This tag contains 2 private blog which isn't listed here.
Although the editor, bless her heart, steadfastly refused to let me have a sneak, pre-publication peek at the other articles that appear alongside this one, my educated guess is that each of them purports to give you answers.I know that's why you usually read Communiqué. In fact, nearly every one of the hundreds of other articles that I've written ...
2253 Hits
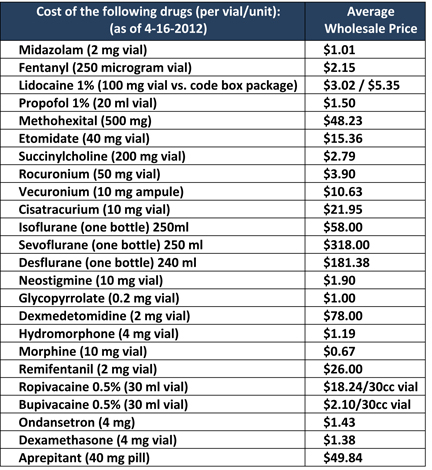 One way in which anesthesiologists can add value to their hospitals’ bottom line is by assuming responsibility for the cost of the drugs they order and administer.
The U.S. general anesthesia market size was approximately $2 billion in 2011 and is expected to grow at a moderate rate of 4% annually from 2011 to 2015, according to a Markets and Markets report. In addition, intravenous anesthetic drugs accounted for the largest share—65%—of the U.S. general anesthetics drugs market in 2011. Individual anesthesiology practitioners and groups have little control over total spending on drugs, just as they have little control over annual national spending on anesthesia services, but they can involve themselves in cost management locally, within their own institutions. As with most activities, success starts with knowledge.
First, anesthesiologists should be aware of the large variation in the cost of anesthetic agents and other medications used during the perioperative process. One...
One way in which anesthesiologists can add value to their hospitals’ bottom line is by assuming responsibility for the cost of the drugs they order and administer.
The U.S. general anesthesia market size was approximately $2 billion in 2011 and is expected to grow at a moderate rate of 4% annually from 2011 to 2015, according to a Markets and Markets report. In addition, intravenous anesthetic drugs accounted for the largest share—65%—of the U.S. general anesthetics drugs market in 2011. Individual anesthesiology practitioners and groups have little control over total spending on drugs, just as they have little control over annual national spending on anesthesia services, but they can involve themselves in cost management locally, within their own institutions. As with most activities, success starts with knowledge.
First, anesthesiologists should be aware of the large variation in the cost of anesthetic agents and other medications used during the perioperative process. One...
26375 Hits
 CMS defines surgical anesthesia time as “the continuous, actual presence of a qualified anesthesia provider. This time begins when the anesthesia provider begins preparing the patient for anesthesia in the operating room or equivalent area. Anesthesia time ends when the anesthesia provider is no longer in personal attendance.” The ASA Relative Value Guide has a similar definition: “anesthesia time begins when the anesthesiologist begins to prepare the patient for anesthesia care in the operating room or in an equivalent area and ends when the patient is safely placed under post-anesthesia supervision.” This is a typical “clear as mud” definition when it comes to anesthesia and CMS. Exactly what is an equivalent area? Is this “equivalent area” ambiguity something we can use to our advantage or is it a disadvantage? Could it be both? It all depends on how or who does the interpretation of the anesthesia record; nevertheless, as long as...
CMS defines surgical anesthesia time as “the continuous, actual presence of a qualified anesthesia provider. This time begins when the anesthesia provider begins preparing the patient for anesthesia in the operating room or equivalent area. Anesthesia time ends when the anesthesia provider is no longer in personal attendance.” The ASA Relative Value Guide has a similar definition: “anesthesia time begins when the anesthesiologist begins to prepare the patient for anesthesia care in the operating room or in an equivalent area and ends when the patient is safely placed under post-anesthesia supervision.” This is a typical “clear as mud” definition when it comes to anesthesia and CMS. Exactly what is an equivalent area? Is this “equivalent area” ambiguity something we can use to our advantage or is it a disadvantage? Could it be both? It all depends on how or who does the interpretation of the anesthesia record; nevertheless, as long as...
