February 2, 2015
Anesthesiologists and pain physicians continue to have questions about the PQRS measures that they must report. This Alert contains comprehensive lists of measures available for reporting with anesthesia and pain services, along with an up-to date explanation of how many measures must be reported. Carefully matching each individual clinician’s practice to the requirements of the applicable quality measures and the cross-cutting measures will ensure that no one need find themselves subject to the PQRS payment penalty in 2017.
The Physician Quality Reporting System (PQRS) was one of the hottest topics on attendees’ minds at the January 23-25, 2015 ASA Practice Management Conference in Atlanta. There is still a great deal of confusion regarding how anesthesiologists and pain physicians can satisfy the reporting requirements and avoid the penalties. In addition to explanations given at the Conference, the following recent publications clarify those requirements:
- CMS 2015 PQRS Implementation Guide; 2015 PQRS Measure-Applicability Validation (MAV) Process for Claims-Based Reporting of Individual Measures
- ASA 2015 PQRS FAQS, and
- MGMA PQRS/Value-Modifier Survival Guide
As most readers know, eligible professionals (EPs) who do not satisfactorily report PQRS measures in 2015 will see a negative two percent (-2%) payment adjustment—government-speak for “penalty”—on all of their Medicare remittances in 2017. The questions most frequently asked are: what quality measures can anesthesiologists, nurse anesthetists, anesthesiologist assistants and pain physicians report? And how many do they have to report? The information presented in this Alert is limited to claims-based reporting, the method used by the vast majority of our readers. If there is sufficient interest, we will address “traditional” qualified registry, electronic health record, and group practice reporting at a later date. We will be providing detailed information on reporting to a Qualified Clinical Data Registry (QCDR) in a future Alert.
What PQRS Measures Can Anesthesiologists, CRNAs and AAs Report?
PQRS reporting is based on the performance of a medical service or procedure to which a quality measure is associated. It is not based on the EP’s specialty but rather on the particular services that the EP performs, which vary from one EP to another.
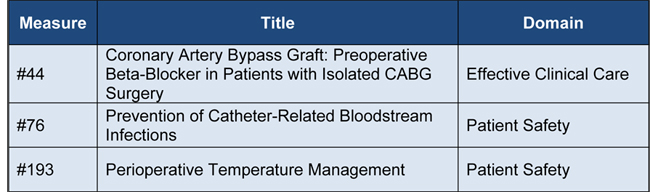
A measure consists of two components, a numerator and a denominator. The numerator describes the specific clinical action required by the measure for performance. The denominator identifies the eligible cases for a measure or the eligible patient population by ICD-9-CM and/or CPT®/HCPCS codes, as well as patient demographics (age, gender, etc.), and place of service (if applicable). There are only two PQRS measures with anesthesia codes in the denominator and one with central venous insertion codes typically reported by anesthesiologists:
Anesthesiologists may report other measures if they perform services identified in the denominators of those measures. The following are the non-anesthesia services that ABC has identified as potentially reportable by anesthesia EPs:

The complete lists of denominator and numerator codes—i.e., the requirements for reporting each measure—can be found in the 2015 Physician Quality Reporting System (PQRS) Measure Specifications Manual for Claims and Registry Reporting of Individual Measures. We emphasize the importance of checking this manual to make sure that all the requirements for the measures selected are performed and documented.
What PQRS Measures Can Pain Physicians Report?
The list of measures that can be reported together with visits provided by pain physicians is more extensive than the anesthesia measures—because none of the measures is specific to pain medicine. Pain specialists work in various settings and will need to choose the measures most appropriate to their practices. There is no single list of PQRS measures that will suit every pain physician. The list below contains measures that ABC has identified as potentially applicable to a typical chronic pain practice:

What about the New Cross-Cutting Measures?
CMS introduced a new component of successful reporting this year. EPs are now required to report a minimum of one (1) cross-cutting measure if they have at least one (1) Medicare patient with a face-to-face encounter. Anesthesia and pain medicine services are considered face-to-face encounters.
There are 19 cross-cutting measures from which to choose. (Some of these can only be reported to a registry.) None of them has an anesthesia code in the denominator, so an EP who only reports anesthesia CPT codes (0XXXX) will not have any cross-cutting measures that apply to his or her practice. An anesthesiologist who performs visit or critical care services listed in the cross-cutting measure denominators should report at least one cross-cutting measure. Measures #1 and #47 both have the following initial inpatient visit codes (99221-99223), subsequent hospital visit codes (99231-99233), critical care code (99291) and outpatient visit codes (99201-99204, 99211-99214) in their denominators. Anesthesiologists who bill for outpatient visits may also be able to report Measures #134 and #326. Something as common as a case cancellation billed to Medicare with code 99233 or another inpatient visit code would call for reporting one of the cross-cutting measures.
A number of cross-cutting measures might apply quite readily to chronic pain practices. These are listed below. There is considerable overlap with the set of pain-practice measures provided above.

