 1, 2015. Diagnostic and therapeutic colonoscopies are still subject to co-payments and deductibles, however, and colonoscopies that are intended as purely preventive but during which the endoscopist ends up removing a polyp or tissue for biopsy are in the middle—Medicare now waives the deductible, but the patient is still responsible for the co-payment.
These confusing distinctions are captured through the use of two different modifiers (-33 and -PT) that must be reported on the claim for the anesthesia service, as shown in the following table from our December 8th Alert:
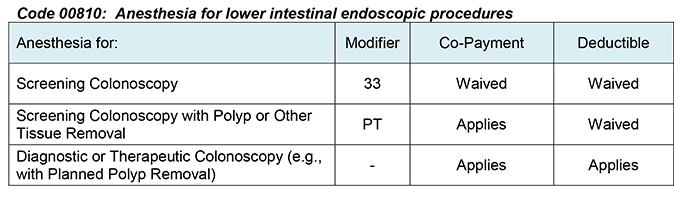
Although CMS described the use of the modifiers as well as their rationale quite clearly in the final rule, stating: “in situations that begin as a colorectal cancer screening test, but for which another service such as colonoscopy with polyp removal is actually furnished, the anesthesia professional should report a PT modifier on the claim line rather than the 33 modifier,” the instructions issued to the Medicare Administrative Contractors (MACs) did not contain the necessary information on modifier -PT. Thus most, if not all, of the MACs have been denying claims for Code 00810 submitted with modifier -PT. Some have reportedly been rejecting the -33 modifier as well, for reasons that cannot be discerned.
The inconsistency between CMS’ stated policy and its mis-application by the MACs is a problem of which ASA is well aware. On February 26, ASA posted a “Washington Alert” on its website notifying members that “ASA has discussed this situation with CMS staff who have informed us that they are aware of this problem and working on [the] best way to address it. ASA will stay in touch with CMS and post information to our website as it becomes available.” Because both the intent and the specific language of the new Medicare policy are clear, we are confident that CMS will correct the erroneous processing by the MACs.
Pending a resolution of the problem at the CMS level, anesthesia practices have two options for reporting screening colonoscopies that end up with polyp or other tissue removal, neither of them entirely satisfactory. They can (1) report the -PT modifier on the claim line, which will most likely result in a denial of the claim, which can then be appealed. When CMS finally straightens out the MACs, the appealed claims should be adjusted. Alternatively (2) anesthesia providers can file their claims for these services without modifier -PT or -33 and collect the deductible amounts from the patients, as various MACs have instructed, but when CMS does act, it will be necessary to recover the deductibles from Medicare and to refund any amounts received from patients other than the co-payments. Fortunately for most anesthesia practices, many Medicare patients will likely have met their deductible—$147 in 2015—in connection with other medical and surgical services obtained early in the year, before they receive and are billed for anesthesia for screening colonoscopies. With the deductibles already satisfied, there will be no need for the anesthesia practice to collect them from the patients whether the MACs accept modifier -PT or not.
Also fortunate is the recent introduction in Congress of the latest version of The Removing Barriers to Colorectal Cancer Screenings Act (S. 624; H.R. 1220), legislation that would eliminate cost-sharing under Medicare for preventive screening colonoscopies, even if a polyp or tissue is removed. If this legislation passes, there will no longer be any reason for CMS to follow different payment rules for the different types of screening colonoscopies through the use of modifiers -33 and -PT (or otherwise).
The situation is also somewhat confused as far as private health plans are concerned. Private health plans are not constrained by the Medicare statute that CMS interpreted to bar waivers of patient deductibles for colonoscopies that turn diagnostic or therapeutic. They vary, however, in whether they recognize modifier -33 for anesthesia for any colonoscopies at all. Typically, Blue Cross Blue Shield plans will cover medically necessary anesthesia services as part of the screening colonoscopy. Blue Cross Blue Shield of Illinois’ FAQs, for example, state that “If a procedure is billed as a screening, colonoscopy benefits will be applied as preventive based on the intent of the test and not on the findings. If a problem is found during the screening and a procedure is performed to address the problem (such as polyp removal), the claim will still be paid as preventive with no cost-sharing—as long as it has been billed with modifier 33.” The FAQs explicitly include anesthesia. In contrast, “United HealthCare states, ‘preventive benefits only apply when the surgeon’s claim is preventive,’ so you may encounter denials if the surgeon neglects to add modifier 33 to the colonoscopy code,” according to an article in Anesthesia & Pain Decisions (Kyles J. Mind your modifiers: Modifier 33 — Add it to screening colonoscopies and watch for denials, March 1, 2015). Anesthesiologists may want to check their own payers’ policies directly.
The principle behind first-dollar coverage of preventive services such as screening colonoscopies should apply, in our opinion, whether or not the procedure reveals an abnormality and tissue is removed for diagnostic or therapeutic purposes. We hope to be able to inform our readers soon that both Medicare and private health coverage reflect the principle properly
With best wishes,
Tony Mira
President and CEO