4195 Hits
 This post was written by:
Aman Mahajan, MD Chair, Department of Anesthesiology, University of California, Los Angeles, CA
Jody Locke, CPC Vice President of Anesthesia and Pain Management Services, ABC
Background
It is often suggested that an anesthesiology department should have more complete and readily accessible data about the clinical care provided in the operating rooms and the delivery suite than any other department of the facility; but how often is this actually the case? Anesthesia providers review and document enormous amounts of clinical detail and critical events for every patient they see, but little of this information is actually captured in a way that allows for its logical indexing and retrieval. Most anesthesia groups and their billing services have been so focused on the data necessary to calculate a charge and generate a claim that they have virtually ignored what is potentially the most valuable of information of all. The...
This post was written by:
Aman Mahajan, MD Chair, Department of Anesthesiology, University of California, Los Angeles, CA
Jody Locke, CPC Vice President of Anesthesia and Pain Management Services, ABC
Background
It is often suggested that an anesthesiology department should have more complete and readily accessible data about the clinical care provided in the operating rooms and the delivery suite than any other department of the facility; but how often is this actually the case? Anesthesia providers review and document enormous amounts of clinical detail and critical events for every patient they see, but little of this information is actually captured in a way that allows for its logical indexing and retrieval. Most anesthesia groups and their billing services have been so focused on the data necessary to calculate a charge and generate a claim that they have virtually ignored what is potentially the most valuable of information of all. The...
4684 Hits
 “Most people choose unhappiness over uncertainty.” — Timothy Ferris
Anesthesiology groups are facing unprecedented challenges. How will the Affordable Care Act affect them? What will happen when ACOs get up and running? Should our group sell to an investment group? Should we pursue hospital employment?
These are truly uncertain times.
Unfortunately many groups are in a reactive mode, struggling with how to deal with threats and opportunities in the marketplace. This is often because their governance and management processes were formed at a time when there were fewer stressors and challenges. Some group are sprinting towards relationships that appear to offer financial reward and some level of security, but at the same time have the potential to severely limit the group’s and the physician’s autonomy.
While there are situations where employment may be appropriate, many groups that pursue this course are “choosing unhappiness over uncertainty.”
If your group intends to remain...
“Most people choose unhappiness over uncertainty.” — Timothy Ferris
Anesthesiology groups are facing unprecedented challenges. How will the Affordable Care Act affect them? What will happen when ACOs get up and running? Should our group sell to an investment group? Should we pursue hospital employment?
These are truly uncertain times.
Unfortunately many groups are in a reactive mode, struggling with how to deal with threats and opportunities in the marketplace. This is often because their governance and management processes were formed at a time when there were fewer stressors and challenges. Some group are sprinting towards relationships that appear to offer financial reward and some level of security, but at the same time have the potential to severely limit the group’s and the physician’s autonomy.
While there are situations where employment may be appropriate, many groups that pursue this course are “choosing unhappiness over uncertainty.”
If your group intends to remain...
7411 Hits
 The specialty of anesthesiology is experiencing an unprecedented level of merger activity and practice acquisitions. The idea of two or more practices joining forces to secure their market position or enhance their strategic options is hardly a new phenomenon. The past few decades has seen the emergence of some very large anesthesia organizations that have dramatically changed the landscape in their respective markets. Once a pioneer in large group practice management, the Anesthesia Service Management Group (ASMG) and its 150 plus physicians in San Diego has become a model to emulate and refine. By some accounts, we have already reached a point where fewer than 100 organizations employ more than 15 percent of all anesthesia providers, but this is only a rough calculation, made especially challenging by the recent infusion of venture capital money that is inspiring an impressive list of practice acquisitions across the country. This dramatic rethinking of...
The specialty of anesthesiology is experiencing an unprecedented level of merger activity and practice acquisitions. The idea of two or more practices joining forces to secure their market position or enhance their strategic options is hardly a new phenomenon. The past few decades has seen the emergence of some very large anesthesia organizations that have dramatically changed the landscape in their respective markets. Once a pioneer in large group practice management, the Anesthesia Service Management Group (ASMG) and its 150 plus physicians in San Diego has become a model to emulate and refine. By some accounts, we have already reached a point where fewer than 100 organizations employ more than 15 percent of all anesthesia providers, but this is only a rough calculation, made especially challenging by the recent infusion of venture capital money that is inspiring an impressive list of practice acquisitions across the country. This dramatic rethinking of...