Although a discussion of QCDR reporting is deferred to a future Alert, it is important to note here that the cross-cutting measure requirement does not apply to those EPs participating in PQRS via the QCDR reporting mechanism.
How Many Measures Do Anesthesiologists and Pain Specialists Have to Report?
Like other EPs, generally anesthesia professionals and pain physicians must report a minimum of nine (9) measures covering three different National Quality Strategy (NQS) domains for at least 50 percent of the individual EP’s Medicare fee-for-service patients. These numbers apply across all available reporting mechanisms: claims-based, “traditional” qualified registry, electronic health record, group practice reporting option and QCDR.
At least one of the nine (9) measures must be a cross-cutting measure, if any of the 19 cross-cutting measures apply to the EP’s practice.
Measures with a zero-percent performance rate do not count (e.g., the EP reports the measure code but adds the 8P modifier, which indicates “clinical action not performed, no reason specified.”) To illustrate, if an EP places a central venous catheter but is unable to complete “all elements of maximal sterile barrier technique, hand hygiene, skin preparation and, if ultrasound is used, sterile ultrasound techniques followed the steps required for sterile technique” because the case is an emergency or for some other medical reason, he or she should document that reason to avoid defaulting to modifier 8P.
If the EP reports one (1) to eight (8) measures and/or fewer than three (3) domains, for at least 50 percent of patients or encounters eligible for each measure, he or she will be subject to the measure applicability validation (MAV) process by which CMS determines whether additional measures or domains could have and should have been reported. If only one measure is applicable, reporting on that single measure for at least 50 percent of the eligible patients will be sufficient to avoid the payment penalty.
What Makes a Measure Applicable to the EP’s Practice? (MAV)
The MAV process is a two-part test in which CMS examines the totality of claims submitted by the EP to see whether he or she could have reported more measures or domains.
Step 1: Clinical Relation/Domain Test
The clinical relation/domain test is the first step and it is based on two factors:
- How the measure(s) satisfactorily reported currently apply within the EP’s practice, and
- The concept that if one measure in a cluster of measures related to a particular clinical topic or eligible professional service is applicable to an eligible professional’s practice, then other clinically related measures within the clinical cluster may also be applicable. Clinical clusters within MAV are measures that are clinically related based on patient type, procedure, or possible clinical action. With the elimination of the antibiotic prophylaxis measure, the only remaining anesthesia cluster is Number 12:

When reporting Measure #76 alone, it is not subject to MAV. If, however, the EP reports Measure #193, CMS will look at all of his or her claims to see if the EP performed CVC placements and if so whether he or she reported Measure #76 on 50 percent of eligible cases. That brings us to the second step of the MAV process.
If the measure reported appears within a cluster, but the other measures in that cluster cannot be reported because the EP does not perform the denominator services, MAV does not require the other measures. As an example, Measure #131, Pain Assessment and Follow-Up, and Measure #182, Functional Outcome Assessment, appear together in Cluster 13. That cluster applies to chiropractic care and physical/occupational therapy, however. The denominator codes for Measure #182 are limited to 97001, 97002, 97003, 97004, 98940, 98941 and 98942 (PT/OT evaluations and chiropractic manipulations). Thus the pain physician who reports Measure #131 does not need to report the second measure in the cluster.
Step 2: Minimum Threshold Test
The minimum threshold test is based on the concept that during the 2015 PQRS reporting period (January 1, 2015 through December 31, 2015), if an EP treated more than a specific threshold number of Medicare patients meeting the denominator criteria of any of the other measures within the clinical cluster, as determined by CPT or ICD-9 codes, then that EP should have reported those measures. The minimum threshold, with a few exceptions not relevant here, is 15 patients (or encounters) during 2015 for each PQRS measure.
How Many Cross-Cutting Measures Must an EP Report?
EPs with face-to-face encounters must satisfactorily report at least one cross-cutting measure. CMS will analyze claims data to determine if at least 15 cross-cutting measure denominator eligible encounters can be associated with the eligible professional. If it is determined that at least one cross-cutting measure was not reported, the EP with 15 or more visit services with CPT codes in the denominators will automatically be subject to the 2017 PQRS payment adjustment and MAV will not be utilized for that EP. For EPs with no face-to-face encounters, MAV will be utilized for those that report fewer than nine (9) measures and/or fewer than three (3) NQS domains.
If you ONLY report anesthesia CPT codes (0XXXX), there are currently no cross-cutting measures that apply to your practice.
To recapitulate, if an EP only reports anesthesia services, no cross-cutting measures apply to that EP’s practice. If the EP reports the normothermia measure (#193) at least 500 times (and has no more than 1,000 cases in the measure denominator), the catheter-related bloodstream infection prevention measure (#76) 14 times and the beta-blockade measure five (5) times, the EP will avoid the payment penalty as long as he or she does not submit claims for any outpatient visits.
Pain physicians can avoid the MAV review by submitting nine (9) measures across three (3) domains. If they report fewer than nine (9) measures, they will be subject to the MAV process. Since the majority of measures that a pain physician will typically report also appear on the list of cross-cutting measures, it should be easy to satisfy the requirement that at least one (1) of the measures reported be cross-cutting.
As noted above, the cross-cutting measure requirement does not reply to EPs who participate in PQRS by reporting to a QCDR. Neither does the MAV process—successful participation requires no fewer than nine measures. We will explore the QCDR option with our readers soon. Meanwhile, we hope that the information in this Alert is helpful.
Find out more about our anesthesiology billing services.
With best wishes,
Tony Mira
President & CEO