May 29, 2018
The changes in base unit values for anesthesia services for upper and lower endoscopy procedures for 2018, along with the replacement of two endoscopy codes with five more specific codes, were expected to have a negative financial impact on many anesthesia practices. An analysis of data for a representative sample of clients across the country reveals that the impact of these changes has not been as extensive as originally predicted. We review findings related to volume of cases performed, units billed and payer mix.
Each year, the editors of the American Medical Association’s Current Procedural Terminology (CPT) publish a new code book. Most of the time, the new and edited codes have little impact on anesthesia. CPT 2018 was a notable exception.
The new American Society of Anesthesiologists (ASA) codes for endoscopic procedures and the corresponding base values in the ASA Relative Value Guide (RVG) require more specific anesthesia documentation. The new base values will have a meaningful financial impact on every practice that provides anesthesia for endoscopic procedures. The question is how great that impact will be.
The two ASA codes for endoscopic surgery used for many years (00740 for upper GI procedures and 00810 for lower GI procedures, including colonoscopy) were both valued at 5 units. This meant that the average endoscopic case resulted in 7 units (5 base units and 2 time units).
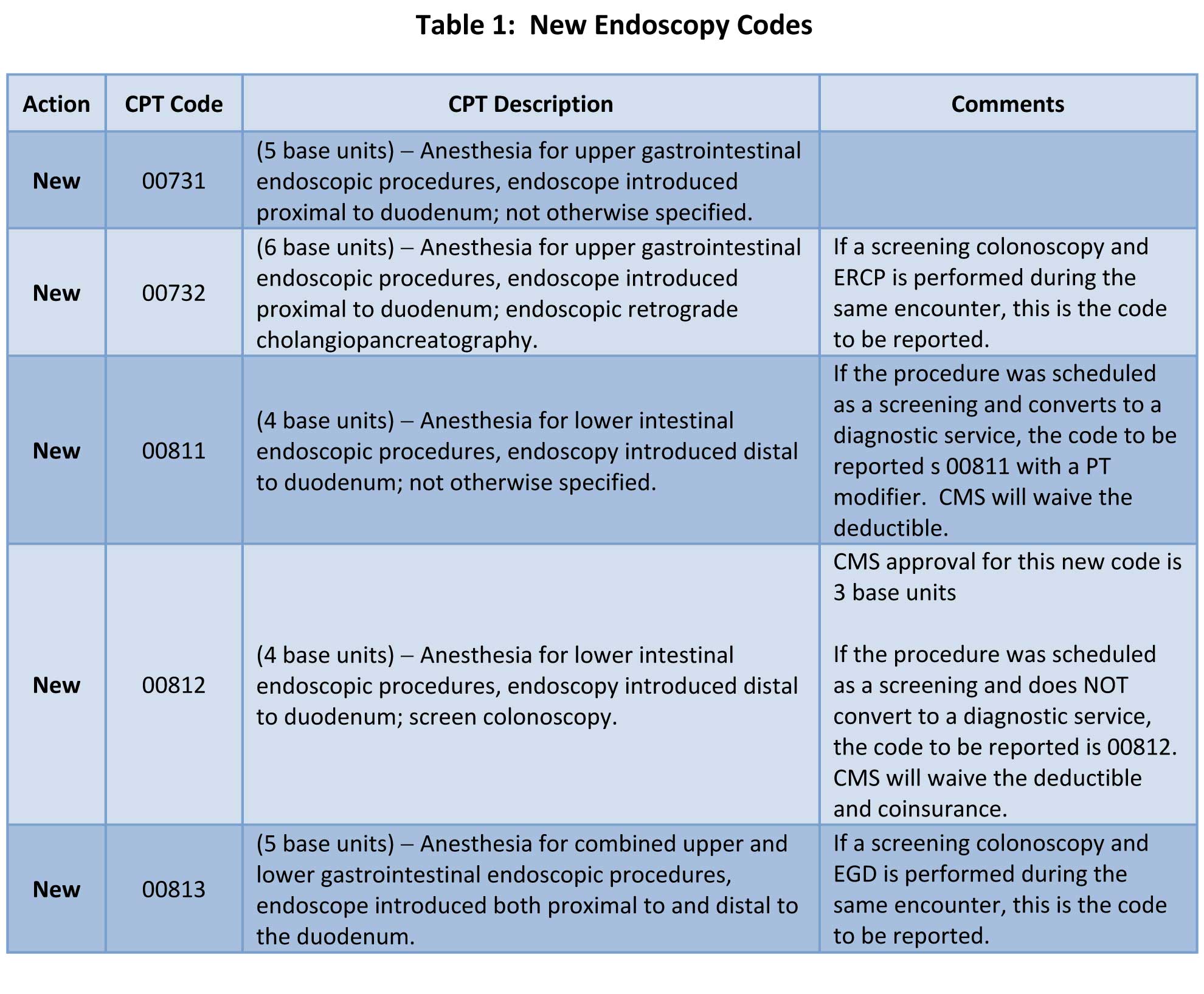