4106 Hits
 Anesthesiologists
increasingly point to their role in driving down the rate of surgical
site and other hospital-acquired infections (HAIs). Not only does
anesthesiologists’ and nurse anesthetists’ compliance with the relevant
quality measures help the hospitals’ quality scores and satisfy PQRS
requirements, preventing HAIs is good for patients and saves on health
care system costs.
Compliance with quality
standards and improvement upon current scores are often elements in
negotiations with hospitals, ambulatory surgical centers and, more and
more, third-party payers. When it comes to including performance
bonuses in contracts, the principle is sound, but the dollar value has
been elusive. A new study published in the online edition of JAMA
Internal Medicine on September 2, 2013, Health Care-Associated Infections: A Meta-analysis of Costs and Financial Impact on the US Health Care System
by Zimlichman et al. at the Brigham & Women’s Hospital in Boston,
analyzed the literature and available databases to determine...
Anesthesiologists
increasingly point to their role in driving down the rate of surgical
site and other hospital-acquired infections (HAIs). Not only does
anesthesiologists’ and nurse anesthetists’ compliance with the relevant
quality measures help the hospitals’ quality scores and satisfy PQRS
requirements, preventing HAIs is good for patients and saves on health
care system costs.
Compliance with quality
standards and improvement upon current scores are often elements in
negotiations with hospitals, ambulatory surgical centers and, more and
more, third-party payers. When it comes to including performance
bonuses in contracts, the principle is sound, but the dollar value has
been elusive. A new study published in the online edition of JAMA
Internal Medicine on September 2, 2013, Health Care-Associated Infections: A Meta-analysis of Costs and Financial Impact on the US Health Care System
by Zimlichman et al. at the Brigham & Women’s Hospital in Boston,
analyzed the literature and available databases to determine...
5053 Hits
 On October 1, 2014, the United States health care system will undergo a major transformation. We will transition from the decades-old Ninth Edition of the International Classification of Diseases (ICD-9) set of diagnosis and inpatient procedure codes to the Tenth Edition of those code sets—or ICD-10. The Tenth Edition is the version currently used by most developed countries throughout the world. ICD-10 allows for greater specificity and detail in describing a patient’s diagnosis and in classifying inpatient procedures, so reimbursement can better reflect the intensity of the patient’s condition and diagnostic needs.
This transition will have a major impact on anyone who uses health care information that contains a diagnosis and/or inpatient procedure code, including hospitals, physicians, other providers, payers, clearinghouses, billing companies, etc.
The change will affect all covered entities as defined by the Health Insurance Portability and Accountability Act of 1996 (HIPAA). Covered entities are required to adopt...
On October 1, 2014, the United States health care system will undergo a major transformation. We will transition from the decades-old Ninth Edition of the International Classification of Diseases (ICD-9) set of diagnosis and inpatient procedure codes to the Tenth Edition of those code sets—or ICD-10. The Tenth Edition is the version currently used by most developed countries throughout the world. ICD-10 allows for greater specificity and detail in describing a patient’s diagnosis and in classifying inpatient procedures, so reimbursement can better reflect the intensity of the patient’s condition and diagnostic needs.
This transition will have a major impact on anyone who uses health care information that contains a diagnosis and/or inpatient procedure code, including hospitals, physicians, other providers, payers, clearinghouses, billing companies, etc.
The change will affect all covered entities as defined by the Health Insurance Portability and Accountability Act of 1996 (HIPAA). Covered entities are required to adopt...
4347 Hits
 Bundled payments are
coming. Are there any readers who have not heard? But do we know what
“bundled payments” might mean for anesthesiologists and pain physicians?
Although there are certainly
anesthesiologists participating in bundled payment systems—common
examples include global surgical packages or OB packages—no one has
written a field guide for the specialty. The chapter on bundled payment
for post-acute care strategies in MedPAC’s June 2013 Report to Congress
provides a thorough and up-to-date review of general bundled-payment
design issues. More important, Congress will consider MedPAC’s
recommendations in any new legislation on the topic, much as it did when
it wrote and adopted the Patient Protection and Affordable Care Act of
2010, including a provision requiring Medicare to test a bundled payment
approach.
In a bundled payment
methodology, a single, bundled payment covers all of the services
delivered by two or more providers during a single episode of care or
over...
Bundled payments are
coming. Are there any readers who have not heard? But do we know what
“bundled payments” might mean for anesthesiologists and pain physicians?
Although there are certainly
anesthesiologists participating in bundled payment systems—common
examples include global surgical packages or OB packages—no one has
written a field guide for the specialty. The chapter on bundled payment
for post-acute care strategies in MedPAC’s June 2013 Report to Congress
provides a thorough and up-to-date review of general bundled-payment
design issues. More important, Congress will consider MedPAC’s
recommendations in any new legislation on the topic, much as it did when
it wrote and adopted the Patient Protection and Affordable Care Act of
2010, including a provision requiring Medicare to test a bundled payment
approach.
In a bundled payment
methodology, a single, bundled payment covers all of the services
delivered by two or more providers during a single episode of care or
over...
4601 Hits
 A "bundled" payment covers a
defined package of services delivered by two or more providers during a
single episode of care or over a specific period of time. Nine out of
nineteen provider-payer pairs studied by Bailit Health Purchasing, LLC
have fully operationalized at least one bundled payment. Two more pairs
are conducting observational pilots and three others have embarked on
developing a bundled payment program.
The Healthcare Incentives
Improvement Institute (HCI3) asked Bailit to examine the status of
bundled payments in 2011, and then to update the results this year.
Overall, as reported in HCI3’s Issue Brief “Bundled Payments One Year Later: An Update on the Status of Implementations and Operational Findings—May 30, 2013,”
payer and provider pairs have successfully brought bundled payments
online and are working toward making them a permanent health care
financing change, although challenges remain.
The Issue Brief illustrates
both the achievements and the challenges through...
A "bundled" payment covers a
defined package of services delivered by two or more providers during a
single episode of care or over a specific period of time. Nine out of
nineteen provider-payer pairs studied by Bailit Health Purchasing, LLC
have fully operationalized at least one bundled payment. Two more pairs
are conducting observational pilots and three others have embarked on
developing a bundled payment program.
The Healthcare Incentives
Improvement Institute (HCI3) asked Bailit to examine the status of
bundled payments in 2011, and then to update the results this year.
Overall, as reported in HCI3’s Issue Brief “Bundled Payments One Year Later: An Update on the Status of Implementations and Operational Findings—May 30, 2013,”
payer and provider pairs have successfully brought bundled payments
online and are working toward making them a permanent health care
financing change, although challenges remain.
The Issue Brief illustrates
both the achievements and the challenges through...
4525 Hits
 Recently I had the pleasure of speaking with anesthesia residents and faculty at a well-known progressive academic anesthesiology department. Opportunities like this are among the high points of my professional life because I invariably know more when I leave these presentations than when I arrive. This time was no different.
My recent professional focus has been on working with hospitals and health systems to identify workflow enhancements and quality improvement initiatives to streamline care delivery and deliver greater total value. On a more theoretical level, I have been identifying and developing novel ways to produce comparable or better perioperative medical care in terms of price, quality, and service by using nontraditional processes or clinicians in nontraditional ways. With few exceptions, however, these latter efforts fall mainly into what one would call product development—showing promise but not yet ready for prime time.
The topic, then, for this visit was the role of...
Recently I had the pleasure of speaking with anesthesia residents and faculty at a well-known progressive academic anesthesiology department. Opportunities like this are among the high points of my professional life because I invariably know more when I leave these presentations than when I arrive. This time was no different.
My recent professional focus has been on working with hospitals and health systems to identify workflow enhancements and quality improvement initiatives to streamline care delivery and deliver greater total value. On a more theoretical level, I have been identifying and developing novel ways to produce comparable or better perioperative medical care in terms of price, quality, and service by using nontraditional processes or clinicians in nontraditional ways. With few exceptions, however, these latter efforts fall mainly into what one would call product development—showing promise but not yet ready for prime time.
The topic, then, for this visit was the role of...