Now there are five codes: two for upper endoscopy (00731 and 00732), two for lower endoscopy (00811 and 00812) and one for procedures involving both upper and lower endoscopy (00813). The base unit value for ERCP increased from 5 to 6 units. The ASA dropped the value of lower GI procedures to 4 units but the Centers for Medicare and Medicaid Services (CMS) dropped the value to 3 units.
Table 1 below summarizes the documentation requirements of each of the new codes:
To assess the potential financial impact of these new codes, we reviewed endoscopic activity for 27 ABC clients across the country, comparing activity from Q1 2017 with that of Q1 2018. All calculations are based on average units per case. (To assess the financial impact on your practice, multiply units by your average net yield per unit. However, keep in mind that these numbers represent the experience of a sample of clients; your experience may not match the reduction in units found among these groups.)
We looked at the data from a variety of perspectives, including overall impact on volume of cases performed, impact on units billed for the service and impact of payer mix, since the value of a Medicare case decreased more than the value of a non-Medicare case.
As shown in Table 2, although there has been a slight overall decrease of 0.65 percent, the total numbers of lower and upper endoscopy cases have remained fairly flat from Q1 2017 to Q1 2018. At the same time, as shown in Table 3, the average number of units billed and the average units billed per case have decreased by 6.7 percent. While this is a sizable drop, it is considerably less than the 10 to 15 percent decrease we had anticipated. Our sense is that these ratios are likely to remain stable for the rest of the year.