5005 Hits
 It is a privilege to bring you another article from Michael R. Hicks, MD, MBA, this time on Successfully Competing in Anesthesia Services Today. Throughout his career as an anesthesiologist and executive, Dr. Hicks has developed unique insights into the qualities that make for success. As a physician, he writes for his peers honestly and without trepidation. Dr. Hicks’s wisdom is among the most valuable information we have published in the Communiqué. In the current issue, he addresses anew the concept of disruptive innovation in anesthesia practice—but as he notes, “successful companies within the anesthesia space are still focused on implementing and executing sustaining innovations” such as quality and process improvement and “better management practices built upon fiscal and behavioral discipline.” The needed innovations will come from five different strategies identified by Dr. Hicks:
Actively manage the performance of the practice and its members, recognizing that neither the group nor...
It is a privilege to bring you another article from Michael R. Hicks, MD, MBA, this time on Successfully Competing in Anesthesia Services Today. Throughout his career as an anesthesiologist and executive, Dr. Hicks has developed unique insights into the qualities that make for success. As a physician, he writes for his peers honestly and without trepidation. Dr. Hicks’s wisdom is among the most valuable information we have published in the Communiqué. In the current issue, he addresses anew the concept of disruptive innovation in anesthesia practice—but as he notes, “successful companies within the anesthesia space are still focused on implementing and executing sustaining innovations” such as quality and process improvement and “better management practices built upon fiscal and behavioral discipline.” The needed innovations will come from five different strategies identified by Dr. Hicks:
Actively manage the performance of the practice and its members, recognizing that neither the group nor...
3957 Hits
In order to be their hospitals’ valued partners, anesthesiologists should understand the needs and forces driving the institutions’ leadership. Some of the strongest of those forces today are creating a wave of merger and acquisition (M&A) activity. In 2012 there were more than 100 deals in the U.S., twice as many as three years earlier. If the relationship dynamics do not encourage partnership between the group and the C-suite, it is nevertheless important to be able to gauge whether one’s hospital is going in the right direction (or staying in the right place).
A recent report from the management consulting firm Strategy&, Succeeding in Hospital and Health Systems M&A: Why So Many Deals Have Failed, and How to Succeed in the Future, is instructive.
In the first of a pair of studies, the authors found that the majority of hospital and health system mergers in the period 1998-2008 had failed to...
4251 Hits
 “The Competition”
These days I hear that term from more and more anesthesia group leaders, and I’m sure that you’re thinking about it more than you’d like.
From the Latin root competitionem, its meaning originated in the sense of rivalry, of a contest for something. Since at least the 1790s, it’s been used to describe rivalry in the marketplace.
Ask yourself what “the competition” means to you. What comes to mind?
In working with anesthesia group leaders across the country, my regular experience is that they envision the competition as another anesthesia group, whether from across the county or across the country. These days, the image that often first comes to mind is that of the predatory staffing-service model.
I certainly can’t fault these group leaders because, especially these days, there is tremendous competitive pressure from outside entities coveting your facility contracts.
So, for most group leaders protecting their practice from...
“The Competition”
These days I hear that term from more and more anesthesia group leaders, and I’m sure that you’re thinking about it more than you’d like.
From the Latin root competitionem, its meaning originated in the sense of rivalry, of a contest for something. Since at least the 1790s, it’s been used to describe rivalry in the marketplace.
Ask yourself what “the competition” means to you. What comes to mind?
In working with anesthesia group leaders across the country, my regular experience is that they envision the competition as another anesthesia group, whether from across the county or across the country. These days, the image that often first comes to mind is that of the predatory staffing-service model.
I certainly can’t fault these group leaders because, especially these days, there is tremendous competitive pressure from outside entities coveting your facility contracts.
So, for most group leaders protecting their practice from...
4291 Hits
 On January 25, 2013, the US Department of Health and Human Services (HHS) Office of Civil Rights (OCR) issued its long-awaited Health Insurance Portability and Accountability Act of 1996 (HIPAA) final omnibus regulations (Final Rule). The Final Rule modified the HIPAA Privacy, Security, Enforcement and Breach Notification Rules (HIPAA Rules) and is comprised of four sub-rules:
Final modifications to the HIPAA Privacy, Security, and Enforcement Rules mandated by the Health Information Technology for Economic and Clinical Health (HITECH) Act;
A final rule adopting changes to the HIPAA Enforcement Rule to incorporate the increased and tiered civil money penalty structure as set forth by HITECH;
A final Breach Notification rule; and
A final rule modifying the Privacy Rule as required by the Genetic Information Nondiscrimination Act (GINA).
While the Final Rule is effective March 26, 2013, compliance with the provisions of the Final Rule is not required until September 23, 2013....
On January 25, 2013, the US Department of Health and Human Services (HHS) Office of Civil Rights (OCR) issued its long-awaited Health Insurance Portability and Accountability Act of 1996 (HIPAA) final omnibus regulations (Final Rule). The Final Rule modified the HIPAA Privacy, Security, Enforcement and Breach Notification Rules (HIPAA Rules) and is comprised of four sub-rules:
Final modifications to the HIPAA Privacy, Security, and Enforcement Rules mandated by the Health Information Technology for Economic and Clinical Health (HITECH) Act;
A final rule adopting changes to the HIPAA Enforcement Rule to incorporate the increased and tiered civil money penalty structure as set forth by HITECH;
A final Breach Notification rule; and
A final rule modifying the Privacy Rule as required by the Genetic Information Nondiscrimination Act (GINA).
While the Final Rule is effective March 26, 2013, compliance with the provisions of the Final Rule is not required until September 23, 2013....
3955 Hits
 What do orthopedic surgery,
cardiology, radiology, gastroenterology and urology have in common?
Compensation in all five specialties is higher, on average, than it is
for anesthesiology, according to Medscape’s Physician Compensation Report: 2013.
Anesthesiology has slipped
from fourth place to sixth place among the most highly-compensated
specialties since last year’s report. Average compensation among
full-time anesthesiologists as reported by Medscape is $317,000—a number
that strikes us as rather low. The explanation may lie partly in the
fact that more respondents reported incomes of less than $200,000 per
year than reported earnings in excess of $500,000. The data apparently
include compensation levels at implausibly low levels ($100,000 or less
reported by 6% of the respondents). The mode is $300,000 to $399,999,
with 18% reporting compensation of $300,000 to $349,999 and 15%
reporting $350,000 to $399,999. Medscape’s Anesthesiologist Compensation Report: 2013.
Medscape defines
compensation in the standard manner: “For employed physicians,
compensation includes...
What do orthopedic surgery,
cardiology, radiology, gastroenterology and urology have in common?
Compensation in all five specialties is higher, on average, than it is
for anesthesiology, according to Medscape’s Physician Compensation Report: 2013.
Anesthesiology has slipped
from fourth place to sixth place among the most highly-compensated
specialties since last year’s report. Average compensation among
full-time anesthesiologists as reported by Medscape is $317,000—a number
that strikes us as rather low. The explanation may lie partly in the
fact that more respondents reported incomes of less than $200,000 per
year than reported earnings in excess of $500,000. The data apparently
include compensation levels at implausibly low levels ($100,000 or less
reported by 6% of the respondents). The mode is $300,000 to $399,999,
with 18% reporting compensation of $300,000 to $349,999 and 15%
reporting $350,000 to $399,999. Medscape’s Anesthesiologist Compensation Report: 2013.
Medscape defines
compensation in the standard manner: “For employed physicians,
compensation includes...
9762 Hits
 The creation of the Medicare/Medicaid Electronic Health Record (EHR) Incentive Program (commonly known as the “Meaningful Use Program”) gave physicians and hospitals a strong incentive to integrate EHRs into their practices. (For more information regarding Meaningful Use, see “Proposed Meaningful Use Stage 2—What it Means to the Anesthesia and Pain Communities” published in the Spring 2012 issue of the Communiqué.) As part of their EHR system, many anesthesiologists have started using mobile devices such as laptops, tablets and smartphones. If used properly, these devices allow access to patients’ EHRs from anywhere that a WiFi connection (or cell phone signal) is available. This often results in quicker responses to questions from patients, families, and other providers. While the use of mobile technology has benefits, anesthesiologists choosing to utilize this technology must pay special attention to making sure they do so in a manner that conforms to their group’s or facility’s security policy...
The creation of the Medicare/Medicaid Electronic Health Record (EHR) Incentive Program (commonly known as the “Meaningful Use Program”) gave physicians and hospitals a strong incentive to integrate EHRs into their practices. (For more information regarding Meaningful Use, see “Proposed Meaningful Use Stage 2—What it Means to the Anesthesia and Pain Communities” published in the Spring 2012 issue of the Communiqué.) As part of their EHR system, many anesthesiologists have started using mobile devices such as laptops, tablets and smartphones. If used properly, these devices allow access to patients’ EHRs from anywhere that a WiFi connection (or cell phone signal) is available. This often results in quicker responses to questions from patients, families, and other providers. While the use of mobile technology has benefits, anesthesiologists choosing to utilize this technology must pay special attention to making sure they do so in a manner that conforms to their group’s or facility’s security policy...