Part of this slightly more positive finding can be explained by payer mix. Current guidelines call for an initial screening colonoscopy at age 50. As a result, a sizable proportion of patients undergoing screening colonoscopies are not yet Medicare-eligible and are privately insured. While most anesthesia practices care for an increasing Medicare population, the Medicare population receiving colonoscopies hasn’t grown as fast as the privately insured population. 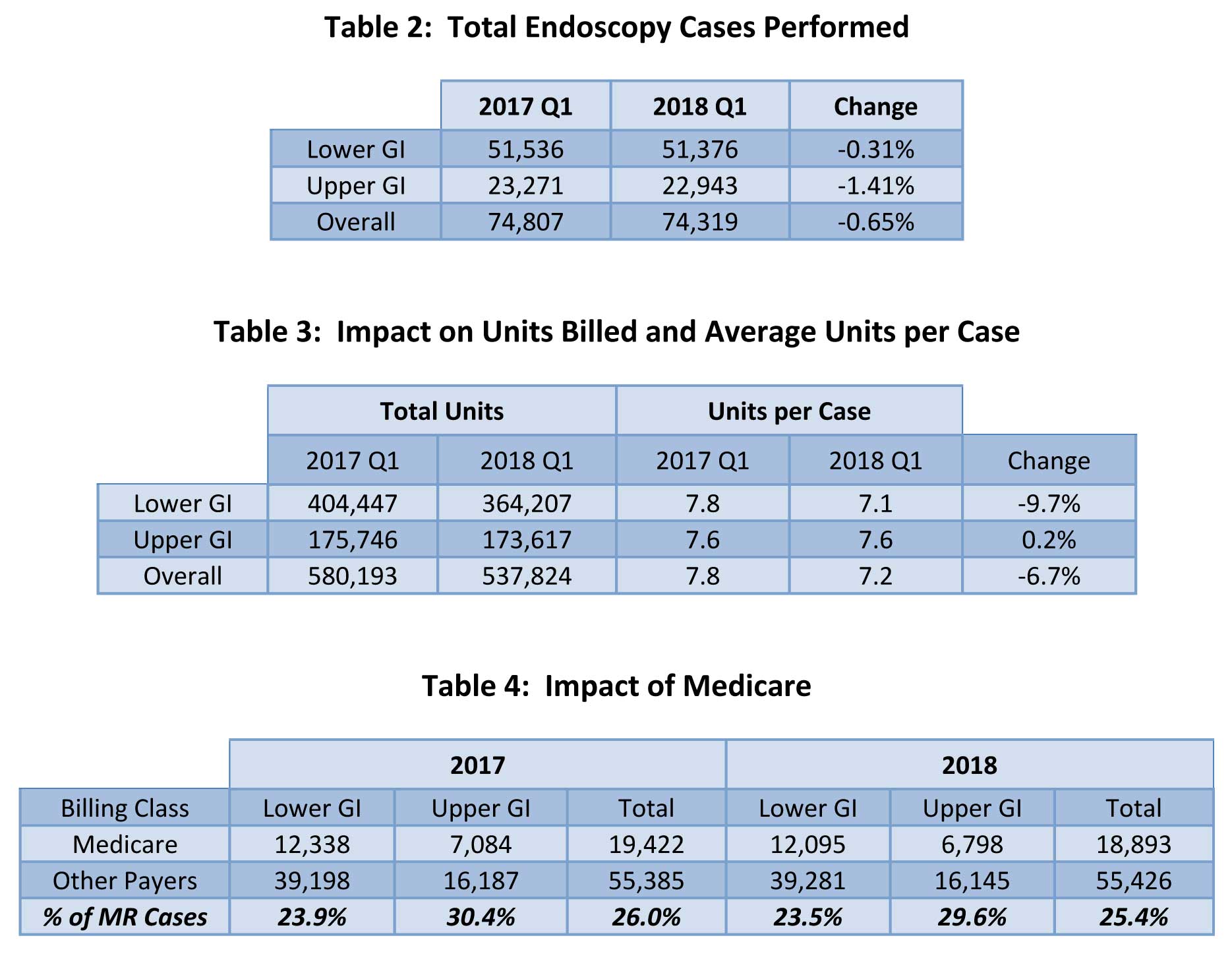
In short, for most anesthesia practices, the actual impact of the new codes is probably somewhat less than initially expected. The drop in unit value starting with 2018 is consistent with a basic and longstanding principle of medical economics: as the supply of a given service increases, the demand drops and inevitably, the price erodes.
These changes signify a tipping point in this line of anesthesia business. The endoscopy wave has crested in most parts of the country. The good news, however, is that virtually all payer policies continue to recognize the value of anesthesia in the safe and efficient provision of endoscopic services. We expect that your practice will be able to count on continued payment in this service line.
If your practice is considering providing services for endoscopy centers, we recommend weighing the potential case rate in deciding whether to sign an agreement. The case volume may be sufficient, but your payment will be lower due to the changes that went into effect in 2018.
We want to hear from you. Do you have a topic you would like to see covered in an ABC eAlert? Please send your suggestions to info@anesthesiallc.com.
With best wishes,
Tony Mira
President and CEO