4855 Hits
 Benjamin Franklin said, “An ounce of prevention is worth a pound of cure.” It is certain that Mr. Franklin was not speaking about the value of preemptive compliance work, yet the old adage aptly applies to the work done by physician groups to prevent allegations of fraud or abuse.
The Office of Inspector General for the Department of Health and Human Services (“OIG”) recently reported that the government expected to set a record of $6.9 billion in recoveries from its investigations and enforcement actions for its fiscal year 2012.1 As the chart in Figure 1 shows2, this $6.9 billion is part of a trend of continuously increasing recoveries.
For this reason, many physician groups have implemented compliance programs designed to minimize the chances that the group will commit what the government perceives to be fraud or abuse. One key to effective compliance is an understanding of those issues of particular importance...
Benjamin Franklin said, “An ounce of prevention is worth a pound of cure.” It is certain that Mr. Franklin was not speaking about the value of preemptive compliance work, yet the old adage aptly applies to the work done by physician groups to prevent allegations of fraud or abuse.
The Office of Inspector General for the Department of Health and Human Services (“OIG”) recently reported that the government expected to set a record of $6.9 billion in recoveries from its investigations and enforcement actions for its fiscal year 2012.1 As the chart in Figure 1 shows2, this $6.9 billion is part of a trend of continuously increasing recoveries.
For this reason, many physician groups have implemented compliance programs designed to minimize the chances that the group will commit what the government perceives to be fraud or abuse. One key to effective compliance is an understanding of those issues of particular importance...
9408 Hits
 There is no doubt that the emergence of the Electronic Health Record (EHR) program is changing the way providers capture documentation on the front end. According to the 2012 NCHS Data Brief, 55 percent of physician groups have already adopted an EHR. Among the 45 percent that have yet to implement an EHR system, nearly half plan to purchase or use a system already purchased this year.1 Hospitals are also purchasing and installing EHRs at a rapid rate.
EHR templates are rapidly gaining footholds despite some growing pains. CMS has issued advice on the use of checkboxes and drop-down menus accommodating discrete data capture. Despite access to such “documentation tools” via point-and-click templates, most physicians are complaining that it takes longer to document an encounter in an EHR than to previously dictate it. The RAND Corporation released a paper describing the phenomenon that occurs when an industry’s technological capabilities improve at...
There is no doubt that the emergence of the Electronic Health Record (EHR) program is changing the way providers capture documentation on the front end. According to the 2012 NCHS Data Brief, 55 percent of physician groups have already adopted an EHR. Among the 45 percent that have yet to implement an EHR system, nearly half plan to purchase or use a system already purchased this year.1 Hospitals are also purchasing and installing EHRs at a rapid rate.
EHR templates are rapidly gaining footholds despite some growing pains. CMS has issued advice on the use of checkboxes and drop-down menus accommodating discrete data capture. Despite access to such “documentation tools” via point-and-click templates, most physicians are complaining that it takes longer to document an encounter in an EHR than to previously dictate it. The RAND Corporation released a paper describing the phenomenon that occurs when an industry’s technological capabilities improve at...
16183 Hits
Over the New Year holiday, Congress finally passed legislation to stop the U.S. economy from going over the fiscal cliff. The new law included a temporary reprieve from the 26.5 percent cut provided for by the Medicare Sustainable Growth Rate (SGR) formula. There will be no SGR reduction throughout 2013—a development that lets us all breathe a deep sigh of relief, even though the formula itself, and its future depredations, are still in the law. Medicare payments to physicians and hospitals are not inviolate for the coming year, it must be noted: automatic two-percent reductions will hit Medicare as part of the “sequestration” process just two months from now if Congress and the White House do not reach another deal.
For many anesthesia practices, the runup to negotiations with hospitals and payers is a cliffhanger—indeed, even contemplating future negotiations often feels precarious. Last year, one of the national anesthesia practice management...
3791 Hits